
Abstract
Caving accidents are rare, but when they occur, they represent a unique logistical and medical challenge. Retrieving the patient to the surface often means navigating stretchers through narrow corridors with limited options for monitoring and interventions. Because the patient is usually not fasting, opioids and sedatives should be used with extreme caution. Therefore, alternative analgesic techniques such as locoregional nerve blocks are a promising strategy to improve patient comfort and safety during cave rescues. In this article, we describe 2 cases in which portable point-of-care ultrasound equipment was used to supplement clinical assessment and provide locoregional anesthesia to facilitate patient evacuation and transport. In this context, we discuss the role of portable ultrasound-guided locoregional anesthesia in cave rescue and in the global preclinical context. In summary, our cases demonstrated that the administration of ultrasound-guided prehospital locoregional anesthesia is a safe, rapid, and effective procedure even in extreme situations such as cave rescues. The advent of portable, high-quality ultrasound equipment may open the door for more widespread application of this technique in the global preclinical setting.
Keywords
Introduction
Cave exploration is a unique activity that combines science, sport, and nature. Accidents are rare, with a predominance of nonlethal traumatic injuries to the lower limbs and an overall mortality rate of 6%. 1 Cave rescues present unique logistical, technical, and medical challenges and often require specialized multidisciplinary teams.2,3 Retrieving the patient to the surface may take several days4,5 and involve the rigging of shafts and even the use of explosives to expand parts of the cave. During this time, it is important to protect the patient from hypothermia, and warm sugary drinks and oral food are often given if the medical condition permits. Transporting the patient implies that stretchers must be navigated through narrow passages, with limited options for monitoring or interventions. Therefore, as the patient is usually not fasting, narcotics and benzodiazepines should be used with extreme caution because management of complications or clinical deterioration (eg, vomiting, bradypnea, or aspiration of gastric content) is extremely difficult in these situations. Locoregional anesthesia (LRA) is a promising alternative for pain control in such cases; however, publications on the topic are scarce. 6 Herein, we describe 2 cases of cave rescues in Switzerland in which patient assessment and pain management with LRA was facilitated using a portable point-of-care ultrasound (POCUS) device.
Case Report
Case 1
In January 2022, a 45-y-old female cave explorer fell from a height of approximately 8 m because of a loose rock. The incident occurred approximately 1 h from the cave entrance (530 m away from the surface and 70 m below it), and the rescue operation, which involved 63 rescuers, lasted for more than 2 d. To reach the accident site, very narrow and winding corridors and 3 shafts had to be overcome. Upon arrival of the medical team, the patient complained of severe pain in both her left foot and right arm. The primary survey revealed tachycardia (110 bpm) without signs of systemic hypoperfusion and intact neurological function. A body check revealed a laceration to the right temple and clinical suspicion of a fracture to the right clavicle, a dislocated wrist, and a dislocated left lower leg. An extended focused assessment with sonography in trauma exam using a handheld ultrasound (US) device (Butterfly iQ+) was performed and revealed normal findings.
After immobilization of the left foot and right arm, an intravenous (IV) line was inserted and analgesia was started according to the World Health Organization (WHO) staging scheme. However, despite repeated doses of IV fentanyl and ketamine, the pain was unbearable, and transport was impossible in this condition. The physician in charge decided to perform 2 POCUS-guided nerve blocks (Butterfly): an interscalene brachial plexus block (lateral approach, in plane US needle guidance, injection under the C5 root into the interscalene groove) with 100 mg of ropivacaine and 75 micrograms of clonidine and a popliteal nerve block (in plane single injection, at the level of the bifurcation between the tibial and common peroneal components of the sciatic nerve, approximately 5–10 cm from the popliteal crease) using 90 mg of ropivacaine and 75 micrograms of clonidine (Figure 1). Overall, the procedures were performed within 30 and 15 min. For both blocks, sentinel neurostimulation was used, with aspiration prior to fractionated injection in order to detect any inadvertent IV injection. Both intralipids and benzodiazepines were readily available in case of local anesthetic systemic toxicity. 7 Thereafter, the patient could be evacuated with administration of only WHO level I analgesics and intermittent low-dose ketamine. She was transferred to the nearest level 1 trauma center, where she arrived 40 h after the incident. Radiologic examinations confirmed a distal multifragmentary radius fracture, a displaced clavicle fracture, a displaced fracture of the upper ankle with fracture of the medial malleolus, and a dislocation fracture of the talus (Figure 2). She had also sustained a slightly displaced fracture of the right upper and lower pubic bone and a superficial fracture of the right temporal bone. The injuries were managed conservatively (pelvic ramus and temporal bone fracture) and operatively. The patient recovered partially and was discharged to a rehabilitation center after 11 d.
