
Abstract
As the field of health and medicine in space develops alongside the spaceflight research paradigm, there are methodologic opportunities to integrate data collection for research with providing precision and personalized healthcare. Specifically, existing field methods in biological anthropology developed and practiced in austere settings can be translated to spaceflight research and the development of healthcare infrastructure with implications for space medical practice. In our era of expanding spaceflight, data-collection methodologies should be flexible, agile, and accessible, paralleling innovative strategies by biological anthropology field researchers assessing human health, behavior, and well-being in austere terrestrial settings. Here we offer an introduction to the methodologic approaches and theoretical frameworks from biological anthropology, including operational insights from investigators working in the field, highlighting flexible mixed methods, low-tech solutions, dialectic engagement with participants, and iterative research protocols. These tools, when performed together with standardized approaches, can be beneficial and augment the advancement of spaceflight health and medicine.
Keywords
As the spaceflight research paradigm expands, there is an increased call for precision and personalized approaches to space health and medicine,1–6 where there is a focus on individual genetic, environmental, and lifestyle variability and accounts for context-specific responses. During the recent decades of active spaceflight primarily under the purview of government agencies (ie, the National Aeronautics and Space Administration and the European Space Agency), a select group of individuals could be carefully and intensively monitored and provided specialized care. However, with the growing presence of commercial ventures, research in spaceflight may look more like work conducted in expeditionary and austere terrestrial settings. 7 As such, spaceflight data-collection methodologies should be flexible, agile, and accessible, allowing for precision medical capabilities, paralleling existing frameworks used by biological anthropology field researchers assessing human health and behavior in austere terrestrial settings.
Biological anthropology uses methodologies familiar to space health research but provides theoretical perspectives and operational practice that are directly translatable and can augment existing space medicine work. Anthropology, the study of humans and their societies, past and present, consists of 4 main subfields that drive the discipline. These subfields include archaeology and linguistic, cultural, and biological anthropology. Many anthropologists use a combination of these subfields—as well as the methods and theories from them—to inform their research designs and approaches. Because of the vastness of the discipline, here we focus on biological anthropology and what it offers for space medicine and health.
Key concepts in biological anthropology include using an evolutionary framework, an emphasis on human biology, and a biocultural perspective. Biological anthropologists who use evolutionary theory to inform their research focus on how variability and adaptations shape reproductive success and survivability.8,9 Human biology encompasses a holistic approach to the study of human health and well-being, with explicit focus on the human body, including anthropometric and physiologic measures of health across time and space.10,11 Drawing on methods and theories from both biological and cultural anthropology, biocultural anthropologic perspectives examine human biology embedded within a social or cultural context; a biocultural approach thus is used in any study of human origins, human ecology, adaptation, psychosocial stress, nutrition, and variations in health within a particular cultural context or human population.12–14 Using these perspectives, biological anthropologists can examine how the social, physical, environmental, and cultural conditions of human beings impact their biology, making waves in their short- and long-term health and longevity.15,16 Examples of this biological embodiment of social and cultural conditions include reconstructions of how humans have adapted to conditions in the past,17,18 examinations of differences in health outcomes due to lived experiences across the life course,19–22 and investigations of how social and cultural contexts shape physiology and behavior via psychosocial stress pathways.13,23–25
Since the advent of spaceflight, human research and space medicine have used methods to capture the varied physiologic and psychological states and, more recently, genetic and epigenetic changes that occur before, during, and after being in the spaceflight environment or analogues thereof.7,26–29 Space clinical medicine includes evaluating human response to spaceflight, spaceflight metabolism and nutritional support, space and entry motion sickness, acute care, decompression-related disorders, medical considerations of extravehicular activity, renal and genitourinary concerns, musculoskeletal response, physical performance, immunology and microbiology, cardiovascular response, neurologic response, gynecologic and reproductive considerations, behavioral health and performance, sleep, circadian rhythms, fatigue management, spaceflight pharmacology, ophthalmologic concerns, dental concerns, and environmental factors such as operational environments and life support systems.27,30,31 The operational setting necessitates that space medical practice rely on telemedicine, self-collection, and an individualized/personalized perspective. Importantly, while data have been collected for human research and space medicine in tandem since the beginning of the space program, they are not necessarily a shared resource.32,33 The lack of overlap between medical data for space patients and accessible personal health data for research purposes is a challenge, although necessary given the heightened privacy demands and requirements with such a limited sample size and very real concerns of revoking flight readiness due to health-related issues. Thus, there is an increased call for the use of a systems medicine approach, similar to the work done in biological anthropology, that could integrate research collection with medical practice and healthcare infrastructure.6,7,34,35 Anthropologic approaches provide a theoretical framework and methodologic expertise for integrating medicine and research. These approaches include accounting for evolution as well as sociopolitical, economic, and cultural contexts undergirding the contexts shaping health and performance, genetic and lifestyle predispositions, and personalized life histories that physicians know to be so critical to treating their patients.
