
Abstract
Ice caving accidents are rare, but when they occur, they represent unique logistical and medical challenges for both explorers and rescuers. Factors such as the dynamic nature of the environment, exposure to cold temperatures, and complex extrication logistics should be taken into account. A hybrid approach between mountain and cave rescue techniques may be necessary. In this article we describe in detail a case of a rescue operation following a 15-m fall into a moulin on a glacier in Switzerland. We discuss the combined use of mountain and cave rescue techniques, adapting to the unique structure of the moulin. Our case demonstrated that even though such incidents are extremely rare, the complexity of this type of rescue can be anticipated and can benefit from optimized rescue strategies based on accumulated experience in both mountain and cave rescue operations.
Introduction
Ice caving is a unique activity that combines glacier mountaineering, canyoning, and caving. Glaciers are dynamic environments. Cold exposure is constant, creating a risk of accidental hypothermia. 1 As in rock caves 2 and crevasses,3–5 accidents in ice caves are poorly documented. During ice cave rescues, rescuers and patients are exposed to unfamiliar environmental, logistical, technical, and medical challenges. Extricating a patient to the surface may require a complex combination of mountain, crevasse, cave, and canyoning rescue techniques. As for cave and complex mountain rescues, specialized multidisciplinary teams are required.6–8 Extrication from a glacier moulin may require navigation through narrow passages, reducing the options for monitoring or intervention. Protection against hypothermia is critical. We describe a case of an ice cave rescue following a fall into a glacier moulin.
Case Report
A 50-y-old male free fell ∼15 m while rappelling into a moulin during an ice caving exploration of a Swiss glacier. The moulin featured an initial 10-m shaft, followed by a meandering passage leading to a final 32-m drop divided into 2 rappels of 12 and 20 m (Figure 1). This complex layout added significant challenges to the subsequent rescue efforts. The entrance to the moulin was located at an altitude of 2600 m on the Moiry Glacier in Valais. Four members were already at the bottom where the patient had fallen. They could only try to keep him warm and awake while waiting. Two of them began setting up pulley systems in case the rescue team couldn’t arrive. The team member who was the closest to the surface in this 6-person team, an emergency physician, ascended the rope. She was able to call for rescue 10 min after the fall. Communication difficulties arose because of cold-induced phone battery failure, limiting the initial information available to rescuers. The dispatch center only received information that there was a fall into a crevasse (whereas it was actually a glacial moulin), with a vague location on the Moiry Glacier. Communication then was lost. The rest of the rescue operation was organized upon the rescuers’ arrival.