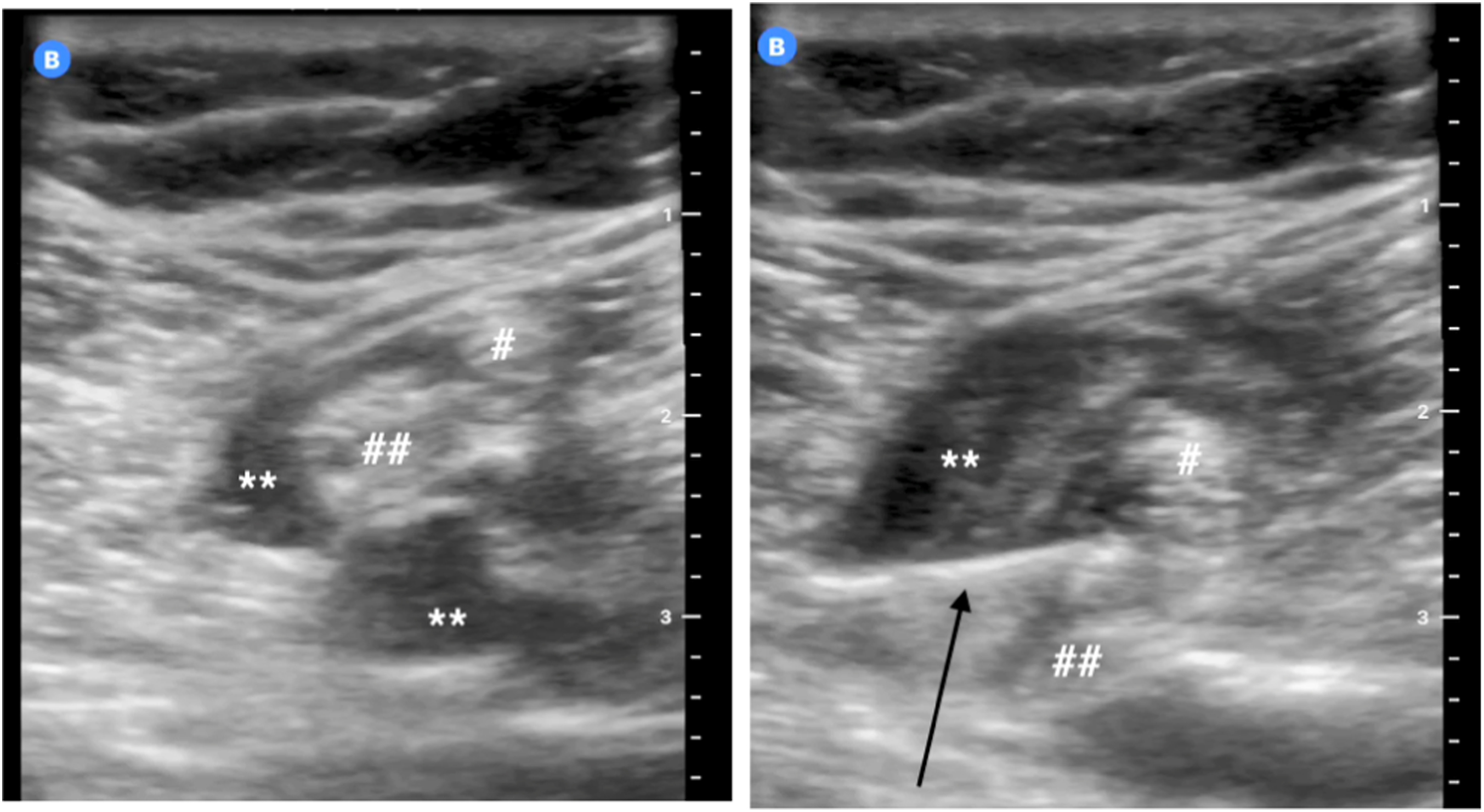
Popliteal block of the first patient with local anesthetics (∗∗) around the peroneal (#) and tibial (##) nerves and injection needle (black arrow).

Computed tomography scan of the first patient showing a dislocation fracture of the talus.
