
Abstract
Introduction
Mountain biking is a fast-growing recreational activity. Electronic mountain bikes (EMTBs) are becoming more common and can attract a different demographic to traditional mountain bikes. The difference in bike design could lead to a differing injury profile. This study examined acute EMTB injuries, an unstudied area.
Methods
A voluntary online survey collected data on EMTB injuries sustained by riders in the Australian Capital Territory and New South Wales. Descriptive statistics were used to analyze injury events.
Results
Over the study period (November 2022–June 2023) 67 injuries were recorded across 46 injury events. The median age of participants was 49 y (range, 20–67 y), and respondents were predominantly male (males 63%, females 35%, other 2%). Common injuries were superficial skin injuries (42%), mainly to the limbs. The study recorded 7 fractures to the limbs and 7 to the head and trunk. Most injuries were sustained from collisions or obstacles (49%). Most occurred traveling downhill (63%) on blue graded single tracks (65%), and 22% injuries occurred whilst traveling uphill. Injury management were spread across self-managed (44%), Emergency Department care (31%) and other health providers (26%). In the 7-d period following the injury 59% of riders experienced moderate to severe pain, and 50% were unable to participate in MTB riding.
Conclusion
Electronic mountain biking participants have a similar injury profile to traditional mountain bikers, but their demographics may differ. More research is needed to determine whether there is increased representation of female and older riders in electronic mountain biking.
Introduction
Mountain biking (MTB) is considered one of the fastest-growing recreational activities around the world.1–3 Memberships of Mountain Bike Australia (now AusCycling), the peak body for MTB nationally, increased by >60% between 2014 and 2019, and bike sale and servicing demands spiked through the COVID-19 outbreaks.1–3 Survey data by AusPlay estimate that nearly 350,000 Australians use mountain bikes and that riders are most likely to be 35- to 44-y-old males riding 1 to 2 h two to three times per week, mostly for recreation. 1
A literature review of traditional MTB injuries found that the most frequent injury sites were the lower limbs, upper limbs, shoulders, and clavicle.4–10 The most frequent injury types were lacerations, abrasions, and contusions.5,6,9–13 Other frequent injuries included fractures, dislocations, strains, and sprains.5,6,10,13 Concussions were reported with higher frequencies in the 2 pediatric studies by Willick et al 10 (23.6%) and Ehn 6 (23.3%) compared with adult-only or combined studies, where concussions or traumatic brain injuries were ∼11% (Romanow et al, 8 12.3%; Ashwell et al, 4 11.2%; and Palmer et al, 13 10.2%). Most injury events were multifactorial, including downhill riding, rider error, poor trail conditions, unforeseen trail obstacles, technical terrain, and pressure situations such as competitions. Most riders reported that more than 1 contributing factor led to the injury event.5,6,13,14
Electronic mountain bikes (EMTBs) have become more common in the community and can attract an older demographic of the MTB population that previously may have been limited by their physical capacity and are now able to participate more fully in the sport.15,16 In addition to attracting a different demographic of riders, EMTBs also differ from traditional mountain bikes in the overall weight and weight distribution through the bike. A review of each of the 4 most recent mountain bikes and EMTBs tested by the Australian mountain biking magazine AMB Magazine indicated a weight range of 14.5 to 18 kg for traditional mountain bikes and 21.1 to 28 kg for EMTBs. 17 The extra weight and some changes in geometry are mainly for the battery and motor, which usually are fitted inside the frame. These provide power-assisted pedaling up to a speed of 25 km·h–1 under Australian law. 18 These differences in bike design and bike riders could lead to a differing injury profile.
There was a paucity of electronic mountain biking-specific injury data. Previous studies of electric-powered bicycle injuries did not specifically examine mountain bikes; instead, they were either unspecified or studied e-road bikes only. However, these studies did show that, overall, more serious injuries were seen in e-road bike users compared with users of self-powered bikes.1,15,16
This cross-sectional epidemiologic study examined acute electronic mountain biking injuries, an area currently unstudied. The results from this study provide insight into the injury profiles of an emerging area of mountain biking. Improved understanding of electronic mountain biking injuries and the riders involved could contribute to improved recommendations for safety equipment and help inform riders, manufacturers, and medical providers of the risks of EMTB riding.
