
Abstract
A live insect within the external auditory canal is an unpleasant possibility during wilderness recreation. To our knowledge, no study has attempted to quantify the risk of this event occurring in the wilderness. However, such events anecdotally seem to occur with some regularity in a variety of climates. Most cases are benign, but a small subset of patients can develop complications including infection, hearing loss, and vestibular complaints related to the foreign body. In the emergency department or clinic, removal of the insect is a simple procedure in most circumstances; however, the material and expertise required for backcountry removal of the insect are often limited. With this consideration in mind, we offer a conservative approach to backcountry insect removal based on a selective review of the published literature on this topic. Where published data are lacking, we make recommendations based on anecdotal experience of the authors dealing with this condition in austere environments and in the emergency department. We recommend insect removal only if the patient is acutely symptomatic and the insect is visualized and graspable with the instrument used for removal. In any other circumstance, intervention should be deferred until definitive care is reached because of risks of complications associated with removal, including infection, bleeding, and tympanic membrane damage.
Introduction
Having an insect take up residence in one’s external auditory canal is an unfortunate potential complication of sleeping outside. It can be a significant source of disability that results in shortened or aborted backcountry trips. There was a dramatic example in July 1957. At the Boy Scouts of America’s National Jamboree in Valley Forge, Pennsylvania, 186 campers experienced Asiatic garden beetles crawling into their ear while they slept. 1 We discuss the current evidence behind the decision to intervene on a retained insect in the ear that does not spontaneously resolve, and the more commonly accepted clinical practices for management of this condition in the austere, low resource environment of the backcountry.
Methods
A search query with the keywords “insects” and “external auditory canal” was entered into the PubMed database. This yielded 56 publications, including formal research, case reports, and case series. Each of these publications were manually searched for results sections with quantitative data related to the extrication of insects from the external auditory canal. These papers were prioritized for inclusion in the manuscript. Two additional publications not included in the PubMed search were also used from select wilderness medicine textbooks. The textbooks were chosen based on the authors’ prior knowledge of their information on wilderness medical kits. After reading cited literature on the insecticidal activity of different reagents, 2 an additional PubMed search was undertaken with each of their reagents as a keyword along with “ototoxicity.” We combined all of these reports with our own experience in the wilderness and in the emergency department to generate our recommendations for insect removal.
Epidemiology
Foreign bodies in the ear are a common complaint in the emergency department setting, and of these, a significant proportion are the result of insects in the external auditory canal. In the adult population, it is estimated that up to 80% of presentations with the chief complaint of external ear foreign body are due to live insects. 3 -5 In the pediatric population, due to children’s proclivity to intentionally place objects in the external auditory canal, this is a lower but still significant 4 to 20%.6,7 The most common insect causing such problems is the American cockroach, which is estimated as the culprit in 50% of insects in the ear. 1 Anecdotally, the majority of emergency department presentations for retained insects happen during routine activities near the home, but prolonged outdoor trips seem to increase the risk.
Clinical Manefestations and Differential Diagnosis
The decision to attempt removal of an insect in the wilderness should be systematic and thoughtful. The initial symptoms of a retained insect may be mild, with only 12 to 36% of patients experiencing otalgia, hypoacusis, or otorrhea; however, up to 20% can experience complications (discussed herein).4,8
In most patients, the clinical history and direct visualization alone are sufficient to diagnose an insect foreign body. However, it is important to consider a broad set of pathologies when presented with a less revealing presentation. A preliminary differential diagnosis for acute otalgia with otorrhea and hypoacusis includes otitis media with tympanic membrane perforation, cerumen impaction, cholesteatoma, otitis externa, otomycosis, and barotrauma in the right clinical setting. Because otoscopy is not feasible in the wilderness setting, it can be difficult to differentiate these entities if there are no distinguishing features on external inspection.
