
Abstract
Introduction
The Levantine coast is characterized by environmental and demographic factors—microtidal regime, shifting sandbars, and crowded beaches. These may shape water-sport injury patterns, yet region-specific data are lacking. We described the types, anatomical sites, and sport-specific distribution of injuries along the Levantine coast.
Methods
We conducted a prospective observational study at a single Levantine coastal emergency department. Injuries from surfing, kitesurfing, windsurfing/wing-foiling, swimming/freediving, kayaking, and motorized boards were recorded in real time, including demographics, injury type, body region, and sport.
Results
A total of 62 patients sustained 66 water-sport injuries (mean age 33.7 ± 11.6 years; 77.4% male). Surfing accounted for most injuries (48.5%), followed by kitesurfing (18.2%), swimming/freediving (15.2%), windsurfing/wing-foiling (10.6%), motorized boards (4.5%), and kayaking (3.0%). Open wounds (37.9%) and blunt trauma (36.4%) predominated; upper (34.8%) and lower limbs (28.8%) were most affected. Surfers had more upper-limb lacerations; kitesurfers, lower-limb injuries.
Conclusion
Surfing had the highest absolute injury count. Because participation was not measured, incidence and relative risk across sports are unknown. Local conditions (wave behavior, seabed morphology, and coastal crowding) may influence mechanisms, but whether they raise or lower injury rates versus other regions remains uncertain.
Introduction
The eastern Mediterranean—particularly the Levantine coast—is classified as a microtidal environment, with minimal tidal variation (typically 10-50 cm). 1 Instead of tides, wave activity is primarily wind-driven. 2 Sediment transport in this region is controlled by wind-generated waves and longshore currents acting over gently sloping sandy beaches. These conditions produce highly energetic swash zones—featuring turbulent backwash and foamy uprush—due to rapid wave breaking over shallow, shifting sandbars, resulting in unpredictable “beach break” conditions. 3 These wave dynamics differ markedly from the more dissipative patterns observed on reef-lined or deep ocean coasts.
Aeolian beach ridges along the Levantine coast further reflect active sand transport and beach morphodynamics, contributing to the unstable, ever-changing beach profiles that intensify the mechanical unpredictability of wave breaking, with implications for injury risk in aquatic environments. 4
Despite the dynamic conditions, wave heights in the Levantine sub-basin are moderate, typically remaining well below 1 meter, even during storms. 5 Wave periods average around 6 s, reflecting local wind forcing, in contrast to the 10–20 s periods seen with oceanic swells. This results in short, choppy waves with abrupt energy release near shore. 6 Furthermore, the eastern Mediterranean exhibits offshore, lower variability wind and fewer gust events than the western basin, 7 offering more consistent and predictable conditions for wind-based sports.
Israel's coastline stretches approximately 195 km, with over two-thirds of the population living within 25 km of the shore. 8
This proximity has fostered a vibrant water-sports culture, including surfing, kitesurfing, windsurfing, stand-up paddleboarding (SUP), swimming, and freediving. In recent years, motorized surfboards (eg, JETSURF®) and wing-foiling, which uses a handheld inflatable wing and hydrofoil board, have also gained popularity.
While aquatic sports injuries have been extensively studied in settings dominated by coral reefs, large swells, marine hazards, and expansive surf zones (such as tropical or Pacific coastlines), these contexts do not accurately represent eastern Mediterranean environments. Systematic reviews describe that surfers commonly sustain lacerations—head, face, neck, and lower-limb injuries 9 —while kitesurfers frequently incur lower-limb trauma due to high-impact landings or board collisions. 10 However, no published studies have systematically examined injury patterns across multiple aquatic sports along the Levantine coast.
Accordingly, this study aims to characterize the epidemiology of aquatic sports injuries presenting to the emergency department in a single hospital located near the Mediterranean coast of Israel. By examining injury types, anatomical locations, and sport-specific distributions, we aim to provide regionally relevant insights to support clinical care and injury prevention strategies tailored to this unique environment.
