
Abstract
Introduction
Avalanches and tree-wells (TW) are causes of snow immersion death in skiers and snowboarders. TW burials may have different victim physiology profiles and rescue considerations than avalanche-related burials due to snow density, burial position, and compensatory physiologic responses. This study aimed to compare the physiological responses between avalanche and TW burials through a prospective controlled trial of simulated avalanche burial to simulated TW burial.
Methods
Eleven volunteers participated in two paired 60-min snow burials: Avalanche and TW simulations, controlling for position and snowpack densities. We monitored core temperature, respiratory rate, minute ventilation, end-tidal carbon dioxide, oxygen saturation, partial pressure of inspired carbon dioxide, and heart rate.
Results
The average cooling rate for the avalanche simulation was −0.017(Δ°C/min) versus −0.012(Δ°C/min) for the TW simulation (p = 0.014*), 1.42 times faster cooling rate than TW burial. SpO2 decreased 10.9 times faster on average in TW burial than in avalanche conditions when normalized by burial time as a rate (avalanche −0.011 vs TW −0.12 (Δ%/min), p = 0.033*). More participants requested early study termination in the TW scenario.
Discussion
Simulated TW burial resulted in a statistically significant slower rate of core temperature cooling and earlier hypoxemia. Inverted body position in TW burials may lead to increased physiologic distress and contribute to earlier hypoxia. These findings may have important implications for search and rescue as well as resuscitation efforts for snow burial victims.
Introduction
An increasing number of skiers and snowboarders are caught in tree-well (TW) snow immersions. 1 Non-avalanche-related snow-immersion deaths occur when a skier or snowboarder falls, often headfirst, into a deep TW or a powder bank. These incidents may be known by other terms, such as non-avalanche snow burial (NASB). Incidents are more common near conifer trees with low-hanging branches, which block snow from filling the area around the trunk. The low-density snow surrounding the tree trunks creates a steep drop-off just beneath the edge of the tree branch coverage. This phenomenon is more prevalent on the western coast of North America. 2 Large volumes of snowstorm deposits, deep snowpacks, and higher moisture content typical in maritime snowpacks further contribute to a deeper and more dangerous TW. When a victim falls headfirst into a TW, they may also dislodge snow on tree branches, further covering their bodies. A struggle to dislodge oneself funnels more snow downward toward the face and further compacts the snow around the body. The headfirst fall into low-density snow, followed by additional snow accumulation from above, creates a challenging situation for the victim and rescuers.
Avalanche snow burials have higher-density snow than TW burials due to violent snow movement and compaction during the avalanche. Reported avalanche debris densities range from 30% for a mid-winter dry snow avalanche to 60% or higher for a springtime wet snow avalanche. 3 Mountain snow coverage in a transitional or continental snowpack that has not avalanched is 10% to 20% snow density by comparison. Previous studies contrasted the higher density of avalanche debris versus gradually accumulated lower-density TW snow. 4 The higher density of avalanche debris snow decreases oxygen extraction from the snow and impedes CO2 diffusion away from the buried avalanche victim.5–7
The positions of avalanche victims vary considerably. The true frequency of final position (eg, inverted vs upright) is difficult to determine. Victims who self-extricate or are quickly rescued in shallow burials are typically not documented in the literature. Fatal avalanche burials in deep snow are more often in the prone versus supine position. 8
While previous studies have evaluated human physiology and hypothermia during snow burial, none have assessed the differences in physiological responses between a person buried in an avalanche compared to TW. Furthermore, most studies are retrospective and thus only extrapolate physiological changes that may have occurred. The objective of this study was to compare the cardiopulmonary and thermoregulatory physiology of avalanche-simulated snow burial to TW-simulated snow burial. We hypothesized that TW-simulated burial would result in more acute respiratory distress and hypoxemia due to inverted position, even though the victim is submerged in a less dense snowpack. This knowledge will educate recreationists on the best survival strategies and guide rescue and resuscitation protocols for non-avalanche snow-immersion victims.
Methods
Fourteen healthy volunteers, 18 to 60 years old, were recruited to undergo two snow burial trials: simulated avalanche burial and TW burial in a crossover study design. Participant demographics are described in Table 1. Exclusion criteria included self-reported smoking, pregnancy, claustrophobia, or diagnosis of cardiac or pulmonary disease. The study was conducted at a ski resort in Utah at 2469 m elevation (average barometric pressure 570 mm Hg, snow temperature of 27.8°F, and air temperature 33.0°F). Participants were randomized into avalanche or TW scenarios for the first burial and alternate burial scenario (avalanche or TW) on their second burial. The first and second burial scenarios were temporally spaced by a minimum of 3 days to avoid any learning bias and to ensure they returned to their physiologic baseline. Burial was terminated upon participant request (anxiety, distress, difficulty with respiratory tubing, or any reason determined by the participant) or predetermined endpoints: core temperature < 35°C or SpO2 < 85%. The study was approved by the University of Utah Institutional Review Board (IRB_00061186).
