
Abstract
We present a case of a 32-y-old male professional surfer who sustained an isolated pelvic ring fracture after wiping out on a large wave and striking the ocean floor during a world championship tour surfing competition in Hawaii. The surfer was rescued by the water patrol lifeguards, evaluated by onsite medical staff, and stabilized for transfer and subsequent surgical management. As surfing and surfing competitions become increasingly popular, medical staff and event organizers must be aware of the possibility for severe, life-threatening injuries during surfing events. Although infrequent, staff must be prepared to manage these injuries, including immediate resuscitation, stabilization, analgesia, and transfer to definitive care. We hope this case encourages not only surf event organizers and medical staff, but also staff of all professional and recreational water sports, to increase their preparedness to stabilize and treat both life-threatening and minor injuries. Expeditious and appropriate treatment of an injured athlete has the potential to decrease morbidity and mortality while maximizing the athletes’ functional outcome after injury.
Introduction
Recent research has demonstrated that surfing is a relatively safe sport. The injury rate in competitive surfing is 6.6 injuries per 1000 h of activity. This rate is lower than that in professional rugby, college football, men’s college soccer, and men’s college basketball.1,2 Surfing injuries are generally limited to lacerations, sprains, and strains. 3 However, professional surfers are increasingly judged on their ability to execute the most technically challenging maneuvers in precise locations on the largest and steepest waves. This has resulted in the rapid progression of the sport and increased the physiologic and competitive demands on professional surfers. 4 As such, professional surfers, more than ever before, are subjected to increasing risks of injury from the weight and pressure generated by larger and more powerful waves. Furthermore, they are subjected to increased risk of injury from encountering an unforgiving seafloor after performing increasingly risky aerial maneuvers. 5 Despite this change in performance and judging standards, there is a paucity of reports in the literature that demonstrate the potential for surfing to cause high-energy, life-threatening injuries during recreational or professional surfing events.
Here, we present a case of a professional surfer who sustained an isolated acute pelvic ring fracture after striking the seafloor during a professional surfing event. We hope this case increases awareness among medical and prehospital staff at competitive surfing competitions and similar water sport events of the potential for rare but life-threatening injuries. Emergency plans should be in place well in advance of a contest to rescue participants from immediate hazards, resuscitate and stabilize both minor and major injuries, and provide rapid transport to definitive care.
This case report involves a 32-y-old male professional surfer who experienced severe pelvic pain and left leg numbness after falling on a large wave during a professional surfing competition. He was initially extracted from the surf by water patrol and evaluated on site by an emergency medicine physician, family medicine physician, and orthopedic surgeon, who immediately suspected a pelvic fracture. Emergency medical services provided transport to a level 1 trauma center for imaging and definitive surgical care. After operative fixation and physical therapy and rehabilitation, this individual had an excellent outcome. Twelve months after injury, the patient had minimal long-term sequelae from his injury and returned to competition as a professional surfer. This case highlights the fact that a multidisciplinary and connected team of professionals is required to achieve the best possible outcome for both professional and amateur athletes who experience an injury.
Patient Case Presentation
A healthy 32-y-old male professional surfer with no medical history was competing at a surfing break known as the Banzai Pipeline, a famous surfing locale known for large and powerful waves that break in shallow water over sharp and cavernous reefs (Figure 1). This surf break has claimed the lives of numerous surfers, including professional surfers. Banzai Pipeline is a beach on the North Shore of Oahu that has a unique, powerful, barreling wave that can be treacherous due to its direct exposure to large swells during the winter months and very shallow ocean floor. As the swell energy approaches the beach, the resultant wave comes into contact with the reef shelf, which rises sharply from the volcanic ocean floor (Figure 2).

Photograph illustrating the Pipeline surf break. The powerful waves break over a shallow volcanic reef, which gives this surf break the reputation of being one of the deadliest in the world. Photo courtesy of Sean Davey.

Photograph illustrating the Pipeline surf break, with waves breaking close to shore. Photo courtesy of Sean Davey.
During the competition, the surfer attempted to take off on a wave but wiped out while riding down the approximately 4.5 m wave face. The surfer reported being sucked over the crashing lip and slammed onto the shallow reef. In his own words: “I was sucked over the falls and pole driven into the reef. I thought I was going to be a paraplegic. When I hit the bottom, it felt like I didn’t even hit the water, [the wave] had sucked out that much. I imagine that part of the reef would normally be about 3 ft [0.9 m] deep. I was quite calm under water, but I felt the break happen in my pelvis as the waves were relentless in driving me into the reef.”