Material and Methods
This was a prospective observational study conducted over a 12-month period from January to December 2023. A prospective design was selected due to the inherent limitations in identifying aquatic sport-related injuries through retrospective database searches. Specifically, such injuries are not assigned a dedicated ICD diagnostic code, and the electronic medical record systems in use do not permit reliable free-text querying of physician notes to capture relevant cases. This study was conducted at a single regional trauma center in the eastern Mediterranean, a public hospital with a multidisciplinary trauma unit co-located with the emergency department. The facility is located approximately 1.5 km from the coastline and serves nearby public beaches and marinas. The emergency department receives both self-presenting patients and emergency medical services (EMS) transports from adjacent coastal municipalities.
To enable systematic case identification, emergency physicians and consultants from multiple disciplines—including emergency medicine, orthopedic surgery, general surgery, pediatrics, and ophthalmology—were requested to report any patient presenting to the emergency department with an injury related to aquatic sports. Upon notification and after patients’ informed consent was obtained, the principal investigator prospectively collected data for each case using a standardized form. The recorded variables included demographic data (age and sex), type of sport involved, anatomical region of injury, and injury type.
In order to facilitate statistical analysis and address the low frequency of cases in certain sport categories, several activity types were aggregated into broader groups based on biomechanical similarity and exposure profile. Specifically, windsurfing and wing-foiling were merged due to shared wind-powered mechanics and similar rider stance and movement patterns. Swimming and freediving were categorized together as immersion-based activities performed without boards or significant impact equipment. Kayaking and stand-up paddleboarding (SUP) were grouped together due to their shared paddling mechanics and reliance on self-generated motion rather than wind or waves.
The study was approved by the Institutional Review Board, and verbal informed consent was obtained from all participants in accordance, before data collection.
All data were anonymized prior to analysis and stored in a secure, encrypted database. No identifiable patient information was collected or retained.