At its core, biological anthropology inherently values evolutionary, social, critical, and political economic perspectives to study the holistic influence these structural and systemic factors interplay on human biological characteristics and individual and population health outcomes. Methodologically, biological anthropologists pull from the fields of morphology, genetics, physiology, and ecology, among others, for quantitative data collections of biological specimens and use evolutionary human biology and biocultural perspectives—often with mixed qualitative and ethnographic approaches—to inform these data for a more critical examination of human health and well-being. This lends to a mixed- rather than a multimethod approach; biological anthropologists use and incorporate mixed methodologies into their research designs, approaches, and analyses to interpret the data into more meaningful and holistic insights into the many facets of human health and well-being. The use of mixed methodologies (ie, various lines of qualitative and quantitative data in analysis that speak to each other) over multiple methodologies (ie, singular qualitative or quantitative data in analysis) can extend the work being done particularly in austere settings.10,36
We aim to showcase how mixed methodologies and perspectives of biological anthropology may integrate with the already defined spaceflight health paradigm into a more adaptable and complex enterprise to better the advancement of space health medicine and spacefarer well-being. Here we also present case studies from 3 different field seasons with personal accounts from principal investigators to highlight different aspects of field methodologies in austere environments. Biological anthropology perspectives from existing field research approaches paired with these operational insights can be translated to the space medicine domain and contribute to future work in building precision space health and medical infrastructure.
Biological Anthropology: Research and Contributions to Health Systems
The perspective and preventative aspects of integrating biological anthropology in medicine can provide long-term health modeling and contribute to the development of lasting medical infrastructure. Anthropology has long examined how the human body and mind adapt to novel and extreme conditions.10,36 Foundational biological anthropology work on populations living at high altitude provided evidence of differences in hemoglobin concentration and percent of oxygen saturation constituting population-level phenotypic variation in adaptation to hypobaric hypoxia.37,38 Incorporating the core biological anthropology frameworks examining genetic and environmental influences on health (ie, the developmental origins of health and disease) has shed light on epigenetic effects of social disparities on cardiometabolic health outcomes across the life course.39,40 Similarly, the exploration of changes in biosocial pathways during economic transitions highlights how sociocultural stressors can affect intergenerational health.41–43 Other established human biology projects with underserved and remote communities have actively incorporated point of care and medical access into their research programs. 44
Methodologically, in many field-based research investigations in biological anthropology related to human health, work in austere and extreme environments benefits from, and is likely only possible, using a diverse and complementary methodologic toolkit.7,10,36 In such work, researchers pair minimally invasive biomarkers with real-time monitoring via wearables and psychometric and ethnographic evaluations.45–50 Real-time monitoring provides information about specific biomarkers as related to participants over the course of their experience but critically also allows for participants to understand what is happening to their own bodies and adjust as needed. Individualized health data such as heart rate, total energy expenditure, and activity intensity are collected with this technology and can be paired with participant psychosocial responses, allowing for precision medical decisions. Patterns of change via trend lines and other graphics from these data are available to show participants immediately after and sometimes during data collection. Integrating these methods can be simple even in austere environments because commercially available wearable monitors such as Fitbits, Whoop bracelets, Oura rings, and Apple watches have exploded in popularity and are used every day.46,51 In addition, studies can be designed to integrate point of care with research protocols because of their ease of use, ability to be used remotely, and minimally invasive nature of specific biological material collection. 51
The following case studies offer a few contextual examples from biological anthropologists using mixed methodologies, point-of-care technologies, and remote data-collection training to showcase how these tools and perspectives may contribute to making health systems research more adaptable in space.
