
Abstract
Objective
To describe the epidemiology of injuries sustained in cyclists and compare the injury patterns in road vs trail biking accidents.
Methods
A retrospective chart review was performed of injured road and trail cyclists presenting to a rural mountain resort–based medical center during a 3-year study period.
Results
Of 304 patients, 70% were male, with 67% sustaining trail injuries and 33% sustaining road cycling injuries. There was a bimodal age distribution. Prehospital care was activated in 16% of patients. The most common injuries were lacerations and abrasions (64%), upper extremity fractures (26%), head injuries (9%), and thoracic trauma (6%). Head injury was more common in road- vs trail-related trauma (16% vs 6%; P = .005), whereas thoracic injury was more common in trail riders (7% vs 2%; P = .053). Head injury and lower extremit y fracture were the most common reasons for patient transfer. Patients with head injuries who did not use a helmet were more likely to require transfer to a neurosurgical unit (38% vs 17%; P = .296); however, this difference did not meet statistical significance.
Conclusions
Lacerations and abrasions are the most common injuries sustained in cycling. Quantifying the role of protective extremity gear in reducing these injury patterns may be of interest for future studies. Protective helmet use may be important in reducing morbidity from cycling-related head trauma; however, more data are needed. Prehospital care providers responding to the injured trail cyclist should be equipped to manage laceration, fracture, head injury, and thoracic trauma in the field.
Introduction
Since its inception in the early 1970s, the sport of mountain biking has grown significantly as a recreational and competitive sporting activity. In 2013, 8.5 million Americans participated in mountain biking, up 20% from 2007 with more than 2.7 billion mountain bike outings per year. 1 The popularity of this style of riding has been bolstered by the development of lift-accessed terrain at ski resorts during summer months, increasing the frequency and access to steeper, longer, and more technical mountain terrain. Currently there are more than 50 North American ski resorts that offer lift-accessed mountain biking trails, with more scheduled for development. 2
As the sport of mountain biking has grown, there has been increased recognition of the risk these activities pose. 3 Data regarding injury patterns and epidemiologic trends have been conflicting as regional data demonstrate increased injury frequency, whereas national estimates point to a decrease in injury frequency during the past decade. 4 –6 Although most injuries are considered minor, approximately 80% of professional and 50% of recreational athletes report at least 1 severe mountain biking-related injury. 7
Injury data for road cycling have led to improvements in cycling safety; however, these data may not extrapolate to mountain biking injuries given the varied terrain and mechanism of injury. 8 Understanding the injury patterns associated with mountain biking could lead to improvements in preventive and protective strategies. The purpose of this study was to provide a comparative population-based review of injury patterns (road and trail) resulting from cycling accidents.
Methods
The Telluride Medical Center (TMC) provides emergency medical services for a catchment area of greater than 1200 square miles. In the region there are hundreds of miles of mountain bike–accessible trails and more than 50 miles of lift-serviced mountain biking trails within the Telluride ski resort. In addition, there are numerous scenic road cycling routes, with significant climbs and elevation change, that are frequented by day and multiday cyclists. All cycling injuries in the catchment area that required hospital-based medical care were provided at TMC.
A retrospective chart review was performed for all patients presenting to TMC between June 2012 and June 2015. All patients presenting to TMC during the study period were screened for ICD-9 injury E-codes corresponding to a cycling-related injury (E826, E006). Patients injured while riding on pavement were classified as “road injuries,” and patients injured while riding on trail, dirt, or gravel were classified as “trail injuries.” The type of bicycle and sport-specific mechanism was not considered. Demographic and injury pattern data were classified based on ICD-9 coding, physician diagnosis, and review of the physician narrative. More than 1 type of injury classification for each patient was permitted. Clavicle fracture and acromioclavicular separation were included in upper extremity fracture groupings. There were no bicycle-related deaths during the study period.
Data were extracted for each case meeting inclusion criteria using a standardized data extraction tool. Patients with the following histories were classified as having comorbid medical conditions based on physician data extraction (hypertension, diabetes, ischemic heart disease, congestive heart failure, chronic renal disease, chronic lung disease, peripheral vascular disease, or active cancer treatment). Deidentified data were entered into Filemaker Pro (version 10.0v3, Santa Clara, CA) and analyzed using the Statistical Package for the Social Sciences (SPSS version 22, IBM Corp, Armonk, NY). Comparison of categorical variables were made using χ2 or Fisher exact test for proportions. A probability value of less than .05, 2-tailed, was considered significant. The medical staff and ethics committees at the TMC approved the study.