Case 2
During an alpine cave exploration, a 39-y-old speleologist was hit on the pelvis by a boulder weighing several hundred kilograms. The entrance to the cave was located at an altitude of 2000 m. The incident occurred 100 m from the cave entrance, 50 m below the surface. Rescue services could not be notified until 1 h and 40 min later, when another caver reached the surface. The first paramedic at the scene arrived after 6 h and 25 min. The rescuers had to overcome very narrow and winding passages and 3 shafts. Parts of the cave had to be expanded with explosives to bring the stretcher to the patient. The primary survey was unremarkable, but the patient complained of significant pain in the right pelvic area above the greater trochanter. Any movement of the patient was impossible because of the pain. An IV line was inserted to administer paracetamol, metamizole, fentanyl, and antiemetic prophylaxis with ondansetron and droperidol. Even the slightest movement of the patient required additional sedation with ketamine or midazolam. It became clear very quickly that alternatives had to be found to rescue the victim. A specialist physician arrived on the scene 40 h and 40 min after the accident. A handheld wireless US device (EagleView) was used to perform an extended focused assessment with sonography in trauma examination, the result of which was negative (Figure 3). Infrainguinal US-guided (in plane technique with lateral approach) blockade of the fascia iliaca compartment was then performed with fractionated injection of 225 mg of ropivacaine and 150 micrograms of epinephrine. As for the first patient, both intralipids and benzodiazepines were available to readily treat local anesthetic systemic toxicity. Thirty min later, the patient was pain-free and was rescued from the cave, which took 6 h (Figure 4). Upon arrival at the nearest trauma center, a complex right anterior and posterior pelvic ring fracture was diagnosed. The patient was managed conservatively and left the hospital after 6 d.
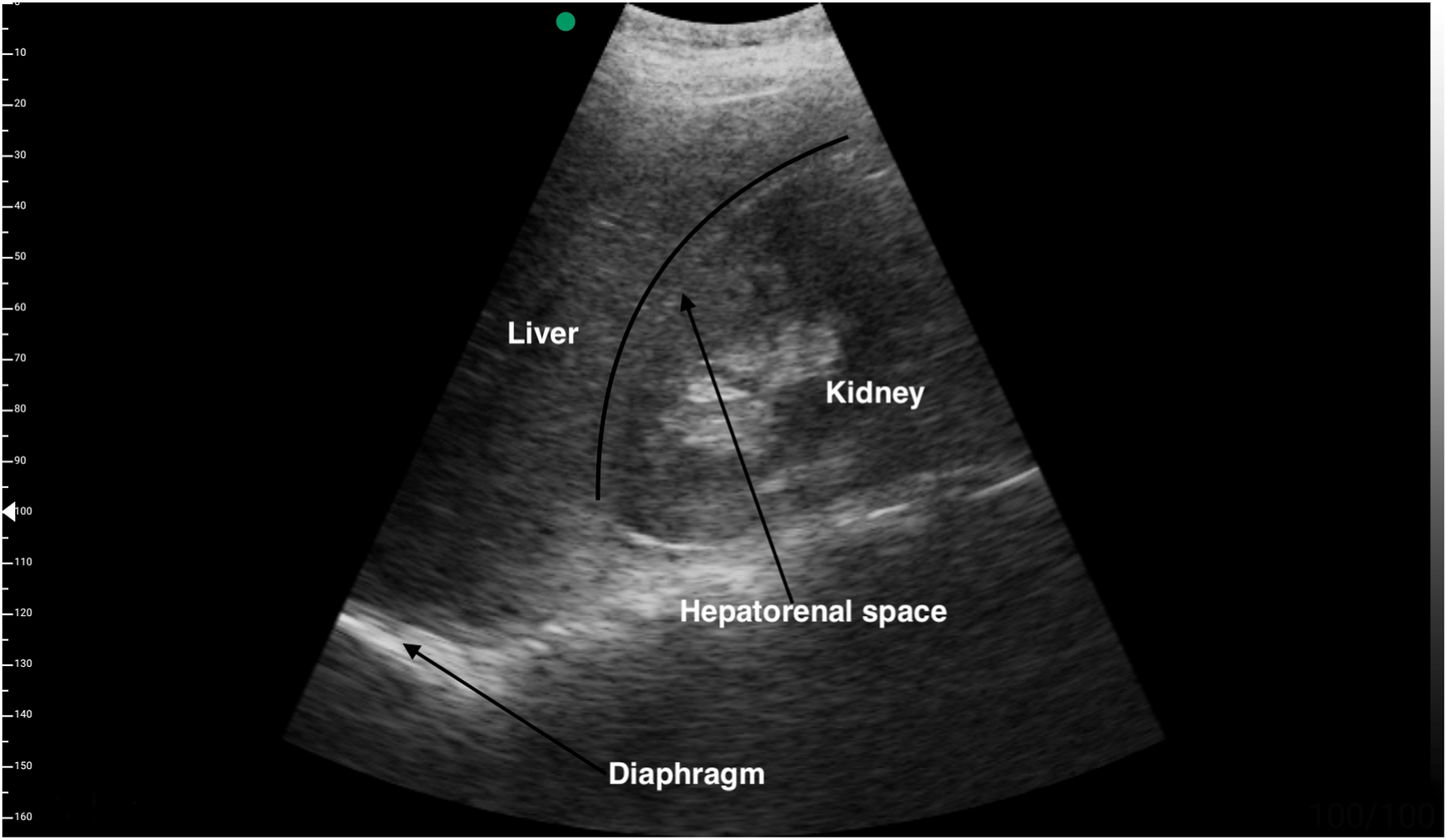
Extended focused assessment with sonography in trauma examination of the second patient showing a normal right upper quadrant view.