Baseline Demographics of Participants.
The snow density was determined at multiple sites using a 250 cm3 wedge density cutter (Snowmetrics, Ft Collins, CO) that measured the water weight per cubic meter. The snow density was reported as a percentage (300 kg/m3 is a 30% density of snow or 70% air). The snow density goal in the avalanche scenario was 40%–50% to replicate a moderate-density snowpack similar to avalanche debris. The snow density goal in the TW scenario was 10%–20% to replicate a light-density snowpack similar to a TW. To standardize the participants and their insulation, each volunteer was fitted with a one-piece Gore-Tex suit, lightweight skullcap, insulated helmet, goggles, face mask, and gloves. The participants wore their own long underwear, socks, and snow boots.
Baseline parameters before the simulated burial were measured with the participants breathing ambient air on the surface. Physiological variables were continuously monitored before, during, and after the simulated burial scenario of TW or avalanche. Parameters included: respiratory rate (RR), tidal volume (VT), minute ventilation (VE), end-tidal carbon dioxide (ETCO2), partial pressure of inspired carbon dioxide (PICO2), oxygen saturation (SpO2), core temperature (Tc), heart rate (HR), and burial time. Participants used a mouthpiece attached to respiratory tubing connected to an Avalung device (Black Diamond Equipment LTD, Salt Lake City, UT) that diverts expired air away from inspired air. This is accomplished using a one-way inspiratory valve on the anterior chest that allows inhalation of air from the snowpack and a second one-way expiratory valve on the chest that diverts expired air to the back. This allowed the subject to breathe air from the snowpack adjacent to the anterior chest area and exhale air posteriorly, thereby reducing the accumulation of CO2 in inspired air during the study.6,7 The device was outfitted with oxygen tubing to provide 100% O2 that could be initiated in the event of hypoxia. The device was also fitted with a CO2 SMO-Plus (Novametrix Medical Systems, Inc., Wallingford, CT, USA) attached in-line with an airway adapter to monitor RR, VT, ETCO2, and PICO2, as well as a pulse oximeter on the index finger that measured SpO2. Tc was measured by an esophageal capsule swallowed just before the burial (VitalSense, Philips Respironics; Bend, OR). The participant was fitted with leads for the 3-lead cardiac rhythm, RR monitor by thoracic impedance, surface temperature probe, and a second index finger pulse oximeter connected to a portable monitor (NPB-4000; Mallinckrodt). As a backup, a third pulse oximeter was used on the middle finger in case there were any problems with oximetry readings (Nonin Onyx, Nonin Medical Products, Minneapolis, MN, USA). A 2-way radio intercom was strapped to their chest to allow for continuous communication during the trial. Burial time was recorded as the time the participant tolerated immersion. The burial duration was limited to 60 min. The burial could be stopped before 60 min at participant request via radio, distress indicated by kicking their feet noted by study administrators, or if a predetermined study endpoint had been met (core temperature <35 °C or SpO2 < 85%). Subjective experience was then evaluated using a brief questionnaire with prompts relating to their subjective experiences.
Avalanche Simulation
To create the simulated avalanche burial scenarios, 1 × 3 meters of untouched snow was selected. New snow was shoveled on top of this area and compacted by researchers (80 kg) walking over the area repeatedly. Once compacted, a 1 × 3-meter pit was dug 1.3 meters deep, with a 60° backrest created for support. The participants were placed upright inside the pit with bodies bent at the waist, legs straight, and back and head reclining against the backrest. Once in position with safety and monitoring equipment check completed, compacted snow was piled around the participant as they breathed using the Avalung device to cover them at least 0.5 meters until fully buried (excluding their legs). Participants’ legs were left unburied distal to their knees as a safety measure for the participant to kick if panicking, such that administrators could pull them out. Although avalanche victims may be found in any position, the decision was made to standardize avalanche victims to the above position to minimize the variables changed and better contrast with the typical position of TW burials. Figure 1a depicts the burial positions described for the avalanche simulation.