Methods
Study data were collected and managed through an online voluntary survey using the secure web-based software platform REDCap electronic data-capture tools hosted at the University of Tasmania. 19 Written consent was given prior to starting the survey. Data were collected between November 2022 and June 2023. The Human Research Ethics Committee of the University of Tasmania (27398) and ACT Health (2022.LRE.00205) granted ethics approval for the study. The study did not receive any funding, and there were no interventions involving the participants.
Participant inclusion criteria were EMTB riders, 18 y of age and over, who reported an acute injury while riding an EMTB in designated mountain bike parks in the Australian Capital Territory (ACT) or New South Wales (NSW) during the period of the study. Through recruitment on social media or advertisements placed at various mountain biking facilities as well as at the Canberra Hospital Emergency Department, participants were invited to complete a short survey.
The survey included questions on age, sex, location and trail conditions, bike type and protective equipment used, activity at the time of injury, site of injury, injury type, and injury severity. Track terrain was based on the mountain bike trail difficulty rating system guidelines, with green trails classified as easy and suitable for beginner cyclists with basic mountain biking skills, blue trails for intermediate mountain bikers, and black trails for experienced mountain bikers. 20 We used the STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS) 21 to collect injury type and location data and a modified Oslo Sport Trauma Research Center Questionnaire 22 to collect injury severity data. Analysis of deidentified data was completed on the REDCap platform or Microsoft Excel. Statistical analyses were presented as frequency for descriptive data and mean for numerical values.
Results
Over the 8-mo study period (November 2022–June 2023), 67 injuries were reported across 46 injury events. The demographics of the 46 respondents were predominantly males (males, n=29 [63%]; females, n=16 [35%]; other, n=1 [2%]) with a median age of 49 y (range, 20–67 y). Thirty-nine participants were working either casually or part or full time. One participant was a student, and 6 identified as either retired or not working.
All respondents in this survey were riding EMTBs, with 40 dual-suspension frames (87%), 5 hardtail frames with only front suspension (11%), and 1 rigid frame with no suspension (2%). Suspension helps absorb impact on technical trails and can improve comfort and stability. Five respondents reported that they had made modifications to override the speed limit on their bike, but it was not identified whether speed was a factor in the injury event.
Participants wore a range of protective equipment, including helmets (n=46; 100%), 17 of which were full face (37%); gloves (n=39; 85%); knee pads (n=21; 46%); eye protection (n=20; 43%); elbow pads (n=15; 33%); shin protectors (n=5; 11%); a chest brace (n=1; 2%); a neck brace (n=1; 2%); and an ankle brace (n=1; 2%). Of the 24 respondents wearing knee, shin, and/or elbow pads, only 2 reported injuries to those protected areas—both were superficial abrasions. There were 6 injuries, all superficial abrasions, to either the knees, shins, or elbows where protection was not worn.
Ride Type and Terrain
The study recorded injury events in NSW (n=30), some of which were in the area immediately surrounding the ACT (n=4), and the remaining were in the ACT (n=16). Most events occurred during recreational rides (n=43; 93%), 1 during a coached session (2%) and only 2 occurring during competition (4%). Across the 46 injury events, 67 unique injuries were reported. Four participants (9%) had 3 unique injuries; 13 participants (28%) reported 2 unique injuries; and 29 (63%) had a single injury.
Track terrain were mainly blue single track (n=30; 65%), with 4 injury events on black graded trails (9%), 7 on green trails (15%), and 5 on ungraded trails (11%) such as gravel roads (n=2; 4%) or a rail trail (n=1; 2%). Most injury events occurred while riding downhill (n=29; 63%), with 7 on flat terrain (15%) and 10 while riding uphill (22%).
Contributing factors that were cited included obstacles such as rocks or tree roots (n=19; 41%), landing from a jump (n=7; 15%), collision with a person (n=2; 4%), collision with a natural object (n=2; 4%), unknown (n=5; 11%), and other (n=11; 24%). The responses to “other” included 6 related to slipping on wet/muddy/loose surfaces, 3 related to incorrect riding on a technical feature, and 2 responses described the cause of the accident to be speed.
Injury Location and Type
Injuries occurred predominantly on the limbs (lower limbs, n=24 [36%]; upper limbs, n=22 [33%]; Table 1). On the trunk, only chest injuries were reported (n=8, 12%). None of these participants were wearing chest armor. There were 3 head and neck injuries (head, n=2 [3%]; neck, n=1 [1%]), and all riders were wearing helmets but not neck braces. There were 8 reports (12%) of a single injury that crossed multiple areas of the body, and 2 of the reported injuries did not specify the injury site (3%).