Case Studies
Case Study 1: Iterative Health Decision Making Under COVID-19 Stress—K. J. Hurd, Oaxaca City, Oaxaca, Mexico
From July to October 2021, at the height of the COVID-19 pandemic in Mexico, I worked with women in Oaxaca City to understand how the pandemic impacted their nutritional well-being, decision making, and metabolic health. The use of mixed methodologies to collect quantitative and qualitative data on health is an established biocultural anthropologic approach that helps assess how humans interpret biological changes as a function of their structural and social surroundings and environment. To assess women's nutritional health in Oaxaca, I used semistructured interviews, 24-h dietary recalls, free lists and pile sorts, surveys, and anthropometric measurements to gather both qualitative and quantitative data. 52 Of particular interest here was the use of minimally invasive finger prick blood draws to instantaneously assess hemoglobin and glucose levels 47 paired with community health and iterative approaches to refine the research process across time. Using a glucometer and HemoCue Hb 201+ System Point-of-Care machine (HemoCue America, Danaher Co, Brea, CA), a finger prick blood sample—a singular drop of blood for each test—can provide participants with instant results. This service is hard to come by but provided free on-the-spot results, limiting the need for multiple paid visits to physicians on the other side of town during working hours. These results were paired with each participant's body composition measurements during biweekly interviews over the course of the study via use of an Omron Body Composition Monitor HBF-514C (OMRON Healthcare Inc, Kyoto, Japan), a device that looks and functions like an at-home scale but has the capability to do a full-body reading via bioelectrical impedance sensing to assess participants’ weight, body fat percentage, body mass index (height measured separately), visceral fat, resting metabolism, skeletal muscle percentage, and body age—all by stepping on the scale and holding a hand grip for less than 1 min.
My training as a biocultural anthropologist valued working with participants, not on them as subjects of study. With this in mind, the iterative refinement of the study included, in this case, the addition of examining glucose levels based on participant feedback due to their growing concern about developing type 2 diabetes. 52 Being able to give each participant their results, talk with them, and show them what their levels meant and why this information was important was critical to the dissemination of the project. This practice allowed for participants to understand how their bodies are affected by their everyday surroundings and social and structural influences on health at a deeper level than simply data on a spreadsheet and improved fidelity and investment in the study. In this manner, applied anthropologic methodologies can be a useful and valuable integration to spaceflight research design as we move to more isolating and remote spaces in need of instantaneous results.
Case Study 2: Agile Biobehavioral Research on Expeditions—M. S. Sarma, American Rocky Mountains
Beginning in 2018, I worked with the National Outdoor Leadership School to collect data from college students participating in semester-long expeditions in the American Rocky Mountains to better understand changes to physiology, behavior, and acclimatization. The stressors experienced in the backcountry conditions included hypoxia, cold exposure, and a novel environment, fixed nutritional availability that primarily needed to be carried in and out, constrained access to resources, and a new social group. 53 This study was operationally challenging, collecting data for multiple small groups, many times simultaneously, in remote and disparate settings. With minimal personnel, a constrained budget (∼$20,000), and participants who were physically hard to reach, successful data collection required participant fidelity and engagement—both of which were contingent on methodologies and mechanisms that were relatively noninvasive and informative, making it worthwhile for students to participate beyond a small-value reward (eg, extra protein bars).