Due to the exploratory nature of the study and the limited sample size within certain sport categories, only descriptive statistics were used. Categorical variables are presented as frequencies and percentages, and continuous variables as means with standard deviations.
Results
A total of 62 patients presented with 66 water-sports-related injuries. The mean age was 33.7 ± 11.6 years. The majority of patients were male (77.4%, n = 48), while 22.6% (n = 14) were female. The most frequently practiced sport was surfing, accounting for 43 injuries (65.2%). Kitesurfing comprised 9 injuries (13.6%), followed by swimming and freediving together with 6 injuries (9.1%), windsurfing and wing-foiling with 4 injuries (6.1%), motorized board with 2 injuries (3.0%), and kayak with 2 injuries (3.0%). No SUP injuries were reported. A detailed distribution of all disciplines is presented in Figure 1.
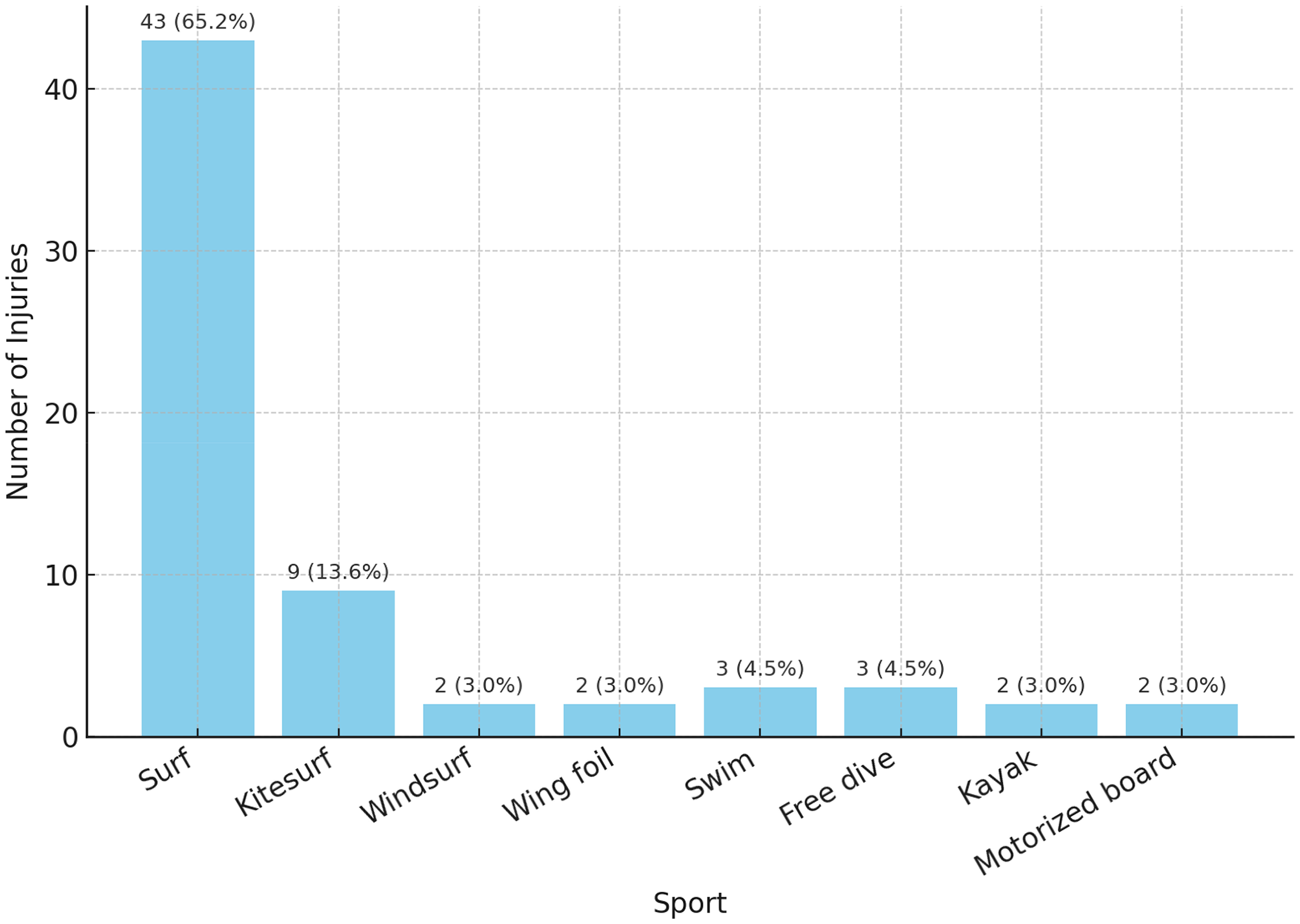
Distribution of injuries by water-sport discipline.
The most reported injury type was blunt trauma, observed in 26 cases (39.4%), followed closely by lacerations or open wounds in 25 cases (37.9%). Fractures were documented in 7 cases (10.6%), joint dislocations in 5 cases (7.6%), and deep soft tissue injuries involving tendons, ligaments, or muscles in 3 cases (4.5%).
In terms of anatomical distribution, upper-limb injuries were most frequent, affecting 22 cases (33.3%), followed by lower-limb injuries in 15 cases (22.7%). Head and neck injuries accounted for 14 cases (21.2%), and facial or ocular trauma was recorded in 8 cases (12.1%). Injuries involving the thorax and abdomen were reported in 4 cases (6.1%), while back injuries occurred in 3 cases (4.5%), making these the least commonly affected regions.
Analysis of sport-specific injury patterns revealed that surfing most commonly involved the upper limb (34.9%) and was associated with both open wounds (37.2%) and blunt trauma (32.6%), with fractures occurring in 14.0% of cases. Kitesurfing injuries were mostly to the lower limb (44.4%), with a relatively even distribution of injury types, and a single fracture was noted. Swimming and freediving injuries were mainly localized to the head (50.0%) and lower limbs (33.3%), predominantly involving blunt trauma and soft tissue injury. Windsurfing and wing-foiling resulted in a small number of injuries, mostly head and lower-limb related, with no fractures. Motorized board injuries included 1 case of blunt trauma to the head and 1 upper-limb fracture. Kayak injuries involved an upper-limb laceration and one facial injury. The complete distribution of injuries across different sports disciplines is shown in Tables 1 and 2.
Injury Type by Sport Discipline.