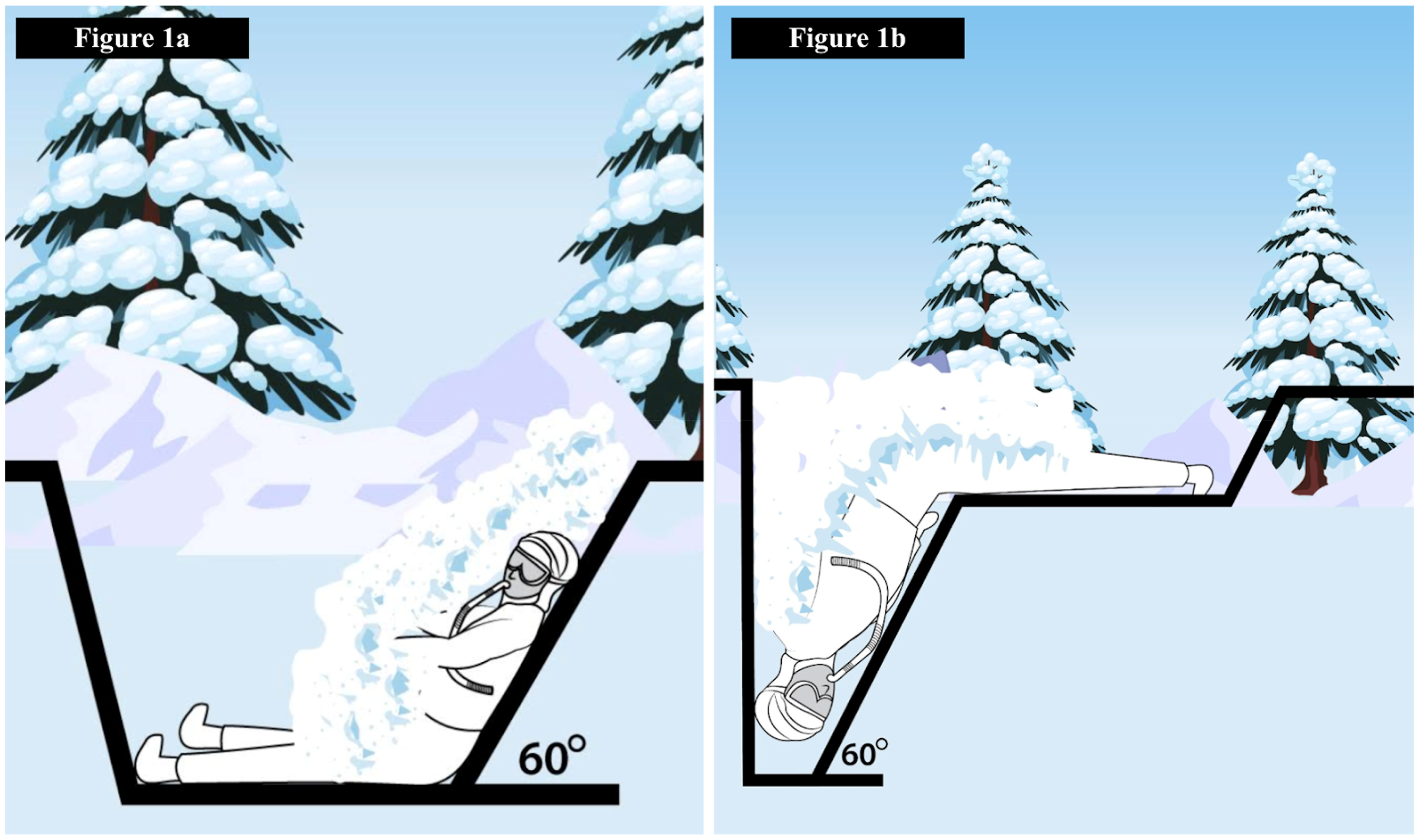
Snow burial positions for (a) avalanche and (b) tree-well scenarios.
Tree-Well Simulation
In the TW scenario, the 1 × 3-meter pad of untouched snow was not compacted. The front of the pit was dug 1.3 meters deep at a 60° angle, creating a hole large enough for the participant's head, arms, and torso to enter. A trough was created to extend the legs. Participants were placed face down with their bodies bent at the waist. Their torso, arms, and head extended downward into the pit with their legs straight in a trough. Once in position with safety and monitoring equipment check completed and while breathing using the Avalung device, non-compacted light snow was piled around the participant to cover them at least 0.5 meters until fully buried (excluding their legs). Figure 1b depicts the burial positions described for the TW simulation.
Statistical analysis with two-tailed t-tests (p < 0.05, 95% confidence interval [CI]) and multilevel/hierarchical regression analyses were conducted using the MCMCglmm package in R version 3.3.0 (2016, R Foundation for Statistical Computing, Vienna, Austria, http://www.R-project.org/). Variables were identified by the start and end times along with the delta. To compare the simulations, the burial time variation was normalized using a linear rate model of change based on the delta value and burial duration.
Results
Of the original 14 participants, 2 did not return for the second burial and 1 participant had equipment failure, resulting in incomplete data; all 3 were excluded from the study analysis, resulting in data from 11 total participants used for analysis. Table 2 depicts the recorded variables by their derived means and statistically identified p-values.