To examine acclimatization to their environment as a role in the evolutionary process, I used a mixed methodologic toolkit to robustly capture the suite of physiologic and behavioral changes. Critically, most of the methods were relatively low tech and allowed for rapid and/or real-time monitoring of physiologic and behavioral changes with outputs that were easy for nonexperts to interpret. These methods included collecting body composition changes (using Tanita BC-558 Ironman Segmental Body Composition Monitor bioelectrical impedance scale; Tanita Corp, Arlington Heights, IL) from saliva samples, fingernail samples, data from wearable actigraphy monitors with linked heart-rate monitors (ActiGraph LLC, Pensacola FL), self-reported surveys with standardized psychological instruments, and open-ended questions (including social network maps), and informal interviews.
During the length of the study, in conversations with the students in these courses, I found them surprisingly enthusiastic about participating and collecting their own data across the entire expedition length regardless of the additional burden because our project gave them the evidence behind the changes they were experiencing and feeling on the expeditions, including body composition changes, 53 as well as how they felt about themselves and their group. The mixed-methods and intermittent monitoring approach I took with this study design maximized data collection while minimizing subject burden. It also meant that I was able to provide information to the students during a remote and resource-limited expedition, through personalized reports. This research encouraged a critical dialectic process – given the repeated collection and required maintained engagement throughout the three-month process, the students, who started as subjects, became participants. We collected data on participants during the expedition, informed them during the process, and then with these data, they were able to make appropriate decisions. These additional data allowed participants to feel like they had some sense of control or agency while working through an austere setting.
Using an evolutionary framework, where behavior and physiologic changes are reflecting a collective adjustment to the environment—and not necessarily a pathologic response—the standard biological anthropology austere-proof mixed-methods data collection 10 reflected their actual experience, where physiologic and behavioral dynamics were connected to each other in time and space. Additionally, the dialectic process builds participant experience and feedback into both the research and prospective medical care rather than a post-hoc analysis allowing for the building of a systems medical approach. 6
Case Study 3: Remote Data-Collection Training for Resource-Limited Local Populations—A. M. Niclou, Apia, Samoa
Between 2020 and 2021, I led a research study assessing brown adipose tissue activity and metabolic health in research participants from Apia, Samoa. Given travel restrictions imposed on the US-based team members during the COVID-19 pandemic, study data collection was completed under remote supervision. I provided specific study protocol training, such as resting metabolic rate measurements and thermography to the Obesity, Lifestyle and Genetic Adaptations Study Group team comprised of local Samoan staff scientists and research associates with extensive expertise in participant recruiting, data collection, and sample processing. Training modalities consisted of prerecorded videos, detailed manuals of procedure, and live-video oversight. To assist the team on the ground in Samoa, I shipped thermal imaging cameras, cooling suits, a portable indirect calorimetry unit, and point-of-care lipid and glucose level measuring devices to Samoa to infer brown adipose tissue activity using a noninvasive protocol that previously had been successful in field settings.54–57 This transition to remote oversight was novel to this group given pandemic restrictions and required new approaches to data collection and troubleshooting equipment malfunction, especially given the use of portable and point-of-care instruments in a nonclinical setting. However, with unique expertise and cultural knowledge, the local Obesity, Lifestyle and Genetic Adaptations Study research staff members were given autonomy and were rapidly able to complete all procedures with minimal oversight, resulting in data collected among 100 participants in 6x mo. 58 The success of this study reflects the benefits of collaboration and trust among research scientists and healthcare professionals despite geographic and time-zone barriers. Critically, the work performed with the team in Samoa demonstrated how well a multisite study could work, with data collected by on-the-ground locals providing additional valuable perspectives on the immediate local conditions, needs, and insights that likely would have been missed in traditional research fieldwork. These successes through remote collaborations between lead research investigators and research staff are similar to the scientific achievements completed on the International Space Station. 59 Other areas, such as medicine and research conducted in remote or austere environments requiring specialized training or health profiling (eg, extreme cold, high altitude, and deep sea), also can benefit from this approach. Future medical work and healthcare infrastructure likely will have to build in remote-work and multisite coordination and likely will benefit from multimodal protocols and trust in an autonomous local population.