He denied striking his head or losing consciousness. After striking the reef, he experienced severe pain and left leg numbness. Unable to swim to shore on his own, he waved for help. Water patrol was stationed in the channel, away from the breaking waves, and retrieved the injured surfer from the water in about 30 to 60 s. The patient was placed on a backboard upon reaching the shore, carried up to the medical tent, and immediately evaluated by 3 physicians. He described his pelvic pain as severe, worse on the left than on the right, and feeling like an intense pressure. On examination, gentle anterior to posterior pressure revealed gross instability in the pelvis. There was exquisite tenderness at the left sacroiliac joint and pubic symphysis. Gross motor and sensory function were intact. A pelvic binder was placed given the concern for internal hemorrhage. Emergency medical services were immediately activated by the contest physicians. Although the closest ambulance was in a nearby town, there was a significant delay in their arrival due to event traffic. Eventually, the patient was transported to the nearest level 1 trauma center in Honolulu, 56 km away.
Upon arrival at the trauma center, his clinical presentation and physical examination were suggestive of multiple pelvic fractures with disruption of the pelvic ring. His vitals upon arrival were as follows: blood pressure was 135/76 mm Hg, heart rate was 71 beats·min-1, respiratory rate was 17 breaths·min-1, and temperature was 36.5°C. He was alert and awake with a Glasgow Coma Score of 15 and could move all extremities spontaneously. Cardiac, pulmonary, and abdominal examinations were normal. All 4 extremities were warm and well perfused. He reported no recent illness, fever, chills, nausea, vomiting, diarrhea, or weakness.
Laboratory workup showed an elevated white blood cell count at 11.9 cells·uL-1. Hemoglobin and hematocrit were borderline low at 13.3 g·dL-1 and 38%, respectively. Platelet count was also reduced at 131,000 uL-1. Prothrombin time was 14.9 s, partial thromboplastin time was 24.8 s, and international normalized ratio was 1.2. His basic metabolic panel was normal.
Chest radiograph was normal. Pelvis radiograph showed displacement of the pubic symphysis with probable acute fractures (Figure 3). Computed tomography of the abdomen and pelvis with and without contrast showed a fracture of the left sacral ala with involvement of the left sacral body. The sacral body was angulated with comminuted and displaced fragments likely arising from the anterior left sacral ala. The fracture also involved S1 and mild buckling and angulation of the S2 sacral cortex. Sheer injury was also present with a mild vertical offset of the pubic symphysis without significant widening. There was presence of extraperitoneal and presacral pelvic hematomas without solid organ injury or intraperitoneal fluid (Figure 4). The imaging studies were consistent with a Young and Burgess Anterior Posterior Compression III type of pelvic fracture, with a probable vertical shear component.
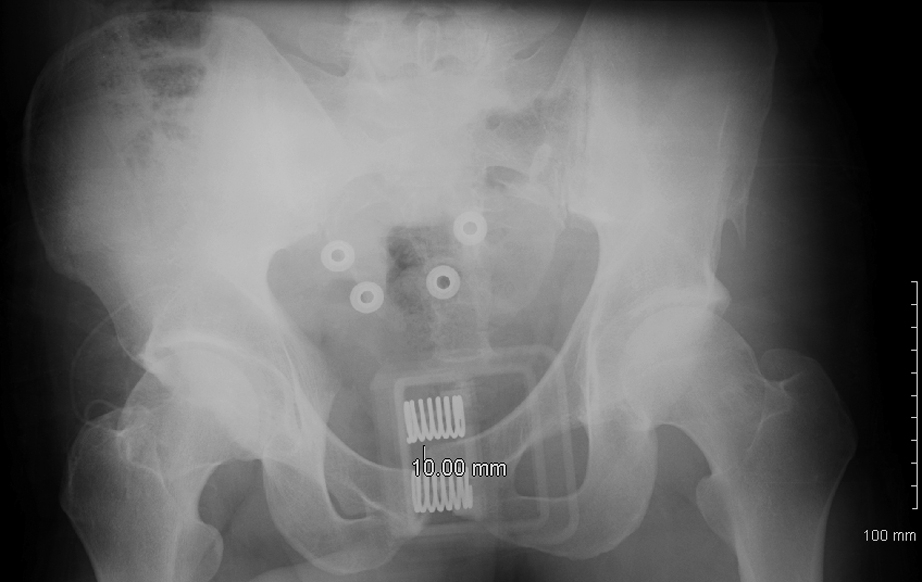
Preoperative pelvic radiograph. Anteroposterior view with pelvic binder in place, demonstrating 10 mm of vertical public symphysis displacement.