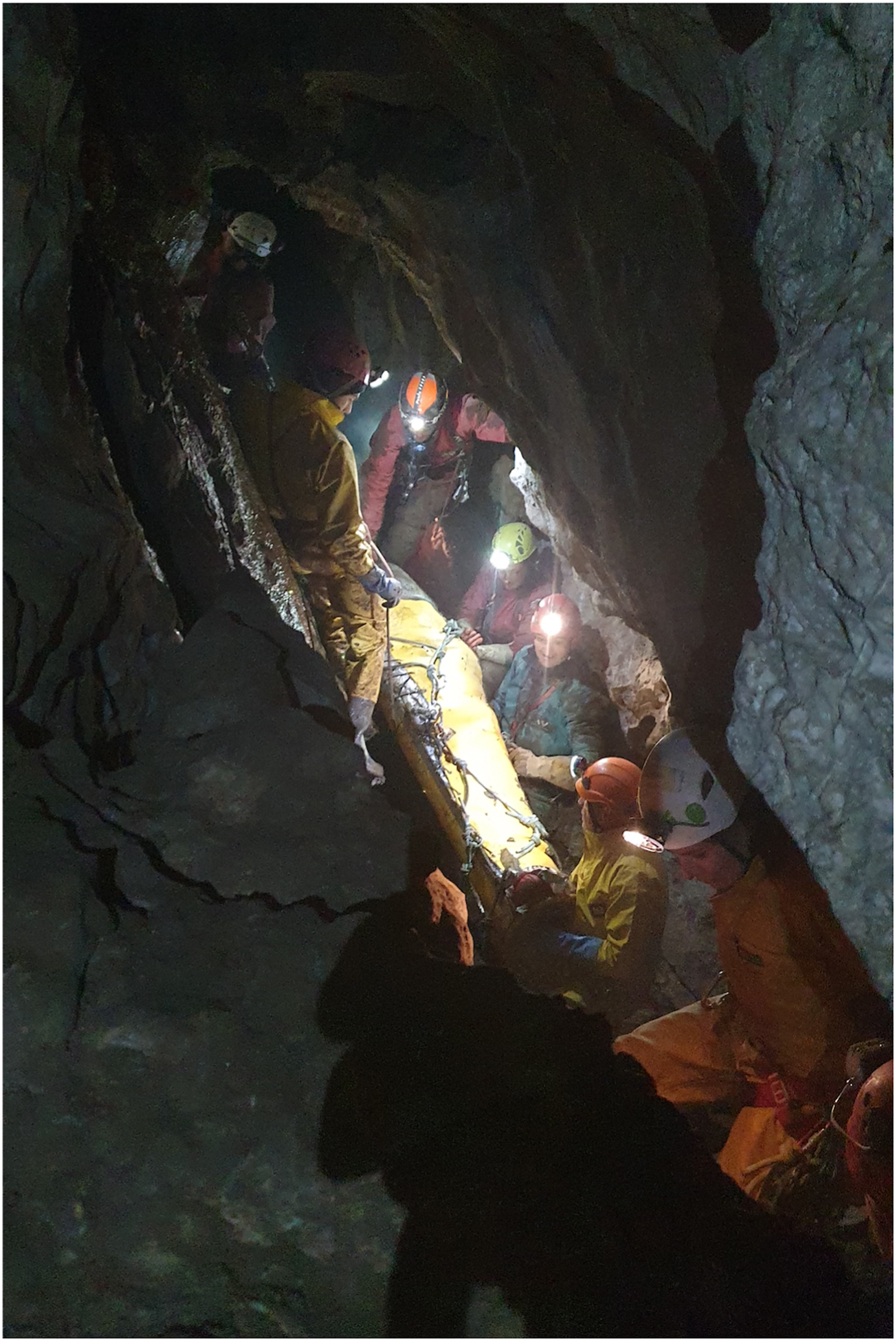
Transport of the second patient. ©Martin Achtmann, used with permission.