Discussion
Existing anthropologic field methodologies for collecting biobehavioral, physiologic, and social data are well situated for translation for space medical and health contexts (Figure 1). From the field-based examples just discussed, we identified the following themes: flexible mixed methods, low-tech (or easy-to-troubleshoot) solutions, dialectic engagement with participants, and iterative research protocols that were informed by both participants and on-the-ground researchers. Together the implementation of these themes in the spaceflight research infrastructure will create a robust research ecosystem that can better integrate health research and medical care. This approach to data collection allows for data that might answer person-specific questions beyond the primary research thrust and provides critical context with participants as active members of the research design and team.
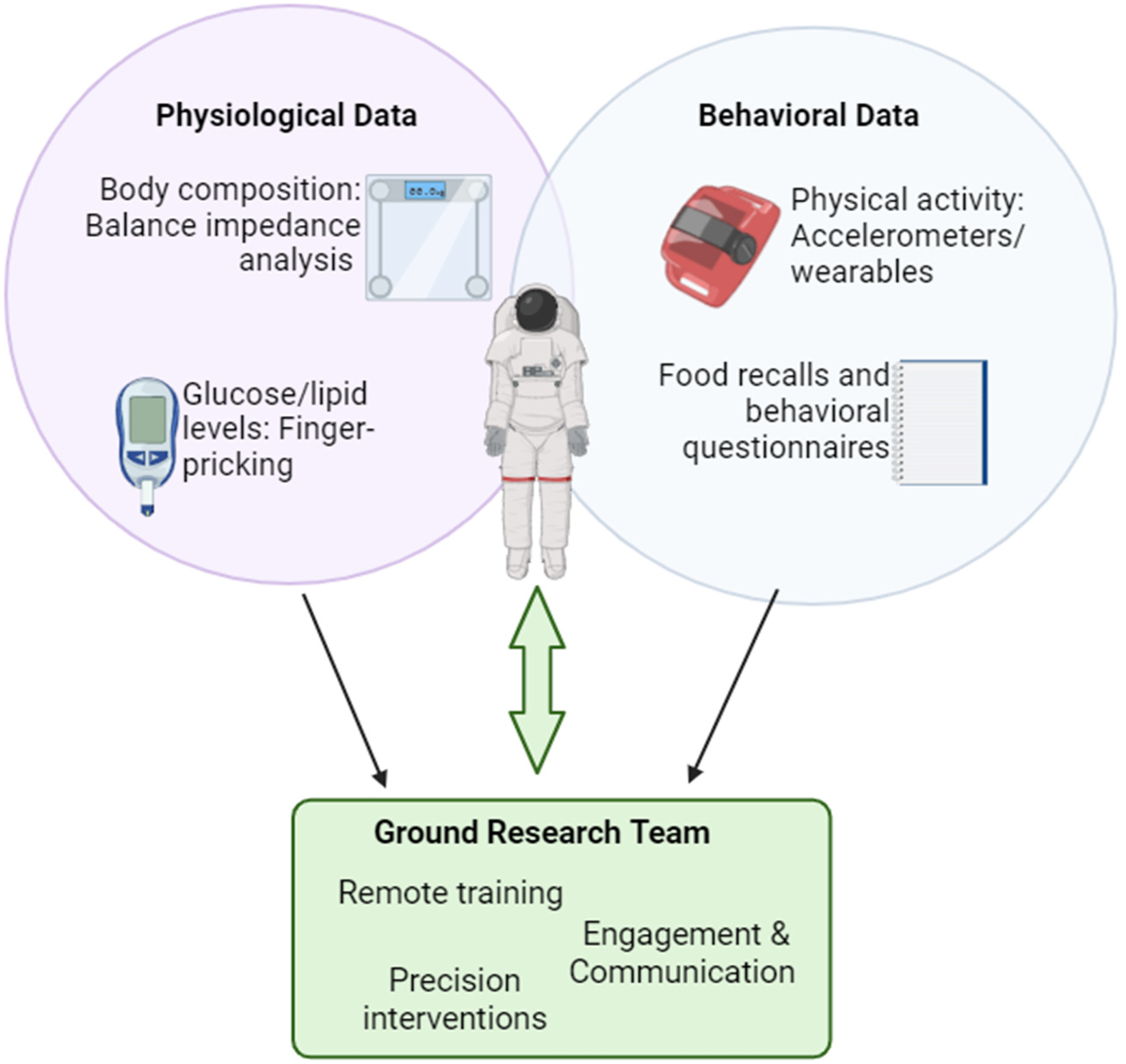
Field-based individualized measures for physiologic and behavioral data collection in austere environments allowing for personalized and time-sensitive interventions.