Complications of Insect Retention and Removal
The most common adverse event of removal of an ear foreign body outside of care by an otolaryngologist is damage to the external ear canal. 4 While complication rates after removal by an otolaryngologist are as low as 4%, that risk increases to 48% when the procedure is carried out by a nonotolaryngologist. 4 One study did estimate a complication rate of 26% when performed by otolaryngology, but the authors noted that they did not consider prior unsuccessful removal attempts by other medical or nonmedical persons. 9 The most common complication identified was a meatal laceration, occurring 15% of the time. 9 Less common were tympanic membrane perforation and otitis externa, occurring in 74% of removals. 9 There is no known data to suggest how complication rates in the wilderness compares to complication rates by otolaryngology in the emergency department. Complication rates of ear foreign body removal could further be stratified into graspable and nongraspable groups, with the graspable group having a higher success rate (64 vs 45%) and lower complication rate (14 vs 70%). 6 It is important to consider infectious sequela of these potential meatal lacerations when definitive medical care is not readily available. Acute otitis externa was documented in 3 to 7% of removals by nonotolaryngologists.4,9 These relatively minor complications, when left untreated, can lead to more severe complications. Although rare, these include ossicle damage and potentially fatal conditions like mastoiditis, osteomyelitis, and cavernous sinus thrombosis.10,11
The risks of leaving an insect in the ear while completing the trip should also be considered. There is a theoretical risk of trauma caused by continued movement of the retained insect, as well as sequela of such trauma, including infection and bleeding. It is often difficult to distinguish between trauma caused by the insect prior to removal versus trauma occurring during the removal procedure itself. There are rare case reports of serious infections including skull base osteomyelitis and cavernous sinus thrombosis due to retention of an insect in the ear, but complications seem to have occurred 10 or more days after an unsuccessful removal attempt. 11 In general, it is thought that leaving the insect, even if there is sensation of animation, is safe if the patient is able to tolerate the symptoms. 12
Indications for Removal
Given the potential complications of removal, if the patient is asymptomatic, we recommend observation only until out of the wilderness. Treatment should then be performed in the hospital or office setting by a clinician, preferably an otolaryngologist.
If the patient is acutely symptomatic, consideration can be given to killing the insect using the methods described below. After killing the insect, the patient should be reassessed for continuation of distressing symptoms, including otalgia. If the patient continues to be symptomatic, then risk of injury during removal should be weighed against the benefit of dislodging the insect.