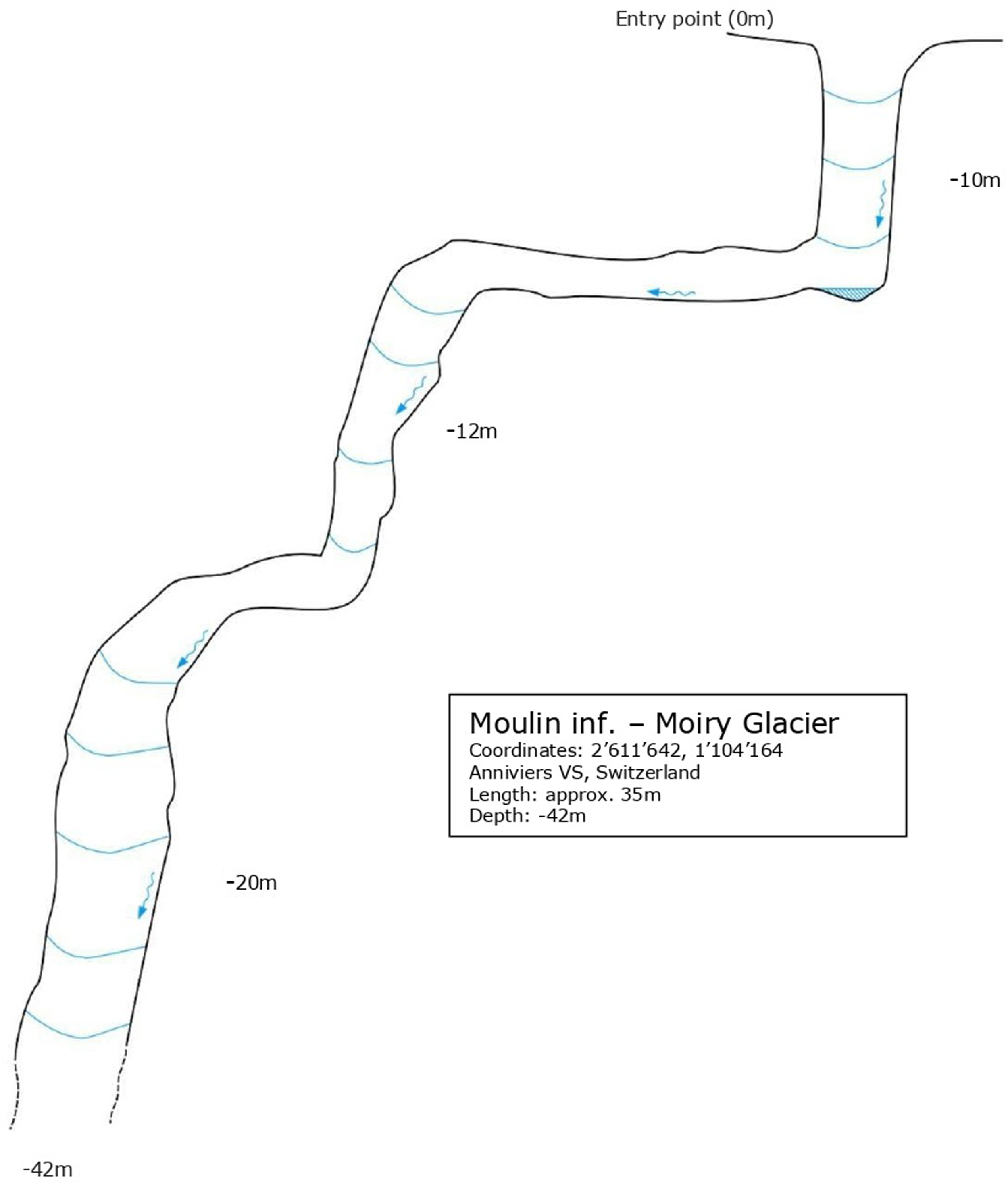
Longitudinal Section of the Moulin System.
The rescue team, composed of 3 mountain guides serving as professional rescue specialists and an emergency physician, arrived by helicopter within 20 min, prepared for a crevasse rescue and not for an ice cave rescue. The exploration team physician joined the rescue team because of her familiarity with the environment, the rescue team, and the fact that she already had the necessary clothing and equipment (ie, headlamp, drysuit, and crampons). The rescue setup involved a tripod anchor system (Figure 2), several ropes, radios, an extrication kit with a Kendrick extrication device (KED), a cervical collar, and a pelvic binder. The team had only a few intravenous medications (eg, fentanyl, ketamine, midazolam, and epinephrine, as well as crystalloid solution [NaCl 0.9%]). One rescue specialist started to descend into the moulin to reach the patient while the physician prepared to descend with the crevasse tripod. During the physician’s descent, the rescuers planned to test the possibility of lifting the patient using the crevasse tripod, despite the structure of the moulin. This potentially would require direction changes.

Tripod Anchor System on Moiry Glacier at 2600 m.
On reaching the patient, the physician found him conscious, supine, in contact with glacial meltwater, and not shivering. He was wearing a thick neoprene wet suit, neoprene socks, and a rain suit. Because access was difficult, no monitoring equipment or thermometer was available. Only a basic primary assessment was performed. The patient was hemodynamically stable with normal respiration and a Glasgow Coma Scale score of 14 (E4/V4/M6). There were no focal neurologic deficits. There were injuries of the left elbow, back, and pelvis, but there was no thoracic or abdominal tenderness. Because of the suspicion of spinal and pelvic fractures, the team stabilized the spine using a cervical collar and the KED and stabilized the pelvis with a pelvic binder. Establishing intravenous access was challenging because of vasoconstriction, but a 22-gauge venous catheter was placed, and a total of 75 micrograms of fentanyl (1 microgram·kg-1) were administered for pain. No other medication was given.
The extrication took more than 30 min, requiring careful coordination by radio because 1 rescuer was hauled up alongside the patient in a vertical position. This allowed for stability and careful guidance during the extrication. The rescuer and the patient were extricated using the tripod system, with additional direction changes made necessary by the complex topography of the moulin. The system was operated by the second rescuer (Figure 3). The physician was positioned at the redirect point in case the patient's condition deteriorated. Once on the surface of the glacier, the patient was secured on a spine board and rapidly evacuated by helicopter as weather conditions deteriorated. The time from the accident until the patient was placed in the helicopter exceeded 2 h.