Biological anthropology builds on fundamentals of human biology, physiology, and evolutionary medicine while simultaneously accounting for behavioral and sociocultural aspects related to the study population, site, or research question that may affect study outcomes. Medicine, particularly space medicine, already includes behaviors such as dietary and physical activity patterns in research and diagnosis.60–62 Yet, the social and physiologic components are often regarded from separate angles instead of combined into interrelated factors affecting health and performance. The mixed-method approach described in the above-mentioned National Outdoor Leadership School study highlights how an interest in composite changes in physiology and behavior during acclimatization to new environments can robustly capture the suite of changes in the dynamic between physiology and behavior. As such, the biological anthropology lens provides a holistic approach that allows the inclusion of behavioral factors in the development of physiologic and medical research questions. Behavioral and environmental components thus not only are considered covariates that need to be adjusted for during statistical analysis but also are fully integrated in the main outcomes alongside biological and physiologic components. Hence, the inherent value of mixed-methodologic data collection and its interpretation is that they provide an integrated and full picture for human health in extreme and austere settings—but can be applied for the more mundane as well—using both qualitative and quantitative data that otherwise may have been lost with only multiple-methodologic data that focus singularly on either quantitative or qualitative data-collection techniques, both not both.
Biological anthropology and space medicine work have demonstrated the variation in health and performance between individuals, environments, and social contexts on their own. Medical practice can benefit from integrating anthropologic perspectives by including broader comparisons across time and space, even in personalized medicine contexts. Although anthropology examines health over a large time frame (ie, an evolutionary time frame), medicine focuses on immediate and individual issues. Yet, the broader understanding of how behavioral and cultural environments have shaped physiologic adaptations over time resulting in current health outcomes provides not only a more in-depth perspective of individual medical profiles but also allows for a more thorough understanding of behavioral and physiologic adaptations to novel environments (ie, space, social isolation, and disease). Collaborations between biological anthropologists and space medicine scientists broaden the perspectives of both fields by introducing new theoretical and practical frameworks to each other's work. 7 Prior to spaceflight, integrating anthropologic methodologies into the modeling of outcomes during missions can contribute to preventative measures gained from long-term perspectives based on evolutionary and sociobehavioral contexts gathered across space, time, and populations. Many anthropologists, in turn, are enthusiastic about implementation-science approaches of medicine, where swift interventions are implemented to individual research participants based on personalized aspects of a shared environment and medical context.10,44,63–65
Integrating these existing biological anthropology field-based methods into space health research can provide rapidly available and multimodal data for research populations. In high-demand environments—such as spaceflight—access to self-data as they change over time can be an important motivation to maintain data collection and fidelity to experimental protocols. It also increases safety because participants have the tools to monitor drastic and potentially life-threatening physiologic changes (eg, heart-rate spikes or low blood sugar levels), increasing the time window for interventions and minimizing risks. Through collaborations with anthropologists and the use of similar anthropologic approaches, space medicine can gain insight into the expected interindividual variation of the long-term effects of current spaceflight endeavors and work toward mitigating the health consequences that may arise from them in the future. This approach would benefit the development of the medical infrastructure currently being built to best accommodate the needs of humans in space by providing evidence of the potential outcomes of long-term spaceflight and social isolation, facilitating the integration of preventative trainings, equipment, and emergency-response procedures.