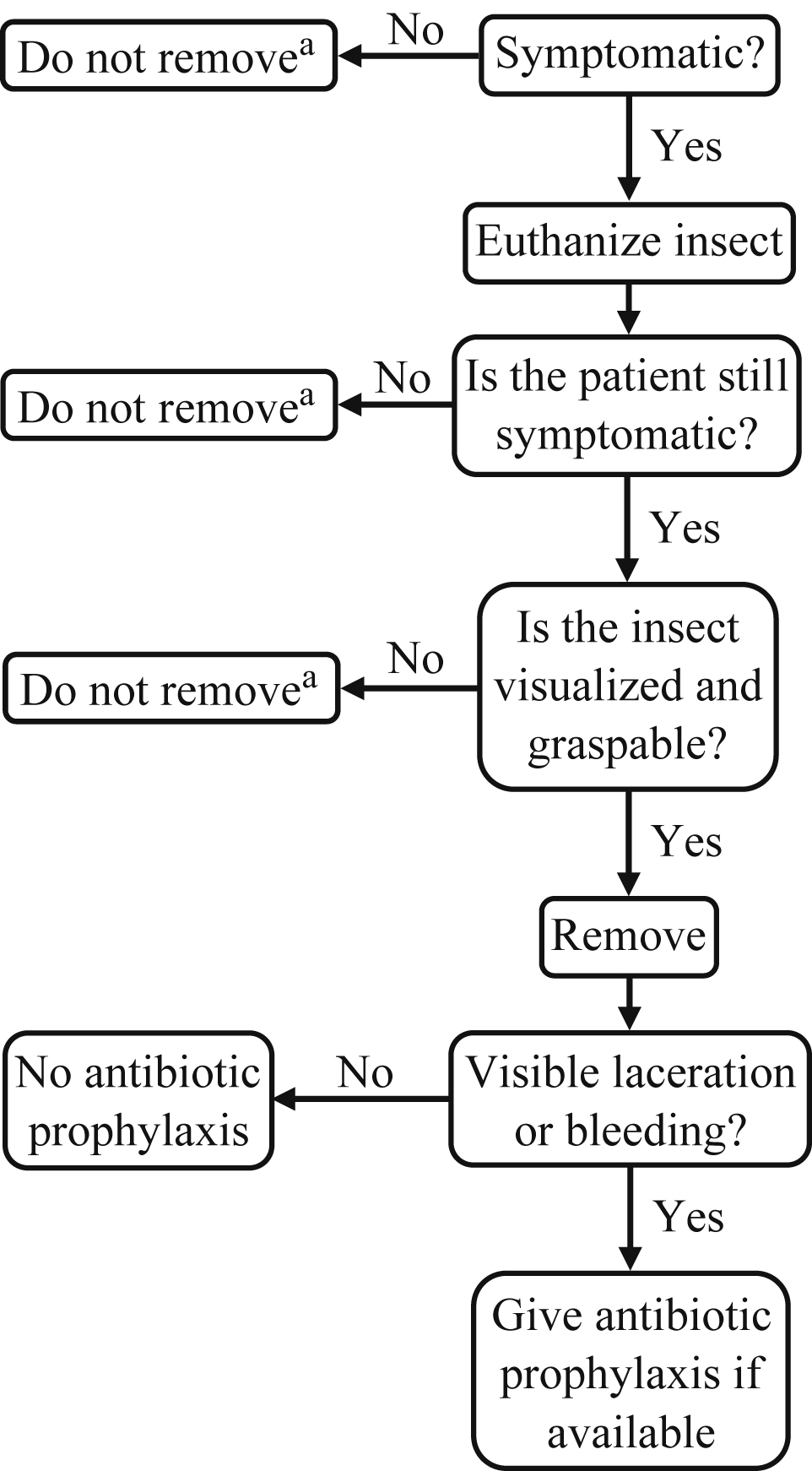
Decision tree for wilderness removal of intra-aural insect foreign body. a Once the trip has finished, seek removal by a medical professional.
Removal Technique
In the controlled hospital setting, a clinician has many tools at their disposal for the killing and removal of an insect; however, many of these tools are not common in the wilderness setting. Most adventurers will not carry an otoscope to aid in visualization of the insect. Of the items recommended by the Wilderness Medical Society to be carried in a wilderness medical kit, the items of potential utility in insect foreign body removal are as follows: tweezers, lidocaine, ethanol pads, and povidone/iodine swabs. Oral antibiotic pills (eg, amoxicillin-clavulanate, ciprofloxacin, or doxycycline), water, salt, vegetable oil, and soap are also helpful adjuncts in management. 13 Other common agents used for insect protection, including DEET and various other sprays, have not been studied in the context of insect removal from the external auditory canal, so we cannot recommend them.
The strategy for removal of an animate ear foreign body consists of 2 steps: killing/immobilizing the insect followed by removal. This stepwise approach is done to ensure the insect does not damage the external auditory canal during the removal (Figure 1).
Insecticides used for extermination of insects are generally split into 3 groups: anesthetics, antiseptics, and miscellaneous liquids (eg, water, saline, soapy water). In a study of the efficacy of different insecticides in vitro, all 3 groups can effectively kill insects (eg, roaches, bees, and beetles) with the exception of ticks, which did not die even after 3 min of submersion. 2 A faster time-to-kill is ideal, as it minimizes the time the insect has to react and cause further harm to the external auditory canal.
Of the 3 aforementioned categories, antiseptics seem to be the most efficacious, resulting in faster kill times than anesthetics or miscellaneous liquids in an in vitro setting. 2 The most likely antiseptics to be available for use in the backcountry are ethanol, povidone/iodine solution, and vegetable oil, which kill either via direct toxicity or suffocation. Of these, vegetable oil and ethanol appear to be the most efficient options, with mean times-to-kill of 28 and 30 s, respectively.2,14 Povidone/Iodine is the next most potent at 58 s. Of note, chlorhexidine is often proposed as an effective killing agent; however, we recommend against its use due to the side effect of ototoxicity. 15 Of the miscellaneous liquids, soapy water was quickest at 67 s, followed by hypertonic saline at 84 s, saline at 158 s, and water at 180 s. 2 It is important to qualify these data as measured in a controlled laboratory setting, and significant departures from these killing times should be expected in the wilderness setting. In our experience, reapplication of the killing agent may be required if the patient continues to have animate foreign body sensation after the initial killing attempt.
