
Abstract
Keywords
Introduction
An insect entering the external auditory canal (AC) is a common, yet distressing occurrence that can lead to significant discomfort, pain, and psychological distress. The insect itself, as well as attempts to remove it, can result in injury to the tympanic membrane (TM) or AC. In some cases, if the insect is not completely and promptly removed, secondary infections may develop.1,2
Standard methods for insect extraction include suction, wound glue, irrigation, or forceps, sometimes accompanied by mineral oil or lidocaine to first immobilize or euthanize the insect. However, in a wilderness setting, access to even basic medical supplies is often limited, requiring improvisation with available resources. This is further complicated by the risk of injury when using instruments without adequate visualization.1–3
We describe the successful removal of an insect from the ear of a wilderness medicine instructor using only duct tape and a headlamp, demonstrating a feasible alternative for insect removal in remote settings.
Case Report
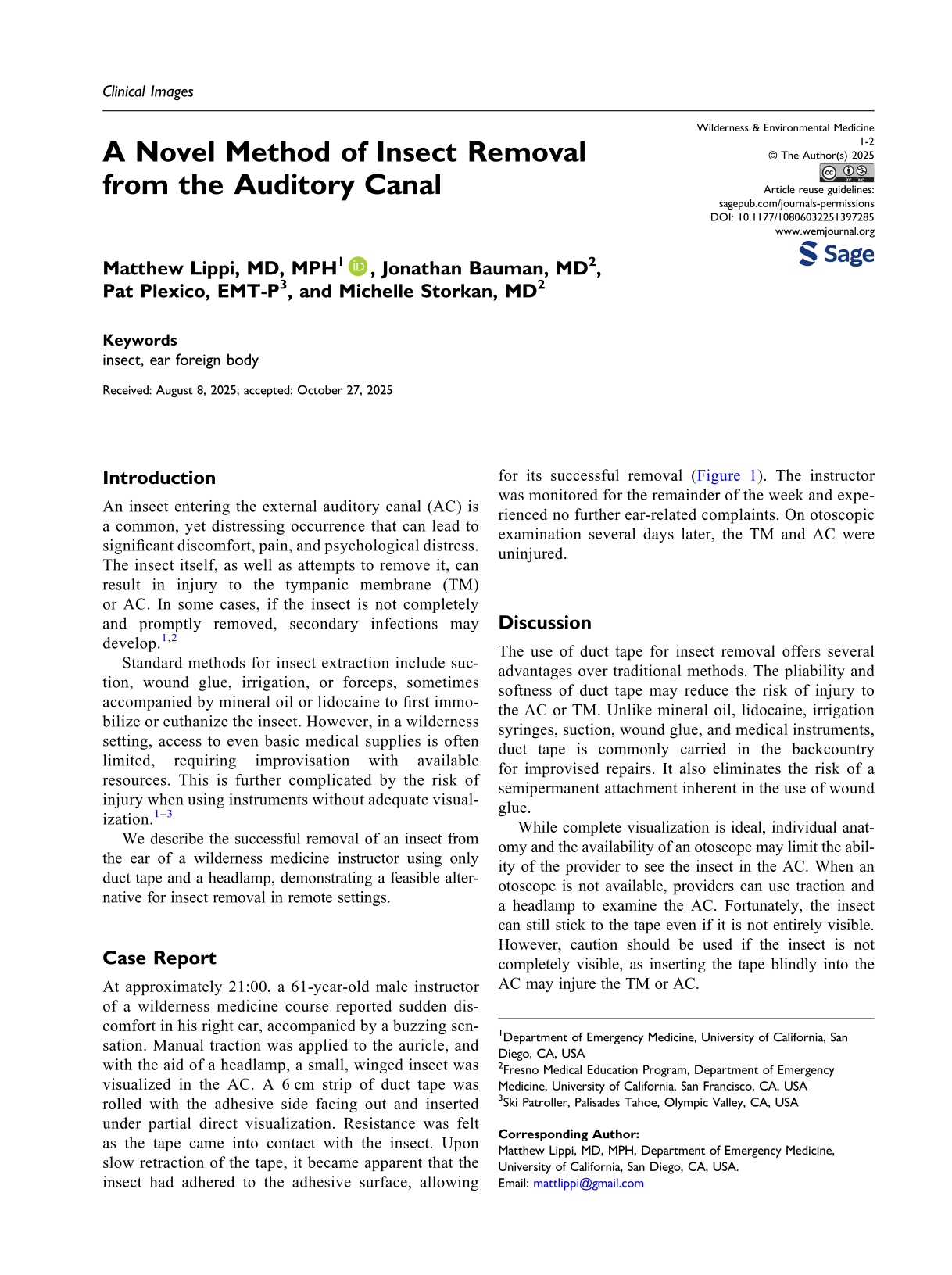
At approximately 21:00, a 61-year-old male instructor of a wilderness medicine course reported sudden discomfort in his right ear, accompanied by a buzzing sensation. Manual traction was applied to the auricle, and with the aid of a headlamp, a small, winged insect was visualized in the AC. A 6 cm strip of duct tape was rolled with the adhesive side facing out and inserted under partial direct visualization. Resistance was felt as the tape came into contact with the insect. Upon slow retraction of the tape, it became apparent that the insect had adhered to the adhesive surface, allowing for its successful removal (Figure 1). The instructor was monitored for the remainder of the week and experienced no further ear-related complaints. On otoscopic examination several days later, the TM and AC were uninjured.

Insect adhered to rolled duct tape after removal from the auditory canal.
Discussion
The use of duct tape for insect removal offers several advantages over traditional methods. The pliability and softness of duct tape may reduce the risk of injury to the AC or TM. Unlike mineral oil, lidocaine, irrigation syringes, suction, wound glue, and medical instruments, duct tape is commonly carried in the backcountry for improvised repairs. It also eliminates the risk of a semipermanent attachment inherent in the use of wound glue.
While complete visualization is ideal, individual anatomy and the availability of an otoscope may limit the ability of the provider to see the insect in the AC. When an otoscope is not available, providers can use traction and a headlamp to examine the AC. Fortunately, the insect can still stick to the tape even if it is not entirely visible. However, caution should be used if the insect is not completely visible, as inserting the tape blindly into the AC may injure the TM or AC.
Insect removal from the AC can significantly alleviate discomfort and prevent the need for urgent evacuation. However, as with all removal methods, the use of this technique includes a risk of TM or AC injury, secondary infection, or unintentionally pushing the insect deeper into the AC. Despite these risks, this case demonstrates that duct tape can safely and effectively be used to remove an insect from the AC in a remote wilderness setting when traditional methods are unavailable.
Footnotes
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.