
Abstract
Introduction
Self-reduction of a shoulder dislocation may reduce the time from injury to reduction and to the relief of patient discomfort. The purpose of this study was to assess adherence to earlier acquired self-reduction techniques during real-time recurrent shoulder dislocation.
Methods
A telephone survey was conducted among 58 patients previously taught shoulder self-reduction via an instructional video sent to their smartphones during a visit to the emergency department (ED) for the treatment of anterior shoulder dislocation. Participants were queried on recurrent dislocations, use of self-reduction methods, success rate, the effect that instruction in self-reduction had on their willingness to participate in recreational sports activities, on the decision to avoid surgery, and on the overall level of satisfaction with self-reduction methods.
Results
Forty-five patients (77.6%; average age 31.4±11.7 y, 10 females) were available for follow-up at an average 60.8±11.0 mo after the index visit to the ED. Eighteen of 23 patients (78.2%) who experienced a recurrent dislocation during the follow-up period attempted self-reduction, and 12 of them successfully achieved self-reduction. Sixteen patients (35.6%) reported that the knowledge in self-reduction increased their willingness to participate in recreational sports activities, whereas 4 (8.9%) patients reported that knowledge in self-reduction affected their decision not to undergo surgical stabilization.
Conclusions
Individuals who sustain recurrent shoulder dislocations should be educated on shoulder self-reduction with the aims of minimizing discomfort, obviating referral to the ED, and motivating participation in recreational activities.
Introduction
Glenohumeral joint dislocation is a common musculoskeletal injury encountered in the emergency department (ED), with annual incidence rates estimated to be between 23.9 and 56.3 per 100,000 person-years.1,2 Joint reduction is typically performed by a trained medical professional, often with the aid of intravenous analgesia and sedation.3–5 Increased distance from medical care centers, poor accessibility, and even high caseloads within medical institutions may delay time to shoulder joint reduction.4,6,7 Such delays prolong patient discomfort and are associated with greater risk of nerve injury and higher failure rates of joint reduction on first attempt.8–10
Several self-reduction methods to reduce the time to joint reduction by obviating the referral to a medical center have been described.11–13 The authors earlier reported an overall 41% success rate of 3 self-reduction methods that had been attempted immediately following a brief instructional video sent to the smartphones of 58 patients admitted to the ED for the treatment of anterior shoulder dislocation. 14 This study reports the medium-term follow-up outcomes of that cohort in terms of those patients’ adherence to video-guided self-reduction methods, success rates of those attempts, and patient satisfaction. The secondary purposes were to assess whether education on self-reduction affected participation in usual recreational sports activities and whether it influenced the decision to undergo a surgical stabilizing procedure.
Methods
A telephone survey was conducted among participants in the previously reported cohort. 14 Briefly, 58 participants presenting to an ED with an acute glenohumeral joint dislocation were randomized to 1 of 3 self-reduction techniques: the Boss-Holtzach-Matter technique, the modified Milch technique, and the Stimson technique. Each patient received a link to a short instructional video explaining how to reduce their shoulder dislocation by means of the technique they had been originally assigned. The participants attempted to reduce their shoulder dislocation without further assistance from ED personnel. Reduction attempts were terminated if joint reduction was achieved, if participants requested discontinuing them, or after 20 min had elapsed without success. Patients with failed attempts were treated according to ED protocol for anterior shoulder dislocation. Success rate, time to reduction, pain intensity, satisfaction levels, and complications were recorded.
This retrospective cohort study aimed to assess adherence to self-reduction shoulder dislocation techniques instructed 3–6 y earlier. The first study had been approved by the institutional review board of the medical center, and the participants had signed an informed consent form that included permission to be contacted over the telephone for future follow-up.
The participants in this investigation were contacted through their smartphones and queried about 8 items: 1) the occurrence of a recurrent dislocation since the index visit to the ED, 2) the number of recurrent dislocations since the index visit to the ED, 3) whether self-reduction had been attempted since the index visit to the ED, 4) if the self-reduction was successful, 5) whether the knowledge in self-reduction influenced the willingness to participate in usual recreational sports activities, 6) performance of surgical stabilization since the index visit to the ED, 7) whether the knowledge in self-reduction influenced the decision to forgo a surgical stabilization procedure of the shoulder, and 8) the level of satisfaction with the knowledge in self-reduction of shoulder dislocations.