Results
During the study period, 10,215 emergency department (ED) visits were screened. Of these, 4127 were during the summer months. Of 316 cases (8% of summer ED visits) that met case definition criteria, 304 had complete records and were enrolled. Of the 304 cases, 70% were male, and age distribution was bimodal in nature (Figure). Younger injured riders were predominantly male, whereas the older group was less skewed according to sex. The majority of injuries in the cohort (67%) occurred while trail riding. Summary data regarding injury pattern and disposition are presented in Tables 1 and 2.
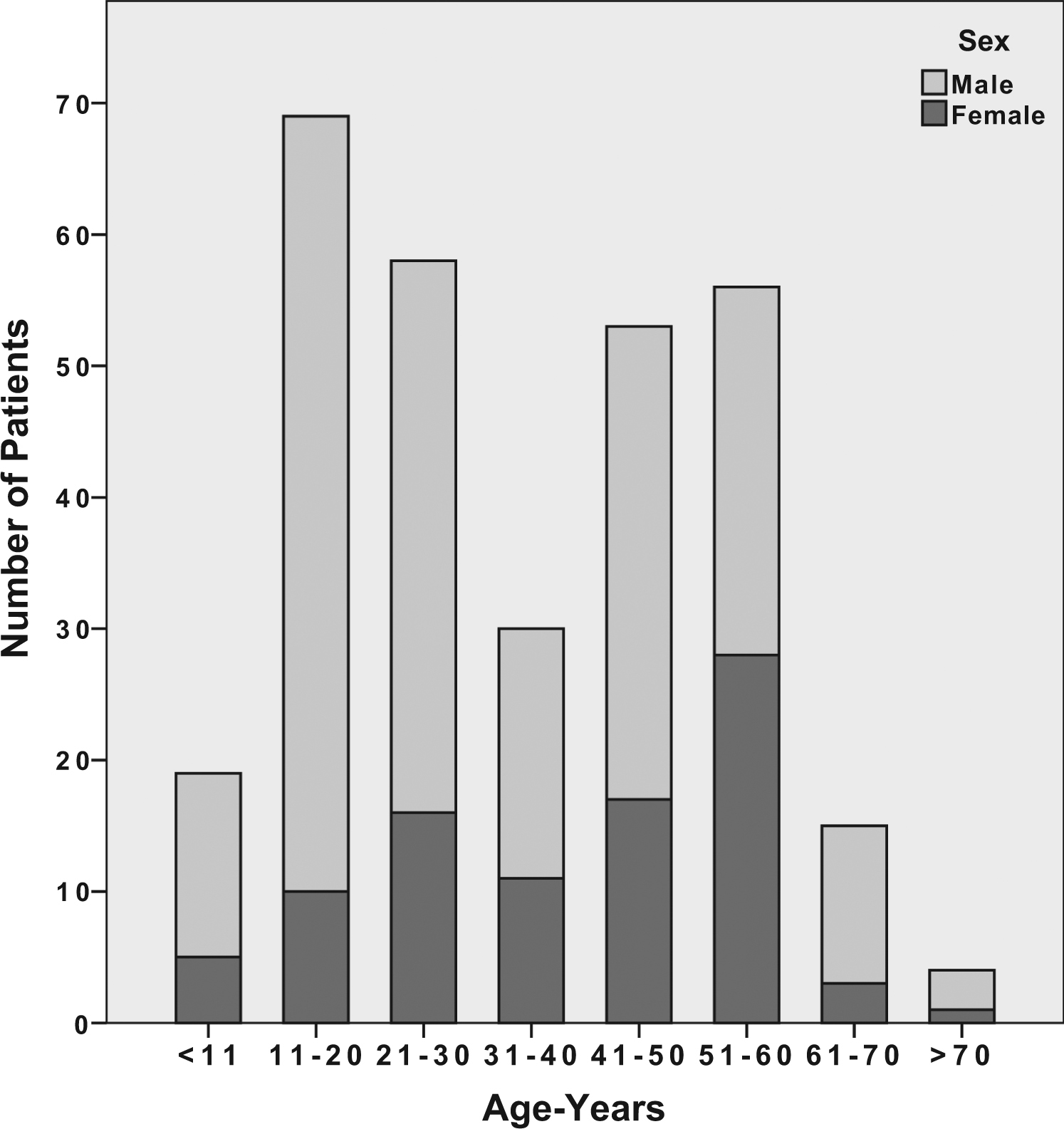
Age and sex distribution of enrolled patients.
Enrolled patient demographics
Proportion of patients receiving prehospital care, requiring transfer to higher level of care and having underlying medical comorbidities in trail vs road cyclists, reported as number (%).
Comparison of trail vs road cycling injury patterns
Values are number (%).
χ2 or Fisher exact testing.