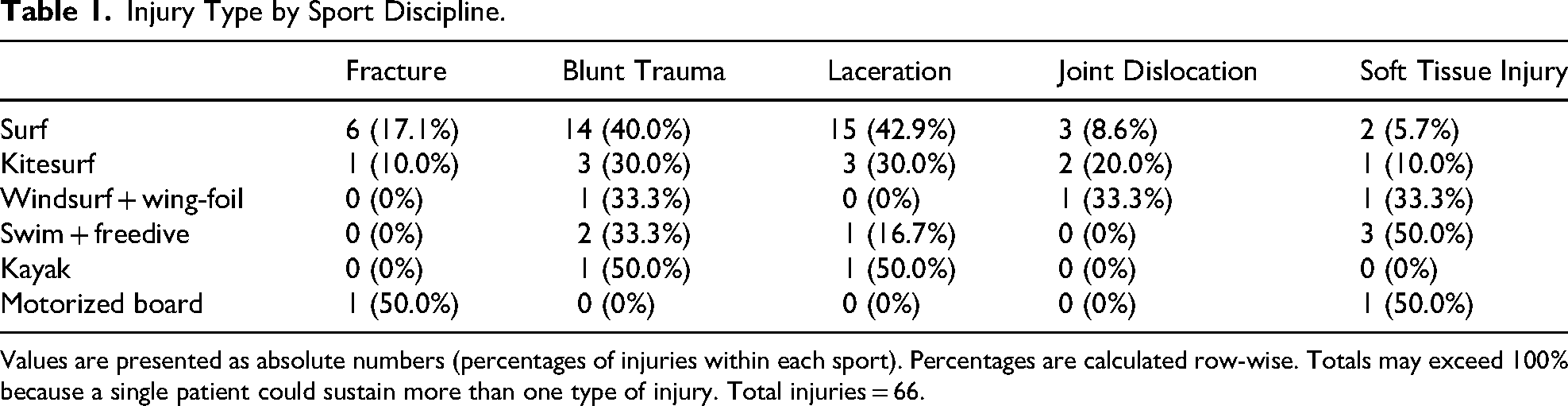
Values are presented as absolute numbers (percentages of injuries within each sport). Percentages are calculated row-wise. Totals may exceed 100% because a single patient could sustain more than one type of injury. Total injuries = 66.
Anatomical Location of Injury by Sport Discipline.
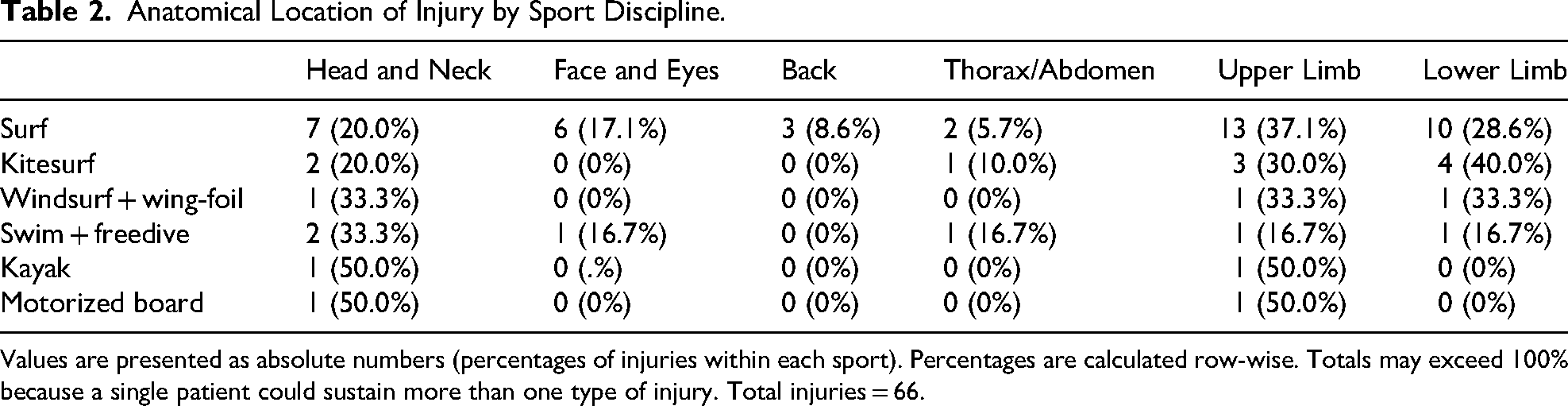
Values are presented as absolute numbers (percentages of injuries within each sport). Percentages are calculated row-wise. Totals may exceed 100% because a single patient could sustain more than one type of injury. Total injuries = 66.