Injury type and location.
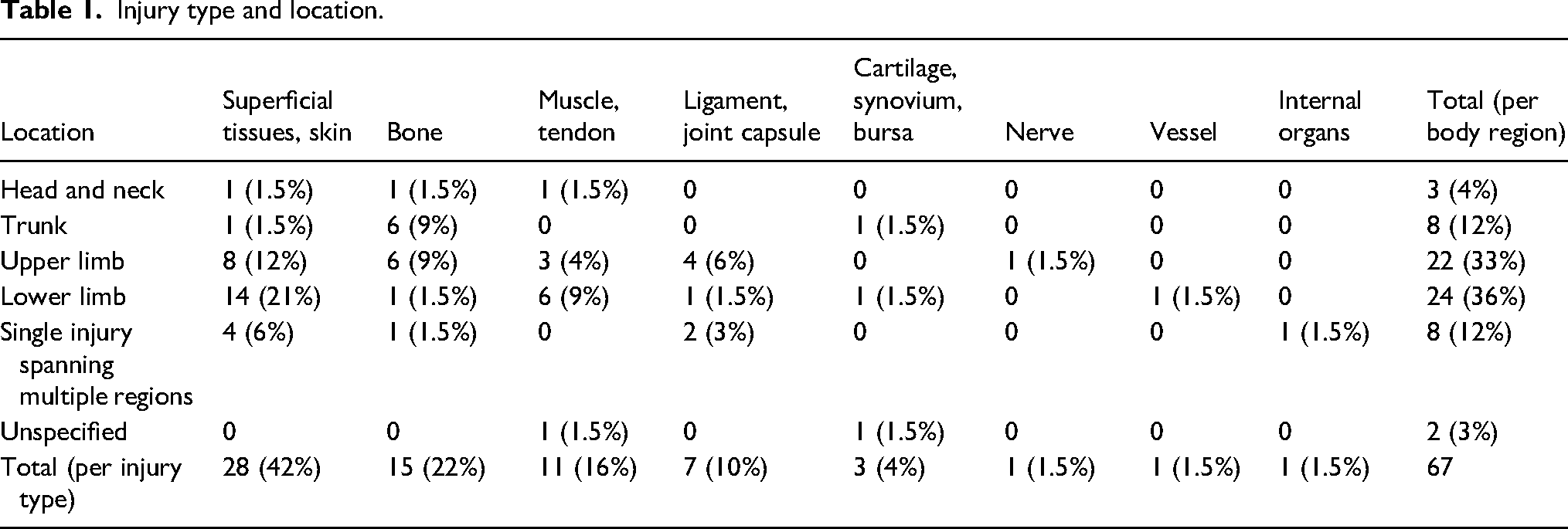
The most frequent injury type were superficial skin injuries (n=28; 42%), which included abrasions (n=11; 16%), contusions (n=9; 13%), and lacerations (n=8; 12%). These injuries occurred most frequently on the lower limbs (n=14; 21%) and upper limbs (n=8; 12%). Of the 28 skin injuries, 9 occurred in locations where protection such as pads or armor were possible but not used. The second most frequent injury type was bone injuries (n=15; 22%), with 6 rib fractures (9%) and 5 wrist fractures (7%). Chest armor was not worn by any of the participants with rib fractures. There were 11 reported muscle injuries (16%), with 9 occurring on the limbs (13%) and 1 neck musculature injury (1%). There were 7 ligamental injuries (10%), n=2 (3%) for the shoulder, n=2 (3%) for the hands/wrists, n=2 (3%) across multiple areas, and n=1 (1%) for the foot. Other injuries were 3 cartilage injuries (4%), n=1 each (1%) for the chest, groin, and unspecified; 1 internal organ (1%); 1 vessel in the thigh (1%); and 1 shoulder nerve injury (1%). Table 1 outlines the injury type by injury location.