Data Means for Each Measured and Calculated Metric Used for Comparison in the Avalanche and Tree-Well Simulations, as Well as a p-Value for Comparative Measure Between the Two Simulations.
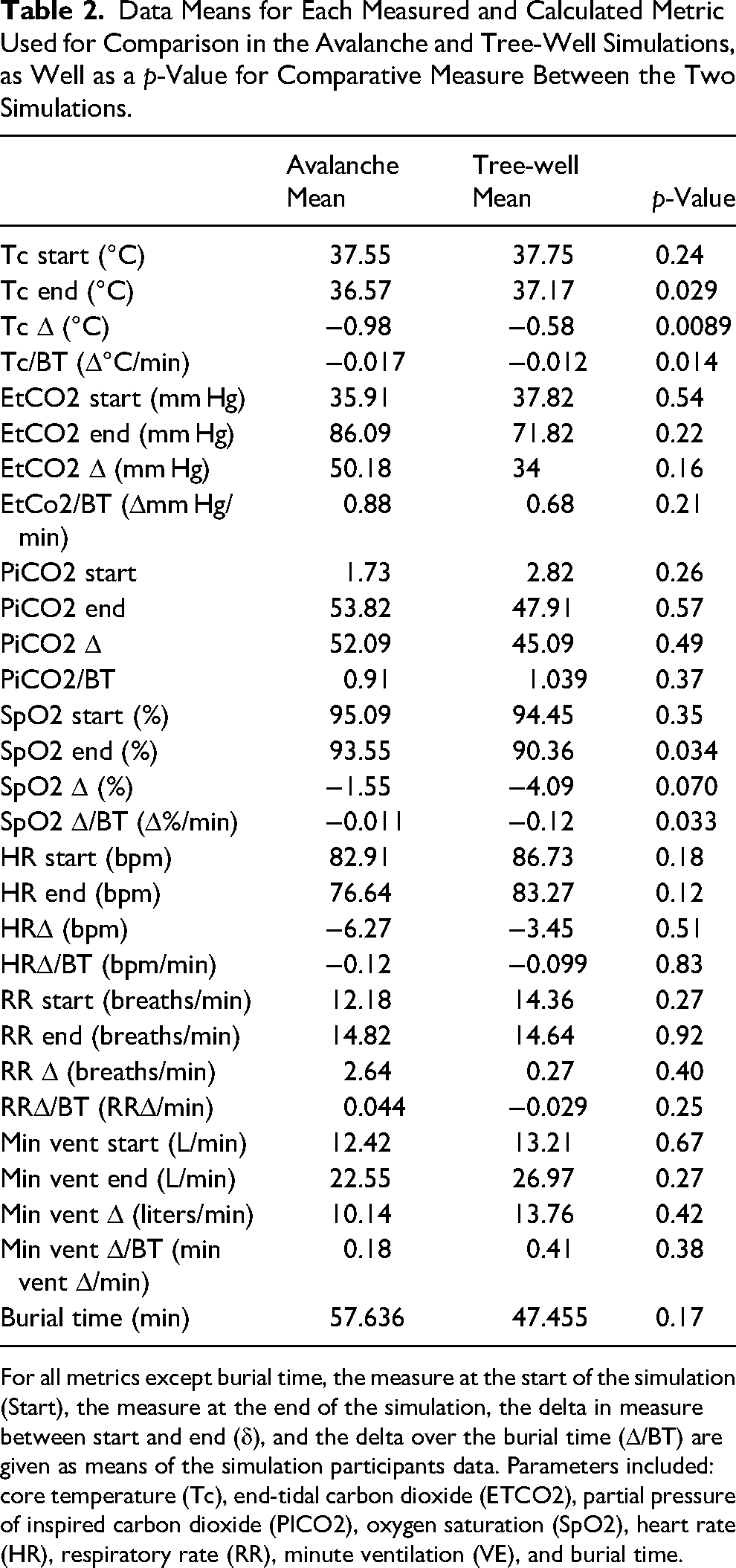
For all metrics except burial time, the measure at the start of the simulation (Start), the measure at the end of the simulation, the delta in measure between start and end (δ), and the delta over the burial time (Δ/BT) are given as means of the simulation participants data. Parameters included: core temperature (Tc), end-tidal carbon dioxide (ETCO2), partial pressure of inspired carbon dioxide (PICO2), oxygen saturation (SpO2), heart rate (HR), respiratory rate (RR), minute ventilation (VE), and burial time.