Discussion
In this report, we describe 2 cave accidents in which POCUS was successfully used for diagnostic and therapeutic purposes. In both cases, the use of LRA enabled safe and painless rescue of the victims despite very difficult operating conditions. The use of US-guided LRA in cave rescue has been described previously for saphenous nerve blockade. 6 However, unlike our cases, this patient was able to reach the exit under his own power. Our cases show that POCUS-guided LRA can play a key role in situations when patients cannot be moved and extreme rescue conditions prevail.
Cave rescues can be extremely complex and challenging operations and may require several days and involve hundreds of rescuers.4,5 Specific equipment is often required, 2 and the rescue team may face several logistical problems. 6 A thorough initial examination of the victim, including the use of US, can greatly improve medical treatment and increase the likelihood of a good outcome, as has been demonstrated in our cases. The Swiss Cave Rescue Association (Spéléo-Secours Suisse) comprises a team of 6 doctors (ST, AM, KH, SW) and 8 paramedics. 2 Over the last 5 y, we performed 11 rescue missions involving 23 victims. The use of POCUS-guided LRA is not yet standard practice because only 2 of the 6 physicians (ST, AM) are trained in such techniques. The Swiss prehospital organization is a 3-tier system involving dispatch of a prehospital emergency physician to support the management of complex cases, 8 and paramedics are not allowed to perform an LRA blockade. Only a few trained anesthesiologists or emergency physicians perform preclinical LRA at this stage. This explains why, in our second case, the LRA was performed more than 40 h after the incident. Other reasons are the time until the decision to perform the LRA, the time needed to organize the transport by helicopter, the transport time itself, and the time needed to reach the patient.
While it is used daily in perioperative medicine, LRA is used sporadically in prehospital and emergency medicine, although it may be useful in the initial stages of trauma care.9,10 Blockade of the fascia iliaca compartment can be safely performed by practitioners of any background with appropriate training, 11 such as emergency physicians 12 and even other healthcare practitioners, such as paramedics.11,13,14 However, systematic implementation of LRA in prehospital care of trauma patients requires extensive specific training, preferentially in anesthesiology, and structural and logistical modifications. With the advent of high-quality portable US machines that can be readily used in prehospital care, 15 some of the barriers to widespread use outside the hospital setting will certainly be removed.6,16 Prehospital POCUS is not novel, as seen, for example, in Australia (in use since 2007) 17 or in Norway (since 2006). 18 Nowadays, it is becoming more and more common, and in Europe, most helicopter emergency medical services are currently using it. 19 Performed by a skilled person, prehospital POCUS is feasible and provides both diagnostic and therapeutic benefits, improving patient management in trauma, respiratory distress, and cardiac arrest without delaying management.18,20 Not surprisingly, POCUS was defined as one of the top 5 prehospital research priorities in physician critical care. 20
In our 2 cases, POCUS allowed us to both exclude life-threatening injuries, such as pneumothorax and abdominal hemorrhage, and facilitate the patients’ evacuation without the need for additional sedatives or narcotics. This approach may be particularly helpful in situations where continuous monitoring of vital signs and securing the airway prove difficult, especially in nonfasting patients at risk of aspiration. Because evacuation under general anesthesia with intubation is not possible in a cave, the need for alternative analgesic strategies, such as LRA, becomes apparent. Petrucci et al 6 suggest that this approach should be incorporated into trauma care in cave rescues. The combination of diagnostic imaging and US-guided LRA is a valuable asset for making quick diagnostic and therapeutic decisions and may increase patient safety. However, in cave rescues, the timing of LRA must be coordinated with the evacuation procedure so that local anesthesia lasts until the surface is reached. For longer rescue operations, catheter-based approaches may be considered, but to our knowledge, this approach has not yet been evaluated. Finally, rescuers should be made aware of the possibility of using LRA in the prehospital setting under certain circumstances to avoid significant delays, as in our second case.
Conclusion
In summary, our cases show that POCUS-guided prehospital LRA is a safe, fast, and effective procedure that can be used in extreme situations such as cave rescues. The advent of portable, high-quality US equipment will hopefully open the door for broader LRA application in the preclinical setting.
Footnotes
Acknowledgements
Author Contributions: conception and design (AM, SW, KH, ST); literature review (AM, ST); drafting of the manuscript (AM, SW, KH); critical revision of the manuscript (LC, KH, SW, ST). All authors approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.