Injury Management and Follow-on Impacts
Of the 46 survey respondents, 42 completed questions on injury management and the impact of the injury event on their participation, performance, and pain in the 7-d period following the injury. Injuries were most frequently self-managed (n=18; 43%), followed by management in an Emergency Department, either brought in by private vehicle (n=12; 29%) or by ambulance (n=1; 2%). Follow-up with healthcare professionals included 4 general practitioners (10%), 3 physiotherapists (7%), 1 nurse (2%), 1 orthopedic surgeon (2%), and 2 other health services (5%).
For at least the next 7 d after the injury, 21 of the riders (50%) were unable to participate in mountain biking, 11 (26%) had reduced participation, 3 (7%) could participate but with injury-related problems, and 7 (17%) were able to continue full participation without injury-related problems. Of the 21 who were unable to participate, 9 (21%) reported bone injuries, 9 (21%) had tendon/ligament injuries, 2 (5%) reported superficial skin injuries, and 1 (2%) had a nerve-related injury. Twenty-three riders (55%) reported that the injury affected their performance to a major extent, with 17 of those (40%) not being able to perform. Only 5 riders (12%) reported that the injury would not affect their performance.
Expected or experienced pain was reported in a high frequency of the survey results. Severe pain was reported by 8 riders (19%), moderate pain by 17 riders (40%), and mild pain by 15 riders (36%). Two riders did not report any pain associated with their injury event (5%).
Discussion
This study-reported injury types, locations, and severity were in line with traditional mountain bike riders. The differences in bike design between EMTBs and traditional mountain bikes did not have a significantly impact on injuries. The demographics of participants in this study were different from those in comparable MTB studies and could indicate that EMTBs attract a different cohort of riders.
The participants in this study tended to be older (median age 49 y) than those in similar traditional MTB injury studies on people aged 16 y and older (median ages 28 and 29.3 y).14,23 There also was a higher frequency of females (35% vs 10–26%).7,8,10,11,13,14,23,24 This could be due to a higher proportion of injuries in these demographics or higher participation on Facebook, which was the main platform to advertise the study. Another possibility is that mountain bike riders are overwhelmingly male, and emphasis on skill and speed is often used as an indicator of experience and performance. Studies into the barriers and experiences of females and beginner males in the sport often cite concern about “not being able to keep up with the guys” as a negative factor in their participation.25,26 The higher response rate of female and older riders in this electronic mountain biking study may be because powered bikes are more appealing to these demographics because concerns about speed may be diminished. As an emerging discipline of mountain bike riding, this identifies an unexplored opportunity to understand the perceived benefits and appeal of EMTBs to female and older riders that may provide an opportunity to increase diversity in the sport and increase lifelong participation in physical activity.
The data collected for this study on contributing factors to injury events were comparable to the data collected by traditional MTB injury studies.4–10 The most frequently reported injury types (Table 1) were superficial skin injuries, including lacerations, abrasions, and contusions (42%); bone injuries (22%); and other musculoskeletal injuries combined (30%). No concussions were reported in this study, which is different from other comparable adult studies, where concussions averaged 11%.4,8,13 All riders wore helmets in this study, but helmet use is widespread in MTB, and although it was not specifically reported in all comparable studies, it is unlikely that helmet use alone can account for the lower frequency of concussions in this study. The most frequently injured sites were on the lower and upper limbs. This is consistent across all comparable studies, although the frequency distribution of specific body areas within the upper and lower limbs varied across the studies.4–10
The injuries occurred across a variety of terrains, with the highest frequency occurring on blue single track while riding downhill. Injury type, number of injuries, and severity were not related to event type, trail terrain, or difficulty. These injury types, sites, and terrain were in line with other similar traditional MTB studies, which also reported the main causes of injury as rider error and adverse or technical trail conditions.4,6,10,23 A point of difference with this study was the higher frequency of injuries occurring while riding uphill (21% vs 6%).6,10
The heavier weight of EMTBs was not a clear contributing factor to any of the accidents reported in this study. High speed, however, was reported as the main contributor to 2 of the downhill accidents in this study, but it was not specifically reported whether pedal assistance was activated at the time. From this study it was not possible to determine whether the weight and higher speed potential of EMTBs were specific causes of injury. The data collected on injury severity also were comparable with those of traditional MTB, which contrasts with studies on e-road bikes, which showed that, overall, there were more serious injuries by e-road bike users compared with self-powered bike users.1,15,16
Musculoskeletal injuries made up 52% of all injuries reported in this study. All Emergency Department presentations and 73% of general practitioner or allied health presentations were for musculoskeletal injuries. There were 8600 hospitalizations in Australia attributed to cycling for sport in 2021–22, and fractures accounted for 58% of those hospitalizations. 27 The healthcare burden of hospital-treated cycling injuries in Australia in 2018–19 was $52 million. 28 To reduce the burden on the individual and the population-level health burden, a focus on prevention of injury or reduction of severity of injury is key.