Early Extrication
In the avalanche burial, 8 of 11 participants completed the 60-min burial; the other 3 required early termination of the study: 1 by participant request (48 min), 1 for core temperature <35 °C at 51 min), and 1 for SpO2 < 85% at 55 min). In the TW burial, 7 of 11 participants completed the full 60 min, with 4 requiring early termination of the study. Three participants terminated early at 11, 14, and 19 min (average time to termination was 14.6 min). All participants cited early termination due to anxiety and distress, with 1 also indicating difficulty with respiratory tubing. Administrators terminated the burial in 1 participant for SpO2 < 85% at 58 min. Burial times for each subject are compared between conditions in Figure 2.
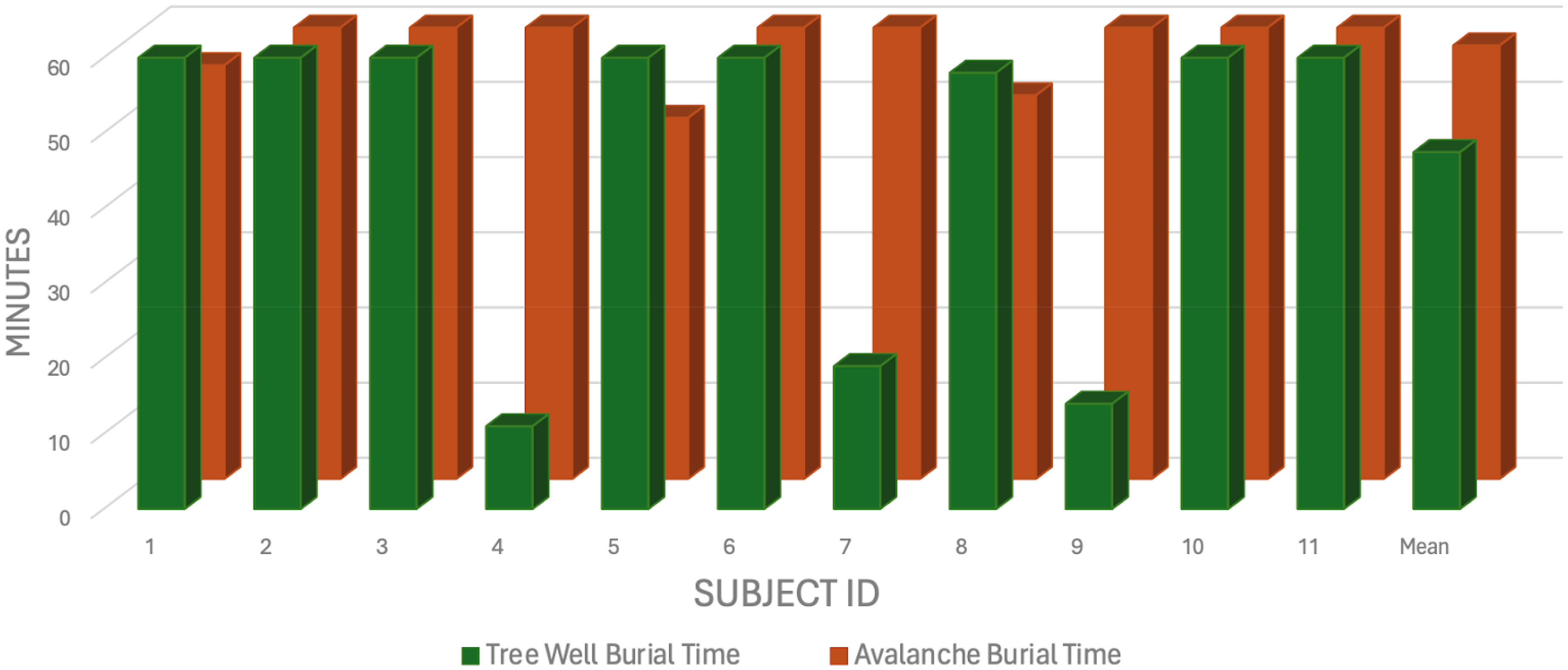
Length of burial times of participants in the TW simulation superimposed on the burial time of their avalanche simulation. A summary of all variables collected at the start and end of both burial scenarios, as well as the corresponding p-values comparing them, is found in Table 2. Upon limiting the false discovery rate to 5%, secondary analyses revealed no statistically significant difference between burial types for RR, VE, ETCO2, PICO2, or HR.
Core Temperature
In the avalanche simulation, the mean Tc Δ (°C) was −0.98 compared to −0.58 in the TW (p = 0.0089*). The average cooling rate calculated by temperature change over burial time (BT) Tc/BT (Δ°C/min) for the avalanche simulation was −0.017 versus −0.012 for the TW simulation (p = 0.014*). Though the different burial positions mean Tc Δ only differed by 0.4 °C more in the avalanche burials, the extrapolated cooling rate indicates that the average cooling rate of the avalanche simulation was 1.42 times faster than the TW simulation. Figure 3 shows the subject-level time series of core temperature for each condition. No statistical difference was found between study conditions for RR, VE, ETCO2, PICO2, or HR.