Initial contact with participants was made through a telephone call by a senior physical therapist who was blinded to the self-reduction method to which each participant had been randomized during the original study. Up to 5 attempts were made to contact each participant through the contact phone number provided during the original study, after which an email message was sent to further pursue the correct telephone contact information.
Statistical Analysis
The collected data were summarized by descriptive statistics with measures of central tendency for continuous variables and frequency counts for categorical variables. χ2 analysis was used to analyze differences in availability for follow-up, rate of recurrence, use of self-reduction techniques, and rate of successful self-reduction attempts among the 3 techniques that had been taught (Boss-Holtzach-Matter technique, modified Milch technique, and Stimson technique). All analyses were performed using IBM SPSS version 29.0 (IBM Corp, Armonk, NY) with an a priori P value of ≤0.05.
Results
Forty-five of the 58 patients (77.6%; average age 31.4±11.7 y, 10 females) recruited for the original study were available for follow-up. The follow-up period ranged from a minimum of 39.8 mo to a maximum of 76.6 mo, with an average follow-up of 60.8±11.0 mo. Seventeen patients (89.5%) from the Boss-Holtzach-Matter subgroup, 17 patients (85%) from the modified Milch subgroup, and 11 patients (57.9%) from the Stimson subgroup provided the follow-up data. Thirteen participants (22.4%) were lost to follow-up.
Table 1 summarizes the responses to the items queried in the survey. Overall, 23 patients (51.1%) reported experiencing at least 1 additional shoulder dislocation since their index visit to the ED (average±SD number of dislocations 1.5±2.4). Eighteen of those reporting a recurrent dislocation (78.2%) had attempted self-reduction, and 12 (66.7%) were successful. To compensate for the loss to follow-up, a worse case analysis was performed as follows: assuming a similar recurrence rate among missing compared with queried patients (51.1%; 7 patients), and assuming that all missing patients had attempted and failed at self-reduction, the overall success rate would have been 48.0% (12/25 patients).
Number (%) with positive and negative responses to each follow-up item.
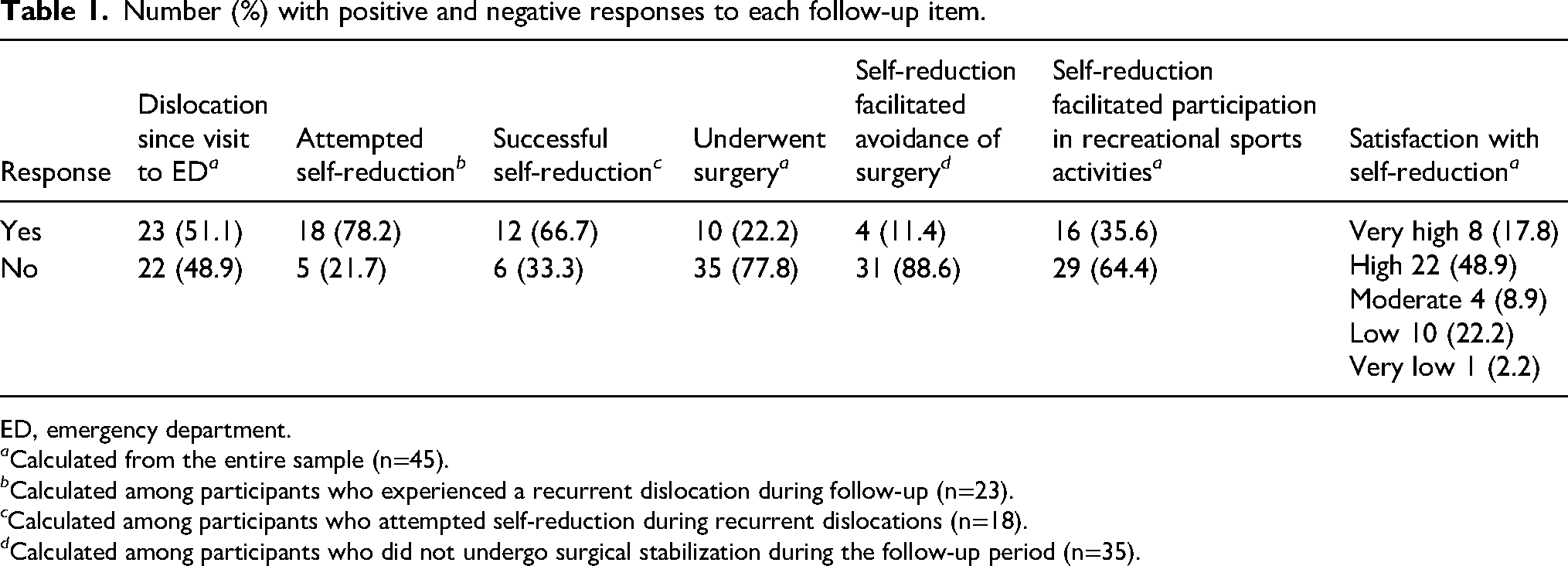
ED, emergency department.