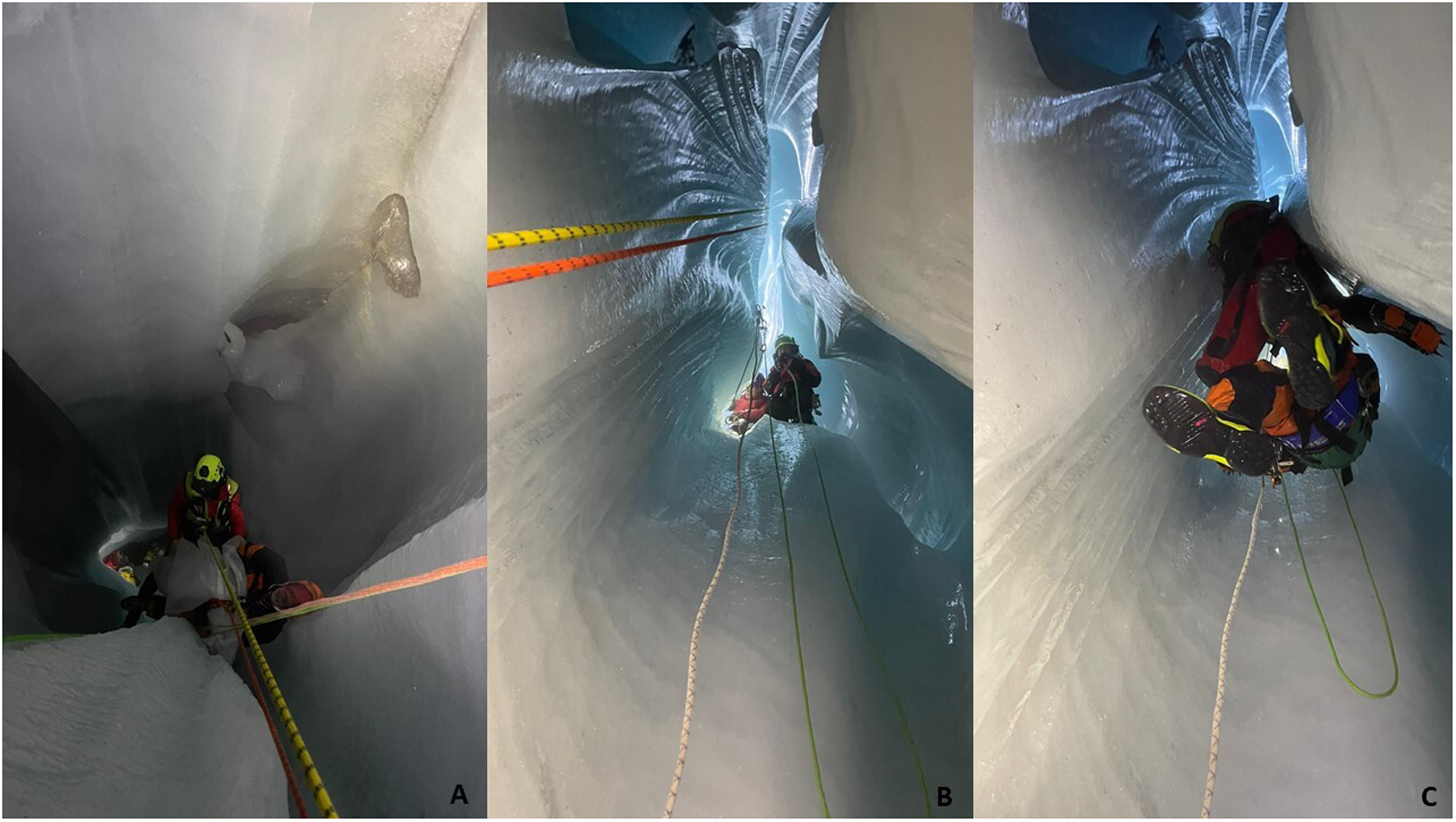
Patient Extraction by the Rescuer.
Transport time to the hospital was 10 min. En route, the patient remained hemodynamically stable. Supplemental oxygen was administered. The patient was protected from heat loss with warm blankets and bubble wrap. At the hospital, the patient had normal respiration and was hemodynamically stable. He was cold stressed with an epitympanic temperature of 35.2°C. He was diagnosed with a small subdural hemorrhage in the right superior frontal sulcus. Additional findings included hemorrhagic infiltration of anterior and inferior mediastinal fat and a nondisplaced anterior sternal fracture. Multiple fractures involved lumbar vertebrae, pelvis, and sacrum, with retroperitoneal fat stranding along the abdominal aorta and a presacral hematoma. Additional bone injuries affected the left elbow and right ankle. The patient received 2 units of whole blood. He underwent surgery for the pelvic and ankle fractures. No hemostatic intervention was necessary. The patient recovered well and was discharged home after 12 d.