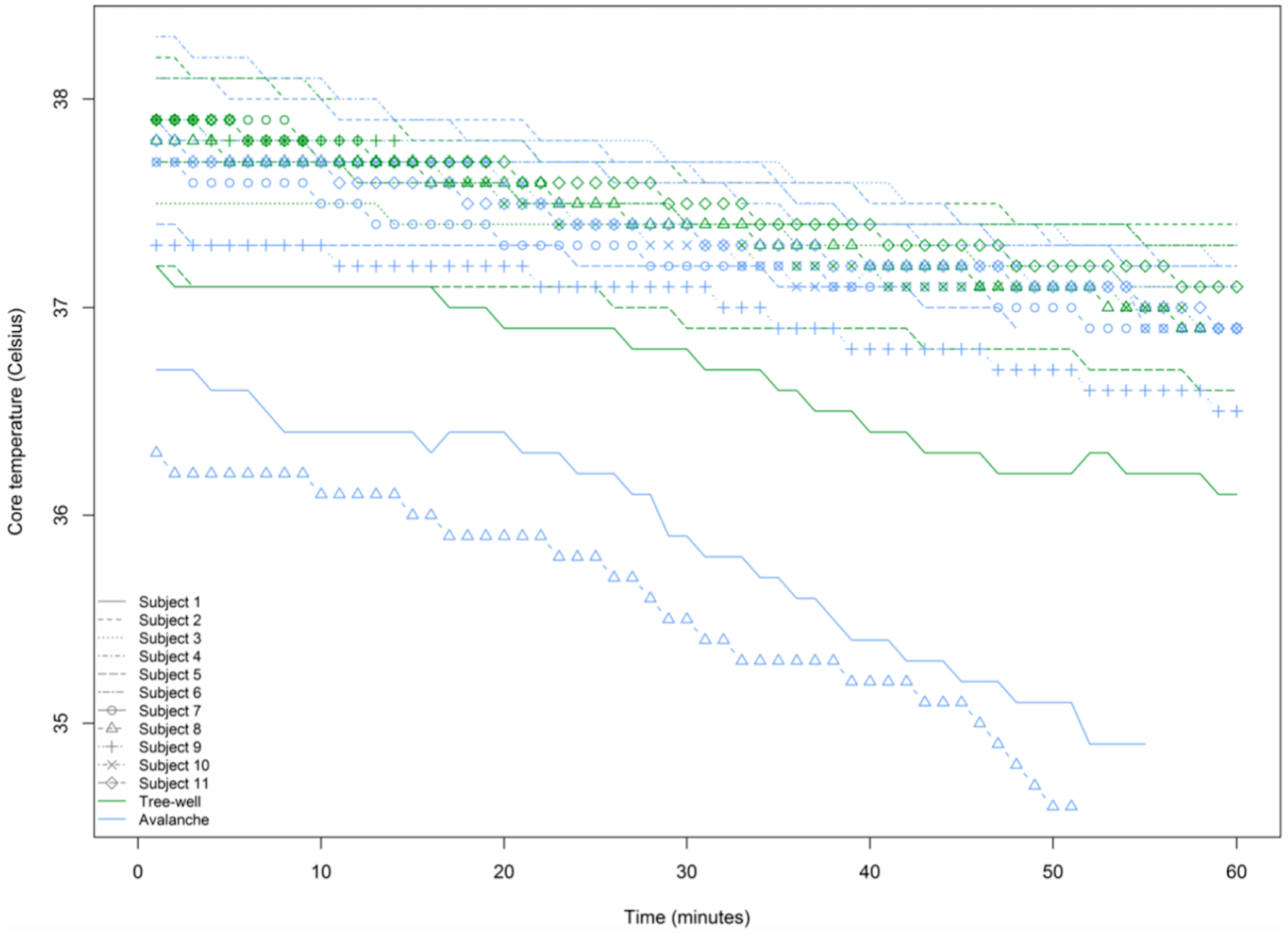
Each participant's minute-to-minute core temperature over time in the TW and avalanche burial simulations.
Oxygen Saturation
SpO2 was found to decrease at a faster rate in the TW simulation. The mean SpO2 Δ (%) approached significance (avalanche −1.55 vs TW −4.09, p = 0.070). Whereas when normalized by burial time, the SpO2 Δ/BT (Δ%/min) showed statistical significance (avalanche −0.011 vs TW −0.12, p = 0.033*). This demonstrated that SpO2 decreased 10.9 times faster on average in TW burial than in avalanche participants. When comparing participant start and end SpO2, a relationship is evident, indicating a more rapid decrease in the TW simulation, which is depicted in Figure 4.