Of the anesthetic options, lidocaine is most commonly used in the emergency department setting and the best studied in the literature. Many popular wilderness medical kits have a small amount of topical anesthetic available, and many wilderness-oriented health groups recommend bringing lidocaine on general expeditions.13,16 While lidocaine and other similar topical anesthetics have been shown to be effective, the risk of vertigo should be considered.17,18 The pathophysiology of vertigo is uncertain, but thought to be the result of lidocaine infiltration into the middle ear then through the round window into the inner ear, where it exacts its sodium-channel antagonism on receptors in the membranous labyrinth. 19 This risk would presumably be higher in a patient with a tympanic membrane perforation. Varying degrees of vertigo were reported in 4 of 9 subjects of a case series where lidocaine was injected over the promontory of the cochlea prior to eighth nerve monitoring. 18 Such a scenario simulates a tympanic membrane perforation and the patients had severe symptoms as a result: 6 to 9 h of incapacitating dizziness, staggering gait, and nausea with or without vomiting.17,18 And although tympanic membrane perforation is diagnosed via otoscopy, vertigo is possible with an intact membrane.17,20 In the austere environment, such debilitation can be a great hazard, not only for the patient but also for the rest of the team, who are tasked with the care of a patient while they themselves are exposed to the elements. In the case series above, symptoms were resolved with antiemetic agents. 18
The agent used for euthanization will likely be decided based on availability. However, if multiple options are available, we recommend vegetable oil as the first line based on reported killing ability and low risk profile. 2 Anecdotally, we have found success with the viscous vegetable oil compared to other liquids because vegetable oil allows for a small amount of movement of the patient’s head during euthanasia without the oil quickly draining from their ear. Ethanol, povidone/iodine, hypertonic saline, soapy water, or water (ensuring the water is potable) is a viable alternative agent depending on available resources.2,14 Because of the debilitating effects of vertigo, we recommend against the use of lidocaine and other topical anesthetics if the decision to remove a live insect is pursued. Once an agent has been chosen, it is important to warm the liquid to near body temperature prior to infusion, as cold-water irrigation can precipitate vertigo.
The second step of insect foreign body removal is the removal itself. Although no studies have been done to investigate whether euthanization of the insect reduces symptoms before removal, the authors’ clinical experience has found this to be the case. Therefore, even if the patient is initially symptomatic, their symptoms should be reassessed post-insect euthanasia to determine whether removal should be considered. Because the instrument being used to remove an insect will likely be basic tweezers or forceps, it is important for the medical provider to be confident in their ability to remove the insect. As discussed above, a prerequisite for removal is that the insect be graspable, as nongraspable objects have higher failure and complication rates than graspable ones. Another factor to consider is the physical properties of the bug itself. A study observing the success rates of emergency department providers showed that the shape and hardness of the foreign body can greatly affect the difficulty of removal. 21 This study employs the terms of “soft, irregular” and “firm, rounded” to characterize the foreign body. Using mostly forceps or flushing, “soft, irregular” objects were successfully removed 86% of the time. In contrast, “firm, rounded” objects were only removed by the same methods in the emergency department 34% of the time. 21 In the wilderness, it is reasonable to assume success rates for removal would be even lower than in the emergency department when using similar removal methods. 9 A 67% success rate is seen when direct visualization alone is used for removal. 9 In addition, it is the authors’ experience that even after removal of superficially-located insects, insect parts tend to remain in the external auditory canal. Because of that, the potential benefit of avoiding a clinic visit with wilderness removal is negated, as follow-up should occur to ensure complete removal. Negative consequences of removal discussed above should also be considered carefully before removal. If removal is deemed too difficult or the patient is no longer symptomatic, the dead insect should be left in place until removal can be performed by a trained provider in a definitive clinical setting.
If the decision is made to remove the insect, proper technique is important to maximize success rates.