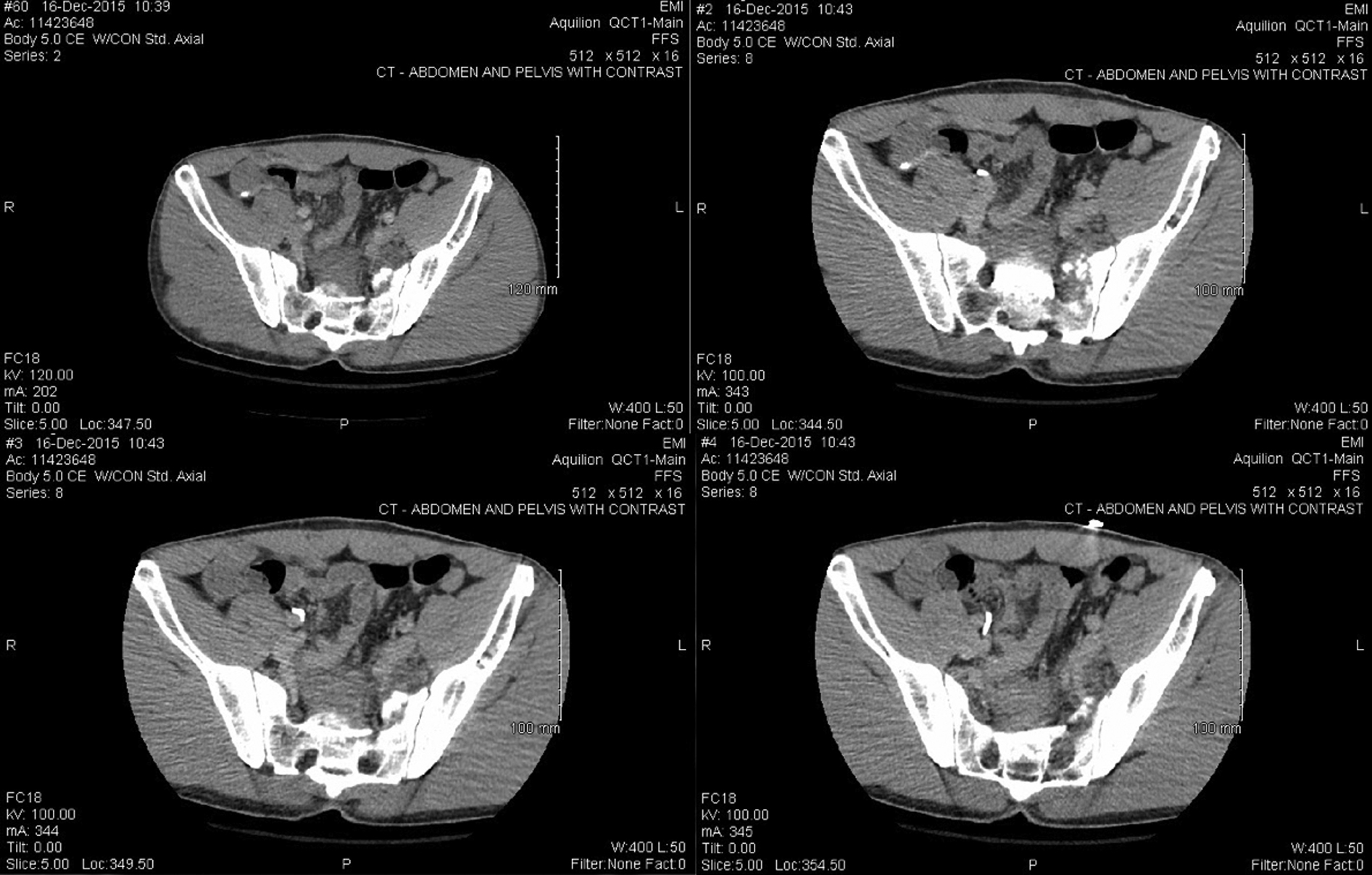
Preoperative pelvic computed tomography, axial series.