A comparison of injury patterns in road- vs trail-riding patients is presented in Table 2. Trail injury was more common in male patients. Patients were more likely to sustain head injury while road riding and were more likely to sustain thoracic injuries on trails. Given the bimodal age distribution of injury, comparison of injury patterns was conducted based on division into 2 groups by median age (33 years; Table 3). Older riders made up nearly all of the thoracic injuries and were evenly distributed by sex, whereas younger riders were predominantly male. Rate of transfer did not differ in the 2 age groups.
Comparison of injury patterns and need for emergency medical services and transfer in young vs old age groups
Values are number (%).
χ2 or Fisher exact testing.
Of the 20 patients requiring transfer to a higher level of care, the majority were because of head injury (40%) and lower extremity fracture (35%; Table 4). Injuries sustained while road riding were more likely to require transfer as a proportion of the total (9% vs 5%; P < .05). Of 28 patients with a head injury, 12 were helmeted and 16 were not helmeted. Six of 16 patients not wearing a helmet (38%) required transfer for management of their head injury, whereas 2 of 12 patients wearing a helmet (17%) required transfer for management of head injury. This difference was not statistically significant (P = .296).
Injury pattern, mechanism and need for prehospital care in patients requiring transfer to a higher level of care
Discussion
In this report, the injury patterns and epidemiology of cycling injuries occurring during a 3-year period in a mountain community are described. More than 8% of ED summer visits were for bike-related trauma in this cohort. The majority of injuries occurred in males (70%) and while trail riding (67%). This is consistent with other studies citing rates of 71% to 86% male predominance. 4 –6,9–11 Few patients had underlying comorbidities (3%), and prehospital emergency medical services (EMS) were dispatched in 16% of cases. The rate of EMS transport was notably higher in this population (16%) than that cited in the Whistler bike park population (8.4%). 6 This may be related to the relative proximity of a bike park to vehicular transport, in comparison to a predominantly backcountry trail network in this cohort, where self-extrication may have been more difficult to accomplish.
The vast majority of injuries sustained were lacerations, abrasions, and contusions (64%), with upper extremity fractures making up the remaining majority (26%). Injury pattern data for trail- vs road-biking injuries were similar except for a higher proportion of head injury in the road cohort and thoracic injury in the trail cohort, likely related to differences in mechanism of injury. Fracture patterns were similar to other reported studies with regard to upper and lower extremity distributions. 6 ,7,10,12 In this cohort, lacerations and abrasions were more frequently observed, likely representing more inclusive reporting as other epidemiologic studies have focused on narrower cohorts such as trauma center admissions or racing- and bike park–related injury patterns. 4 ,6,10–12
The role of protective equipment in mitigating sports-related morbidity is highlighted by the debate and history of protective helmet use in cyclists and skiers. Although slightly controversial, data on helmet efficacy in the past 2 decades have spurred a major increase in protective helmet use, with many ski areas and downhill terrain parks requiring the use of helmets in certain rider and cyclist groups.13,14 With the further quantifying of the associated risks and injury patterns in mountain cyclists, the role for protective knee and elbow equipment may also come to the forefront of discussion in injury prevention. Although not reported in this study, many of the lacerations sustained in trail cyclists are complex, contaminated, and frequently on the knees and elbows. Future investigation should seek to characterize the role of protective knee and elbow equipment in trail cyclists, as the promotion of protective knee and elbow equipment may have a role in injury prevention.
Because the study facility does not support inpatient services, all patients requiring admission were transferred, with approximately 7% of all biking injuries requiring admission or transfer. Of the transferred patients, the majority were because of head injury or lower extremity fracture. Of the 28 patients with a head injury, 17% of those wearing a helmet required transfer vs 38% of those not wearing a helmet who required transfer for inpatient management of head trauma. This difference was not significant, and is likely a function of the small sample size in this subgroup. Larger case-control studies have demonstrated a similar efficacy (relative risk = 0.3–0.6) for reduction of severe head injury with hard helmet use in cyclists.13,14
Limitations
The global applicability of this study may be limited because the population and mechanism of injury may be different based on terrain and human subject variables. More specific data regarding mechanism of injury were not available and may have been useful for further characterizing injury patterns. The retrospective methodology used may limit the breadth of injury pattern data that are uniformly available in the medical record.
Conclusions
The vast majority of injuries occurring in road and trail cyclists were lacerations, abrasions, contusions, and upper extremity fractures. Quantifying the role of protective extremity gear in reducing these injury patterns may be of interest for future studies. Protective helmet use may be important in reducing morbidity from cycling-related head trauma. Prehospital care providers responding to the injured trail cyclist should be equipped to manage laceration, fracture, head injury, and thoracic trauma in the field.