Discussion
As far as we know, this is the first published case of an ice cave rescue. It highlights the technical complexity of rescue from a moulin—characterized by darkness, poor radio communication, narrow passages in a dynamic austere environment, and multiple direction changes, which can be technically challenging in confined spaces. The rescue necessitated a hybrid approach combining technical mountain rescue and cave rescue techniques. In some countries, such as Switzerland, the national cave rescue organization operates independently from traditional mountain rescue services. 7 Cooperation between mountain and cave rescue teams has been documented 6 but not, as far as we are aware, in an ice caving accident.
Glaciers are dynamic environments. Conditions inside a moulin can be highly variable, with melting ice altering the landscape within hours, increasing the risk of rockfalls and sudden changes in water flow. The risk of accidental hypothermia from cold exposure may require rapid extrication. 9 As in cave rescue, on-site medical interventions are limited. 8 Because of the confined-space environment, the team prioritized rapid clinical assessment without cardiac monitoring. The rescue physician did not administer tranexamic acid, which might have been indicated, 10 for possible pelvic hemorrhage because she had previously decided to carry only 4 medications in the small medical kit
Because of the confined space, the victim was extricated in a vertical position using a KED (Figure 4). Vertical orientation is often required in crevasse rescues despite being less favorable hemodynamically than the horizontal position.4,11 The use of devices such as the KED allows spinal motion restriction and facilitates movement of the victim, allowing for more rapid rescue. 11 A special cave stretcher could have been the ideal option, but the rescue was carried out by mountain rescue specialists, not knowing at first that it was a glacier cave rescue.
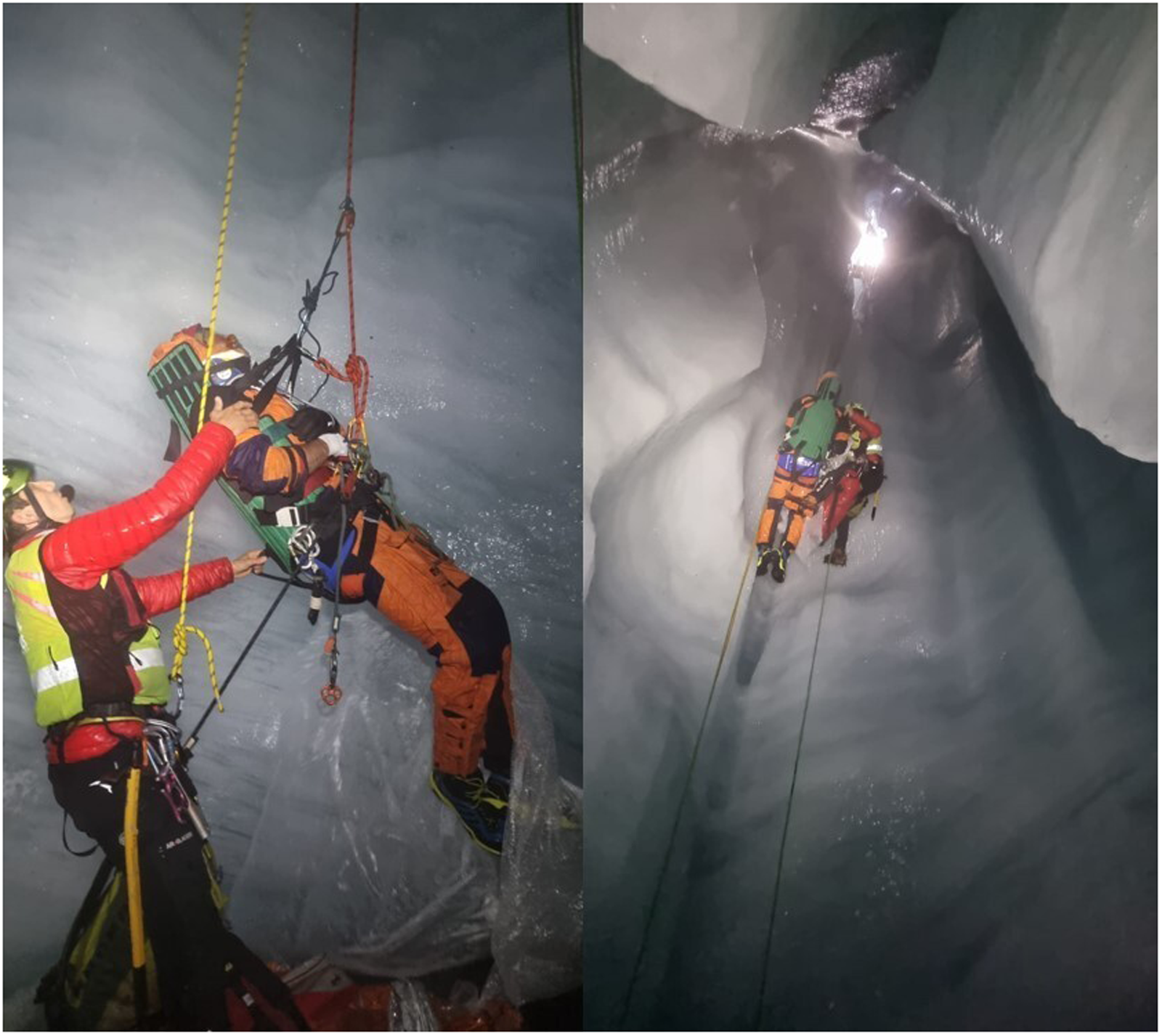
Patient Extraction Facilitated by the Kendrick Extrication Device.
Despite the International Commission of Alpine Rescue Medical Commission (ICAR MedCom) recommendations, 12 the patient was immobilized on a spine board rather than a vacuum mattress. Within our Helicopter Emergency Medical Service (HEMS), the vacuum mattress is the preferred choice. However, for rescue in difficult environment such as this, especially if the patient needs to be transported in a confined environment or will eventually need to be verticalized, we prefer to use a rigid lifting device instead of a vacuum mattress. For cases such as this one, we use the CombiCarrier II (Hartwell Medical LLC, Carlsbad, CA), which is a special lifting and transport device that combines the features of a rescue board and a scoop stretcher. With a transport time of 15 min or less to the emergency department, where the patient is transferred to a soft stretcher, we are able to avoid the formation of decubitus ulcers on a board. The ICAR Med om recommendation states that the use of a spine board is acceptable in certain circumstances but that its use should be brief.