The patient was brought to the operating room for open reduction and internal fixation with an anterior symphyseal plate and posterior sacroiliac joint fixation. Anterior fixation was performed with a 4-hole pubic symphysis plate. Posterior fixation began with a percutaneous incision. A guide pin was advanced through the incision under fluoroscopic guidance. A transiliac-transsacral guide pin was placed adjacent to the S1 body, and a lateral x-ray was taken to ensure appropriate placement posterior to the iliac cortical density. The length was measured, and a fully cannulated screw was driven through the right and left sacral ala. The guide pin was then removed. AP inlet and outlet films were taken, and both reductions and hardware placements were adequate (Figure 5).
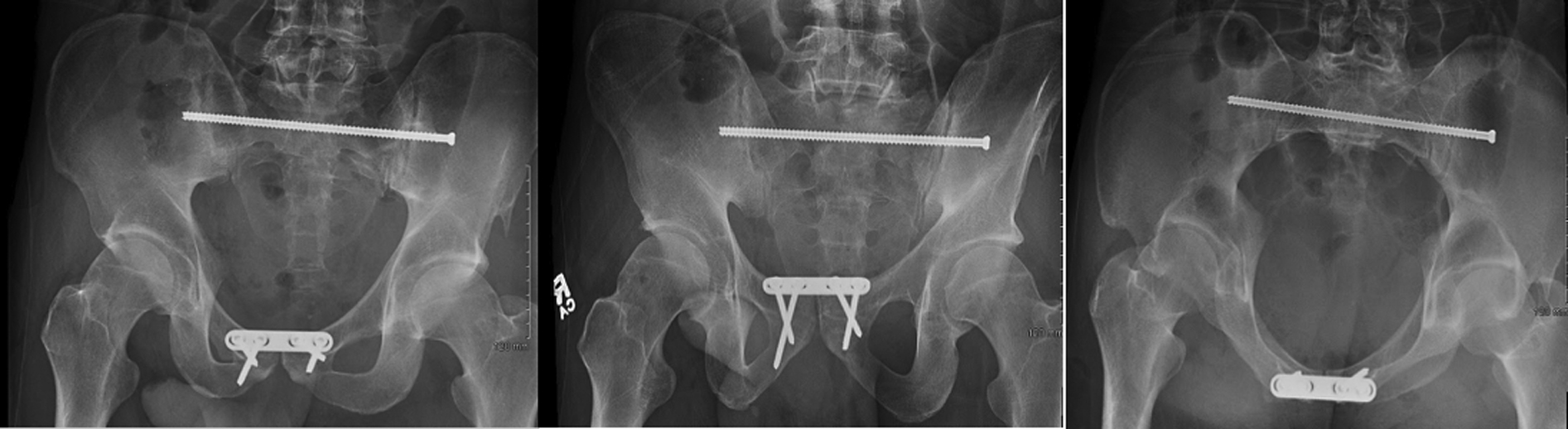
Postoperative pelvic radiographs, anteroposterior, inlet, and outlet views.
After the operation, the patient was seen by physical and occupational therapy to improve his mobility under recommendations from the orthopedic surgery service. He reported mild dizziness during one of these therapy sessions and was found to be anemic, with a hemoglobin of 7.2 g·dL-1 and a hematocrit of 21%. He was transfused 1 unit of blood, which resolved his symptoms. Once he began tolerating a full diet and was transitioned to oral pain medications, discharge planning was started. Nine days after being admitted, he left the hospital and returned home.