All participants in this study wore helmets, and most wore gloves (n=39). Despite a high incidence of limb injuries, however, fewer than half of the participants wore knee pads (n=21; 46%), shin pads (n=5; 11%), or elbow pads (n=15; 33%), which may have prevented or reduced the severity of some of the reported injuries, mainly lacerations and abrasions. The highest-frequency fracture sites were ribs and wrists. Only 1 respondent, who had a lower limb injury, reported that they wore chest armor, which may decrease the risk of rib fracture. There are some options for wrist protection for mountain bike riders, but it is not clear whether these products have been adequately tested for effectiveness. Future research on the effectiveness of protective equipment for the most common MTB injuries could help prevent future injuries.
Limitations
There were several limitations to this study, particularly in the areas of recruitment, participation, and survey design. Recruitment was mainly through targeted posts onto ACT- or NSW-based electronic mountain biking Facebook groups (n=35; 76%), some of which identified as female-only/female-targeted groups. No information was collected on the number of members in each of these Facebook groups, the genders of the members in the groups, or the reach of each post. Different social media platforms are known to attract different demographics, and the use of Facebook as the only social media platform for this study may have had an impact on the demographic of the participants compared with the general electronic mountain biking population. Six of the participants were recruited via posters that were only displayed at mountain bike parks in the ACT and at the Canberra Hospital Emergency Department, which accounts for 50% of all responses within the ACT. Two also were recruited through in-person recruitment at an ACT MTB facility. The median age of these 8 participants was 40 y, and females were 30%, which are both less than the participants recruited through social media (median age 49 years, females 37%).
Participation in this study involved voluntary completion of an online survey covering an injury that occurred anytime during the study period. The limitation of self-completed surveys include potential recall bias of the event due to misremembering, forgetting, or not knowing specific details. Knowledge of medical terminology also could have impacted the accuracy of the injury site sand types reported. This would be especially true in self-managed injuries who may not have received a formal diagnosis. The impact of the injury on the rider also may be inaccurate if it was reported prior to 7 d after the injury.
In addition to errors in reporting the injury event, there also was potential for nonresponse bias, which could underestimate injury prevalence. Another limitation was that exposure was not reported. The survey did not include any questions on rider experience or capabilities or how many hours the rider had ridden their EMTB in a mountain bike park within the timeframe of the study. Exposure was not included in the survey because responses were taken throughout the study period rather than after the study period had passed.
Conclusion
This study of EMTB injuries recorded a higher frequency of female and older riders compared with studies of traditional MTB injuries due to possible recruitment bias. Because females are traditionally poorly represented across all disciplines of mountain biking, however, further studies into barriers to female participation may provide valuable insight into increasing female participation in electronic mountain biking and the sport overall.
In this study, electronic mountain biking injuries were comparable in injury type and location to traditional MTB injuries and occurred due to similar factors such as obstacles, collisions, and slippery surfaces. Injuries occurred across a variety of terrains, most commonly on blue-rated single tracks while going downhill. The injuries were not more severe compared than those in traditional mountain biking, which is not the case for other e-road bike studies.
Most riders did not wear protective gear for the most commonly reported injury sites (ie, limbs and trunk). Research into barriers to the use of protective equipment, as well as promotion of the use of protective equipment options in the sport, may help reduce further injuries and reduce the healthcare burden of these sporting injuries.
Practical Implications
Riders of EMTBs tend to be older than in other MTB disciplines, and EMTB riding may be an opportunity to retain people in the sport for longer. EMTB riding may attract a greater proportion of female riders, who traditionally have been poorly represented in the sport. Electronic mountain biking injuries have a similar injury profile (location and type) to traditional MTB injuries. Most riders, however, do not wear protective equipment that may prevent injury or reduce the severity in these areas.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Accessibility Statement
The data collected in this study can be shared on reasonable request. Shared data would require proof of secure repositories for storage, and data would be anonymized prior to sharing. Data should be cited in any future research.