21
Visualization. Adequate visualization should be a requirement prior to removal of the insect. In the wilderness, perhaps the most beneficial light source will be a camper’s headlamp. If the insect is visualized but retreats farther into the ear canal when stimulated with the light source, the removal should be aborted. Preparation for irrigation. Once an available irrigation solution has been chosen as discussed, make sure the solution is as close to body temperature as is feasible. Then fill a container that will allow for a pressurized stream of solution during irrigation. We recommend a 60 mL syringe with a narrow tip if available. If a syringe is not on hand, creation of a small perforation in an improvised container (eg, a clean, compressible water bottle or plastic bag) may serve as a possible alternative. Irrigation. Direct steady stream of irrigation solution behind the insect in the external auditory canal. Multiple washes can be used. Wait several minutes and reassess the insect’s position and movement. In the ideal irrigation, the insect will become dislodged and become easier to remove. After allowing time for euthanization and reassessing the patient’s symptoms, attempt removal of the insect with the smallest available forceps under direct bright light visualization. During removal, take note of debris that remains in the external ear.
Alternative Removal Techniques
Various other techniques have been described both anecdotally and within the literature that could be feasible in a resource poor pre-hospital setting, including light assisted removal, 22 and cyanoacrylate (superglue) 23 added to cotton swabs. The authors have not seen such techniques employed in either the clinic or austere settings. If providers have experience with these techniques, they may be viable. However, partial or full occlusion of the external auditory canal with adhesive material is a likely complication, especially in the anxious patient who is not completely still.
Post-Removal Considerations
Once an insect has been successfully removed from the ear, further management of symptoms is important to maximize patient comfort and reduce risk of infection. Pain within the ear canal can be expected in the period after insect removal and is reasonable to treat with basic analgesics brought on the trip, including acetaminophen and ibuprofen. People with signs and symptoms of active infection, including fever, spreading erythema, and purulent discharge should be immediately evacuated if possible. Patients with comorbidities that predispose to malignant otitis externa (eg, diabetes, immunosuppression) should carry a lower threshold to begin evacuation. Additionally, intractable vertigo should also be evaluated as these patients can decline quickly and lose the ability to participate in their own extrication from the austere environment.
It is generally accepted that patients with evidence of external auditory canal trauma after removal should receive antibiotic ear drops, typically of the fluoroquinolone class.24,25 If tympanic membrane rupture is suspected, only fluoroquinolone drops should be used to avoid middle ear ototoxicity caused by other antibiotic classes. However, the rate of infection after foreign body removal in patients who either have or have not received antibiotic drop prophylaxis is not well studied. Oral antibiotic prophylaxis after external auditory canal trauma, on the other hand, is not routine management and there is no proven efficacy of this practice. We therefore recommend using clinical judgement before administering oral antibiotics for minor ear trauma. Systemic antibiotics carry risks of their own, including allergic reactions and diarrheal disease. Consider basic wound care alone (eg, boiled water irrigation with careful monitoring for signs of infection) in cases of minor trauma.
While there is little data on the pathogenicity of skin infections in the wilderness, it is reasonable to assume that common skin flora (eg, staphylococcus and streptococcus species) are major contributors to otitis externa in the wilderness. We recommend treatment with amoxicillin/clavulanate, a cephalosporin of any class, doxycycline, or trimethoprim/sulfamethoxazole. 18 Pseudomonas infection is an additional concern specific to otitis externa, and is best treated with an oral fluoroquinolone like ciprofloxacin if ear drops are unavailable. Additional research is needed to identify wilderness-specific causes of otitis externa and skin and soft tissue infections in general, as etiology likely varies widely by environment.
Conclusions
Live insects within the external auditory canal represent a rare but potentially debilitating condition across a wide range of expedition environments. We recommend that euthanasia of insects, ideally using vegetable oil or ethanol, be attempted in symptomatic cases. Insect removal should not be attempted unless the patient continues to be symptomatic post-euthanasia and the benefit of removal is deemed to outweigh the risks (infection, middle ear trauma).
Footnotes
Acknowledgements
Author contributions: Study concept and design (AG, BA); drafting and critical revision of the manuscript (AG, BA); All authors approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.