Discussion
The current literature supports the idea that most surfing injuries are minor and consist of lacerations, sprains, and strains.1,6,7 Most of these injuries are caused by the surfer’s own motions or by impact with the surfboard or ocean floor. Most of these patients are discharged when they present to the hospital, and current data suggest that the rate of hospitalization for surfing injuries is approximately 10%. 2 However, it is unclear from the research what percentage of these hospitalized injuries are life threatening. This case is the first case report of an acute pelvic fracture during a professional surfing event and supports the idea that there is potential for severe traumatic injury when participating in surfing and similar water sports. The mortality of closed pelvic fractures is estimated to be around 15%. 8 Because of the forces involved, pelvic fractures are isolated in only 20 to 40% of cases 9 and commonly are associated with chest trauma, long bone fractures, and head or abdominal injuries. 10 The leading cause of death in these patients is hemorrhage, likely from the sheared sacral venous plexus and small to medium arteries of the pelvic retroperitoneum or associated abdominal injury.11,12
With blunt traumatic injuries, there must be a high initial suspicion for pelvic injury that should be identified in the primary assessment as part of the catastrophic hemorrhage assessment, along with airway and breathing issues. The literature suggests that owing to the significant incidence of missed pelvic fractures in patients who have experienced blunt trauma, pelvic stabilizer placement should be considered in the prehospital environment. 13 These pelvic binders are effective in reducing pelvic volume and decreasing pelvic mobility while being safe, noninvasive, and easy to apply.14,15 Other management principles should be consistent with advanced trauma life support guidelines, including monitoring for signs of hypovolemic shock and applying fluid resuscitation through large bore intravenous access. Minimal response to fluid resuscitation is indicative of increased risk of mortality 9 and requires urgent transfer to a facility capable of definitive control of hemorrhage, which may include fixation, angiography, and embolization. 12
In this case, a 32-y-old male patient had an anteroposterior type III fracture.16,17 This injury pattern is caused by extreme anteroposterior compression and results in the complete separation of the hemipelvis from the remainder of the pelvic ring. 18 Definitive surgical intervention for this injury requires an anterior symphyseal plate and posterior stabilization with sacroiliac screws or plate. The patient underwent both procedures within hours of his initial injury, including posterior fixation with a single percutaneous iliosacral screw, which has been shown to be noninferior to 2-screw fixation. 19 This time frame was beneficial; it has been shown that a prolonged time to operative pelvic fixation leads to worse functional outcomes. 20
The orthopedic literature demonstrates that despite early surgical intervention, significant functional impairment remains. 21 The most common sequelae are chronic back pain or sacroiliac joint pain.5,22,23 These sequelae commonly prevent patients from ever returning to work, and only 35% of individuals are able to return to work without modifications. The patient returned to surfing 6 mo after the initial injury but reported residual tightness in his lower back. This is a common complication of iliosacral pin fixation. 24 Pin removal is still controversial but may provide pain relief. The patient decided to have the iliosacral pin removed approximately 14 mo after the initial injury. He reported immediate increased mobility and reduced stiffness. Remarkably, this patient returned to professional surfing competition. He successfully competed in the same pipe masters event at Pipeline just 12 mo after his initial injury.
Although definitive care was provided by the orthopedic surgeons at the referral hospital, immediate life-saving care was provided by the on-site medical staff, including lifeguards, paramedics, and physicians. The importance of removing the athlete from immediate hazards after injury should not be understated. The outcome of this case may have been different had the initial water rescue taken longer, allowing another set of waves to break on top of the patient. If these powerful waves had reached the defenseless and incapacitated surfer, they not only would have jeopardized the surfer’s life but prolonged his watercraft rescue. This case highlights the fact that a multidisciplinary and connected team of professionals is required to achieve the best possible outcome for both professional and amateur athletes who sustain an injury.
Conclusions
Surfing is an increasingly popular and generally safe sport. However, as the level of competition increases, bigger waves are being ridden, and the complexity of maneuvers has increased. The forceful impact and compression from the energy of larger and more challenging waves can result in life-threatening injuries. This results in a greater risk of severe injury, mortality, and morbidity than previously recognized. Medical staff and event organizers of both recreational and competitive surfing events need to prepare and have a treatment and transport plan for the management of not only common, minor injuries, but also rare life-threatening injuries. Tools such as emergency action plans should be designed and implemented well before each contest. Emergency plans should reflect the roles of all of the stakeholders, while taking into account each locale’s unique conditions and resources. Being able to quickly and reliably rescue, resuscitate, stabilize, and transfer these patients to definitive care is essential in minimizing mortality and maximizing their functional outcome. With appropriate preparation and planning, medical and prehospital professionals can provide athletes with the greatest chance of returning to their sport at the highest levels of competition.
Footnotes
Acknowledgements
Author Contributions: All authors contributed equally to the writing of this manuscript.
Financial/Material Support: None.
Disclosures: None.