In austere human health research, there is also a benefit to maximizing low-tech data options to ensure data collection in bare-bones circumstances, such as not having electricity or access to freezers or a cold supply chain. In addition, there is a benefit to looking for solutions that are relatively inexpensive but relay on real-time health monitoring information so that participants can understand their own health data and can potentially make informative decisions based on the data they have available. These approaches allow for robust data collection, creating as full of a picture as possible to be able to address unanticipated phenomena. This kind of well-rounded data collection is crucial in austere settings where populations may be vulnerable and phenomena can be fleeting with minimal to no opportunities for repeated data collection, but particularly in a spaceflight setting.1,66 Further, this anthropologic approach also allows for iterative investigation, where research is done with participants rather than on participants. For example, in one of the case studies, the implementation of new point-of-care measures (ie, glucose monitoring) introduced community concerns for pathologies beyond the narrow scope of the research. This additional methodologic inclusion allowed for further investigation into those other pathologies. 52 In addition, as seen in these case studies, working with participants includes providing individualized and personalized information while simultaneously building a group dataset. This individualized attention helps build the foundation for precision medicine and precision health. This development of a personalized knowledge base is crucial in an austere environment, including in spaceflight, 1 because it supports nuanced decision making when there is limited access to resources and expert care. Further, in austere settings, providing care and information to both individuals and populations takes on additional value because such resources would be inaccessible otherwise. 67 In many terrestrial settings where this work is actively undertaken, it is an ethical duty to contextualize the data that are collected and provide related health data.44,67 In many situations, individual access to personal data may have helped participants make better-informed medical decisions. This access and understanding of their own health data introduce a sense of control in unpredictable conditions. Embracing these methodologies facilitates agency for self-care and encourages further investigation.
Wide ranging mixed-methodologic data collection that encompasses dialectic engagement and iterative research protocols is an operational challenge; it requires interdisciplinary expertise and careful coordination across many entities. However, interdisciplinary collaboration of this nature has been wildly successful in recent spaceflight research68,69 and implies that the effort for this kind of data collection is worthwhile. Using these established field practices embraces this ethos. In addition, translating these field methodologic approaches to spaceflight can leverage the many emerging spaceflight analogues. There is an opportunity to test these practices, develop and standardize technologies among physiologic and behavioral evaluation needs, and integrate medical care into research design.
In a spaceflight environment, we suggest using perspectives from biological anthropology to facilitate the integration between medical care and research that allows both to occur in tandem under (relatively full) transparency. Austere settings are a transformative space where behavioral decision making shifts based on health and medical data availability. Implementing these field method perspectives introduces an important paradigm shift in how we approach data and the overarching research design that shall likely shape our spaceflight futures.
Footnotes
Author Contribution(s)
M. S. Sarma, A. M. Niclou, and K. J. Hurd contributed to the conceptualization, and writing (original draft, review & editing) of the manuscript. They each contributed to the specific data curation, formal analysis, funding acquisition, and investigation of the data presented in individual case studies, respectively. A. M. Niclou created the figure and M. S. Sarma oversaw project administration, and supervision of the manuscript.
Disclaimer
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the United States Army, the Department of Defense, or the National Institutes of Health. Any citations of commercial organizations and trade names in this report do not constitute an official Department of the Army endorsement or approval of the products or services of these organizations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AMN was funded by an appointment to the US Army Research Institute of Environmental Medicine administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the US Department of Energy and the US Army Medical Research and Development Command. AMN also was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under Award No. T32DK064584. MSS was supported by the National Institute on Deafness and Other Communication Disorders of the National Institutes of Health under Award No. 5T32DC000023-33.