Gender-based differences in injury patterns were modest. Females had a slightly higher proportion of deep soft tissue injuries (14.3% in females vs 2.1% in males), while fractures and dislocations occurred only among males. The distribution of blunt trauma and lacerations was otherwise similar between genders.
Discussion
This study provides the first single-center descriptive overview of water-sports injuries across multiple disciplines along the eastern Mediterranean, with a focus on the unique geographic and environmental context of Israel's Levantine coast.
The distinctive coastal ecology of the Levantine shoreline likely modifies injury distribution beyond sport-specific mechanics. Unlike reef-based or large-swell environments where injuries are often related to seabed impact or high-velocity wave energy, the Levantine coast produces frequent shallow beach-break waves over shifting sandbars. These abrupt breaking patterns promote upper-limb lacerations and blunt trauma in surfers, while the crowded recreational zones amplify the risk of inter-user collisions and board strikes. Thus, environmental context—not only sport mechanics—contributes to the injury spectrum observed in our cohort.
Israel's beaches are subject to exceptionally high-population pressure, with approximately 60% of the national population living within the narrow coastal strip. Due to the concentration of ports, military bases, and industrial facilities, only about 130 kilometers of the 195-kilometer coastline remain accessible for public recreation. 8 As a result, recreational zones are often densely crowded, which may contribute to injury risk by limiting maneuvering space and increasing the likelihood of user collisions. However, our data do not directly quantify overcrowding as a risk factor, so this interpretation should be considered speculative. Long-term wave data from the Levantine Sea indicate that significant wave heights during normal conditions range from 0.4 to 0.8 meter. 5 Unlike oceanic environments where wave height is a dominant risk factor, 11 in the Levantine coast the primary hazards stem from wave velocity, abrupt breaking over shallow sandbars, and highly energetic swash zones. These beach-break conditions amplify the risk of sudden board-to-body impacts, collisions, and falls. Taken together, these beach-break dynamics and coastal use density may skew injuries toward board-to-body impacts and user collisions in surfers and toward lower-limb trauma in kitesurfers; however, we did not measure incidence, so any effect on absolute risk remains uncertain.
Wing-foiling was associated with one reported injury—a lower-limb open wound. Due to its recent introduction and low numbers in our sample, no conclusions can be drawn.
Overall, our findings partially align with the existing literature but also diverge in key aspects. Injury patterns in aquatic sports appear to be influenced not only by sport-specific mechanics but also by regional environmental conditions, such as wave type, seabed structure, wind stability, and population density. Future studies should consider these factors when developing localized injury prevention strategies.
This study has several limitations. First, data collection relied on real-time clinician reporting, which likely led to underreporting of injuries—especially when cases were not referred or missed during busy emergency department hours. Second, the study was conducted at a single center, which limits the generalizability of the findings to other regions or countries. Third, the number of individuals participating in each sport remains unknown, preventing accurate injury incidence or prevalence estimation. Finally, a larger, multicenter study with access to coded databases and retrospective methods is needed to capture a broader, more representative injury spectrum over time.
Conclusion
This study offers the first comprehensive assessment of water-sports injuries along the eastern Mediterranean, highlighting distinct sport-specific injury patterns within the unique environmental and demographic context of the Levantine coastline. Surfing accounted for the highest number of injuries, likely due to both high participation rates and hazardous beach-break conditions. Kitesurfing and motorized board sports demonstrated a predilection for high-energy, lower-limb trauma, while swimming, freediving, and paddling activities were associated with milder upper-limb injuries. These patterns likely reflect a combination of sport mechanics and regional factors such as wave behavior and beach morphology. However, without incidence or prevalence data, the extent to which these coastal conditions increase or decrease overall injury risk remains uncertain. A better understanding of these local dynamics can inform targeted preventive strategies and clinical awareness. Future multicenter studies with broader surveillance are essential to validate these findings and guide injury mitigation in coastal recreational settings.
Footnotes
Ethical Considerations
This study was approved by the institutional ethics board.
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of Data
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.