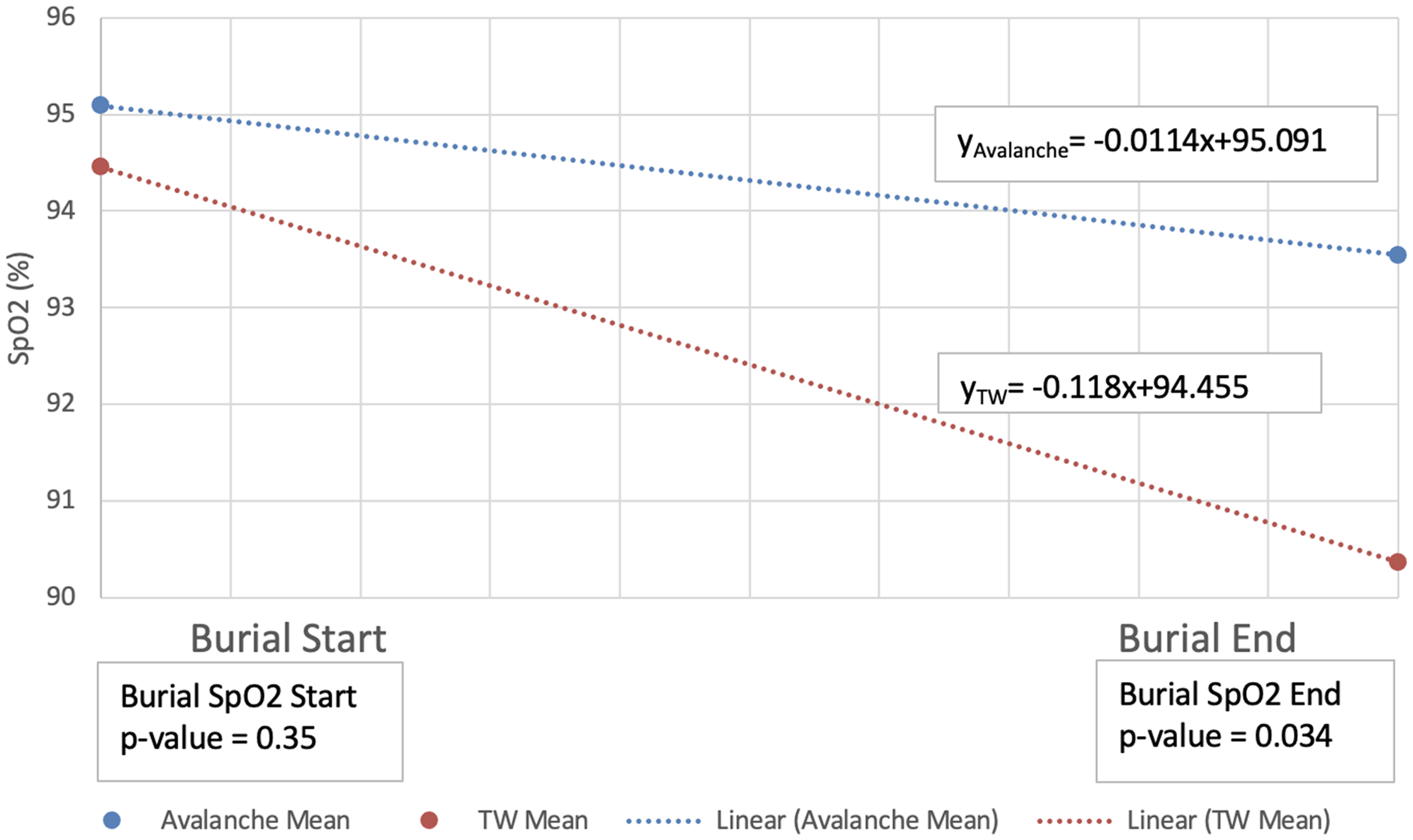
Mean SpO2 recorded for both the TW and avalanche conditions at the start and end of the burial condition simulations. Simulations were ended early if the participant reached the predetermined endpoint of SpO2 < 85% or met the criteria for early simulation termination. The slope for the avalanche simulation was −0.0114(°C/minute of burial) and −0.118(°C/minute of burial) for the TW burial.
Subjective Reports
73% of the participants rated the TW simulation as being more challenging to tolerate. The most challenging parts of the avalanche burials were “air hunger” and “breathing through a tube,” whereas in the TW simulation, they also indicated “burial position” and “feelings of anxiety.” Subjects in the TW simulation further commented that reasons for early termination included: “shortness of breath leading to panic,” “giving up because it was hard to breath,” and “anxiety leading to hyperventilation leading to dizziness.”