a Calculated from the entire sample (n=45).
b Calculated among participants who experienced a recurrent dislocation during follow-up (n=23).
c Calculated among participants who attempted self-reduction during recurrent dislocations (n=18).
d Calculated among participants who did not undergo surgical stabilization during the follow-up period (n=35).
Table 2 summarizes the data on dislocation recurrences and attempts at self-reduction among the 3 self-reduction techniques: fewer patients from the Stimson subgroup were available for follow-up (Stimson, 11/19 patients; Boss-Holtzach-Matter, 17/19 patients; modified Milch, 17/20 patients; P=0.04). Among patients available for follow-up, there were no differences in the rate of recurrence, rate of attempts at self-reduction, or rate of successful self-reduction.
Number of participants with recurrences, number attempting self-reduction, and number achieving successful self-reduction in each self-reduction technique subgroup.
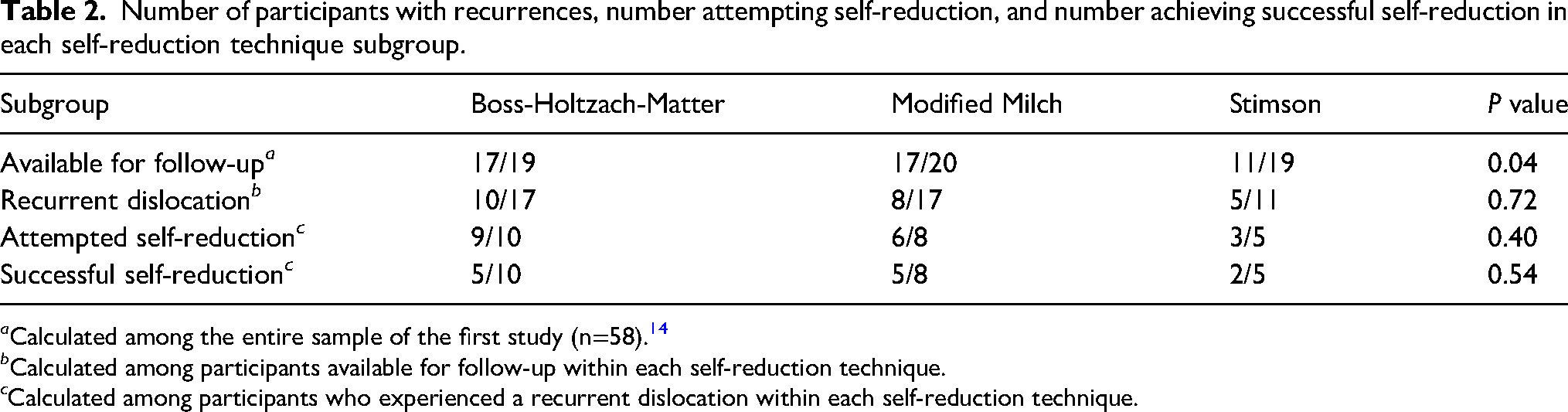
a Calculated among the entire sample of the first study (n=58). 14
b Calculated among participants available for follow-up within each self-reduction technique.
c Calculated among participants who experienced a recurrent dislocation within each self-reduction technique.