One of the main risks during this rescue was accidental hypothermia. This can become fatal.1,13 However, even in cases of rescue collapse, prognosis can be favorable with proper management and rapid transport to a facility equipped for extracorporeal rewarming.4,13 Fortunately, in this case, the epitympanic temperature, measured at the hospital, was 35.2°C, which was higher than expected given the cold, wet conditions. The patient was protected by his canyoning clothing. This is consistent with previously reported cases of survival in crevasses by victims with adequate garments.14,15
Effective communication and coordination among the rescuers with a combination of technical mountain rescue and cave rescue techniques were key to the success of this rescue. Although it took place in an unusually austere setting, other situations, such as crevasse falls and cave rescues with a risk of accidental hypothermia and difficult extrications, are common in the mountains.3,5 As with complex technical extrications in mountain rescue, standard crevasse rescue techniques had to be adapted to the intricate structure of the moulin, with rigging solutions common in cave rescues. 6 The rescue team was prepared for a crevasse rescue, not an ice cave rescue—a key distinction, because personal equipment, such as dry suits and headlamps, and technical equipment differ between the two types of rescues. Although a tripod is generally sufficient for crevasse rescues, it is often inadequate on its own for ice cave rescues because some moulins extend deep beneath the glacier. In such cases, additional equipment, including rope ascent systems and multiple ropes, is required.
Incidents such as the case we describe are complex and rare but can be anticipated. Rescues in such situations benefit from optimized rescue strategies based on accumulated experience in both mountain and cave rescue operations.6,7
Conclusion
An ice cave rescue requires a combination of mountain and cave rescue techniques and specific clothing, equipment, and devices. Because of the austere conditions, these rescues should aim to minimize extraction time while still ensuring operational safety. The complementarity of rescue teams is a key aspect of the continuous improvement of rescue strategies in this extreme environment.
Footnotes
Acknowledgment
We express our sincere gratitude to Dr. Cedric Luyet, PhD, for the critical review of our manuscript.
Consent for Publication
The corresponding author obtained the written informed consent from the patient to publish his case.