Discussion
We found that TW burial simulations resulted in a statistically significant slower rate of cooling, a quicker occurrence of hypoxia, and earlier study termination compared to avalanche simulations.
The faster cooling in the avalanche simulation likely occurred because the snowpack density was higher in the avalanche than in the TW simulations, and thermal loss was therefore greater. This faster cooling rate in avalanche situations may have implications when considering anticipated treatment for hypothermia in burial victims. However, the statistical difference may only have clinical significance in recoveries after long burial times. For example, if starting at 37°C, it would take 412 min in an avalanche scenario to drop core temperature below 30°C, where one would expect clinically significant sequelae from hypothermia, such as ventricular fibrillation or ventricular tachycardia. However, in a TW scenario the same 7°C drop in core temperature would be expected to take 583 min—171 min longer than the avalanche scenario.
The second finding was that SpO2 decreased faster in TW simulations than in avalanche simulations. Higher snow density results in less diffusion of CO2 away from the participant and increased PICO2 and decreased PAO2 in the alveolus according to the alveolar gas equation. This phenomenon of the denser snowpack culminates in progressive hypoxemia. If this were the primary variable leading to hypoxia, then we would expect to see SpO2 decreasing faster in the avalanche simulation rather than the TW. Given this relationship of snow density to breathable air diffusion, we believe that burial position may be more influential on the development of hypoxemia. The inverted TW position increases pressure on the diaphragm, which limits the ability to inspire an adequate tidal volume, further contributing to hypoxia. The head-down position in TW burials may lead to increased psychological distress, causing more rapid and shallow breathing and resulting in a quicker rate of hypoxia.
The faster decline in SpO2, indicating more rapid hypoxemia in the TW burial, is supported by the subjective survey questionnaire responses in which participants reported more “panic” and “oxygen hunger” among the TW burial; 73% of the participants rated the TW burial as being more challenging to tolerate.
The third finding was that more participants requested early study termination in the TW scenario. Moreover, those who terminated the avalanche simulation early outlasted those who terminated the TW burial by an average of 38 min. This suggests that the inverted position creates a substantially more intolerable subjective experience earlier in the experiment. We believe the intolerance of TW burials can be attributed to the inverted position, resulting in anxiety due to abdominal contents pressing down on the diaphragm, leading to respiratory distress. Further studies on the correlation between inverted position, distress, and hypoxia could benefit both emergency medical services and winter outdoor enthusiasts.
When skiing in TW terrain, skiers and riders should maintain a strict buddy system, ideally keeping within line of sight of partners and using radios to communicate position and status. In the event of a fall, verbal calls such as “skier down” can alert nearby partners to initiate a rescue. Additionally, using GPS location tracking and sharing one's position with the group may improve response times in case of a TW burial. To reduce entrapment risk, skiers should observe increased caution when riding in tree lines, especially after a recent substantial snowfall, tucking and rolling to land on their skis or grabbing a tree branch to prevent full submersion. If caught in a tree-well, staying calm and creating an air pocket while minimizing struggle may help delay asphyxiation until rescue arrives. Implementing these proactive safety measures may mitigate the risks associated with tree-well burials and improve survival outcomes.
Limitations
Our findings are limited by the small sample size and use of simulated burial scenarios. Avalanche and TW burials were standardized with a single body position and simulated snow conditions; a myriad of other positions are possible to simulate actual burials. Real-life variables such as snowpack proximity to the face, aspiration, presence of an air pocket, and position following avalanche turbulence all can affect respiration during burial. Our study also did not consider the physiological effects of self-extrication during snow burial, as a real burial victim may attempt to self-extricate. An actual snow burial would likely elicit an immediate and strong anxiety response due to the unexpected avalanche or TW burial situation. Our planned and standardized burials could not account for these real-life circumstances.
Conclusions
Our avalanche and TW burial simulations revealed 3 salient findings when comparing TW to avalanche scenarios: TW scenarios resulted in a statistically significant slower rate of cooling, a quicker occurrence of hypoxia when normalized by burial time, and an earlier request for study termination.
Footnotes
Acknowledgments
We would like to acknowledge and thank Grissom et al for loaning our study group the majority of the equipment, including monitors and safety gear, as well as the University of Utah Department of Emergency Medicine for allowing our study group access to safety gear and oxygen tanks.
Author Contribution(s)
Data Access Statement
Research data supporting this publication are available from the corresponding author.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Utah Emergency Department research fund. The majority of the equipment, including monitors and safety gear, were graciously loaned to our study group from Intermountain Medical Center.