Ten patients (22.2%) underwent surgical stabilization during the follow-up period, whereas 4 patients (8.9%) reported that knowledge in self-reduction influenced their decision not to undergo surgical stabilization. Sixteen patients (35.6%) reported that knowledge in self-reduction increased their willingness to participate in their usual recreational sports activities. Patient satisfaction with having learned shoulder self-reduction was high or very high among 30 patients (66.7%) (Table 1).
Discussion
We conducted this medium-term study to determine the influence of our instructional video on the decisions of patients regarding resolution of their recurrent shoulder dislocations. The results of the telephonic survey revealed that most patients (78.2%) attempted to self-reduce their shoulder and that successful self-reduction was achieved by two thirds of those attempting it.
The high compliance rate among our patients (78.2%) suggests that the concept of self-reduction is well accepted by patients with recurrent shoulder instability and that it affords a feasible means of initial self-management that should be recommended by physicians to patients following first-time shoulder dislocation. This excellent compliance rate also supports the role of simple instructional videos in the long-term self-management of patients with musculoskeletal injuries.
The considerable success rate among patients attempting self-reduction in this cohort (66.7%) suggests that education in self-reduction often can shorten the time to reduction and minimize patient discomfort, preclude travel to the ED, and possibly even decrease the risk of secondary nerve injury associated with prolonged tissue deformation. 9 Interestingly, 5 of the patients in this cohort also reported instructing other individuals in self-reducing a dislocated shoulder and that self-reduction was achieved in 4 of them.
Several studies have demonstrated that shoulder self-reduction is possible following a video tutorial 14 as well as under the direct supervision of a trained medical practitioner,11,13,15,16 but only 1 study reported on the follow-up use of previously taught shoulder self-reduction. 17 Marcano-Fernandez et al 17 reported that 9 of 11 patients were able to reduce their dislocated shoulder by applying the Boss-Holtzach-Matter technique over a 1-year follow-up period. The small sample sizes in that study and in our study preclude a meaningful analysis of the difference in success rates between studies, but the positive results observed in both support the generalizability of these findings.
Younger patients following shoulder dislocation are often advised to undergo surgical stabilization to reduce the risk of recurrences.3,18,19 Nevertheless, the percentage of patients who actually pursue surgical intervention for shoulder dislocation has been reported as <20%. 20 This preference toward conservative management is not without a price, however, because patients following first-time shoulder dislocation often exhibit elevated fear of movement, reduced level of activity, and consequently decreased quality of life. 21 Educating patients on shoulder self-reduction may serve to promote greater self-efficacy and confidence in the ability to conservatively manage shoulder instability. It also may help reduce avoidance behavior and improve the quality of life among patients with shoulder instability who opt for conservative management. Accordingly, over one third of the patients in this study indicated that possessing the knowledge of how to perform shoulder self-reduction promoted their greater willingness to participate in their usual recreational sport activities. Four patients also reported that education on self-reduction played a role in their decision to forego surgical intervention.
One consideration pertaining to shoulder self-reduction is the concern of worsening an associated injury such as a greater tuberosity fracture, a rotator cuff tear, or a neurovascular injury. Although shoulder self-reduction is inherently safe due to patient control over the reduction maneuver, it may still be more prudent to await arrival at a medical facility in circumstances involving acute numbness, coldness, or loss of motor function immediately following a shoulder dislocation as well as in any individual over the age of 60 y, in whom these complications are more common. 22
Limitations
This study has several limitations. The sample size was relatively small and lacked the power to determine possible differences in the success rate among the 3 self-reduction techniques. Second, despite considerable effort to contact all the participants of the original cohort, 13 patients (22.4%) were lost to follow-up, more so among those from the Stimson subgroup. This could have affected the between-group comparisons. Finally, the data were obtained via telephone interviews and therefore subjected to recall bias.
Conclusions
In the event of real-time recurrent dislocation, patients who adhere to a previously viewed self-reduction educational video may be able to achieve reduction of a recurrent dislocation independently. Teaching shoulder self-reduction to some individuals who sustain a shoulder dislocation carries the potential to limit discomfort associated with recurrent events, increase self-efficacy, and promote enhanced quality of life.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.