
Abstract
Frostbite is frequently seen in high altitude climbers. Many Sherpas, members of an ethnic community living high in the Himalayas in Nepal, help the climbers as a guide or an assistant. They often seem to undertake few precautionary measures thus suffer more from frostbite. A young Sherpa, who had reached the top of Mt Kanchenjunga in March 2009, suffered from deep frostbite in his fingers. Fortunately, he recovered well with generous treatment. Though there is no evidence whether Sherpas are more or less prone to frostbite, simple techniques for adequate prevention of hypoxia, hypothermia and dehydration will benefit any climber to the high altitudes.
Introduction
Frostbite is the most common cold injury in mountaineering and is frequently seen in high altitude climbers. 1 Many believe that Sherpas, members of an ethnic group from the most mountainous region of Nepal, high in the Himalayas, do not suffer from high altitude illness and frostbite. Many Sherpa staff on treks and expeditions do not take the necessary precautions required to prevent frostbite and therefore suffer from this problem. We discuss some of the causes, prevention, and treatment of frostbite, especially in the Himalayan setting.
Case Report
A 23-year-old male Sherpa climber-guide was involved in the Kanchenjunga Expedition that started in late March 2009. He did not use supplemental oxygen. At the summit (8585 m) he felt extremely cold. When he took off his gloves to take pictures, he felt even colder and had severe pain in all of his fingers. He was shivering and had numbness and tingling in his extremities. He also felt fatigued with loss of appetite and he drank very little fluid. By the time he descended to base camp (5100 m), he had swelling of the fingers and toes with darkening of the skin of some of his fingers. Gradually, the swelling in the fingers turned into blisters, some of which ruptured spontaneously. He had never previously had such problems during his career of 6 years in mountain trekking and climbing to altitudes above 8000 m. When he reached base camp, his hands and feet had already thawed spontaneously. Povidone-iodine dressing was applied and tetanus toxoid injection was given. Blistered areas were not debrided. He was given analgesics and sent to Kathmandu.
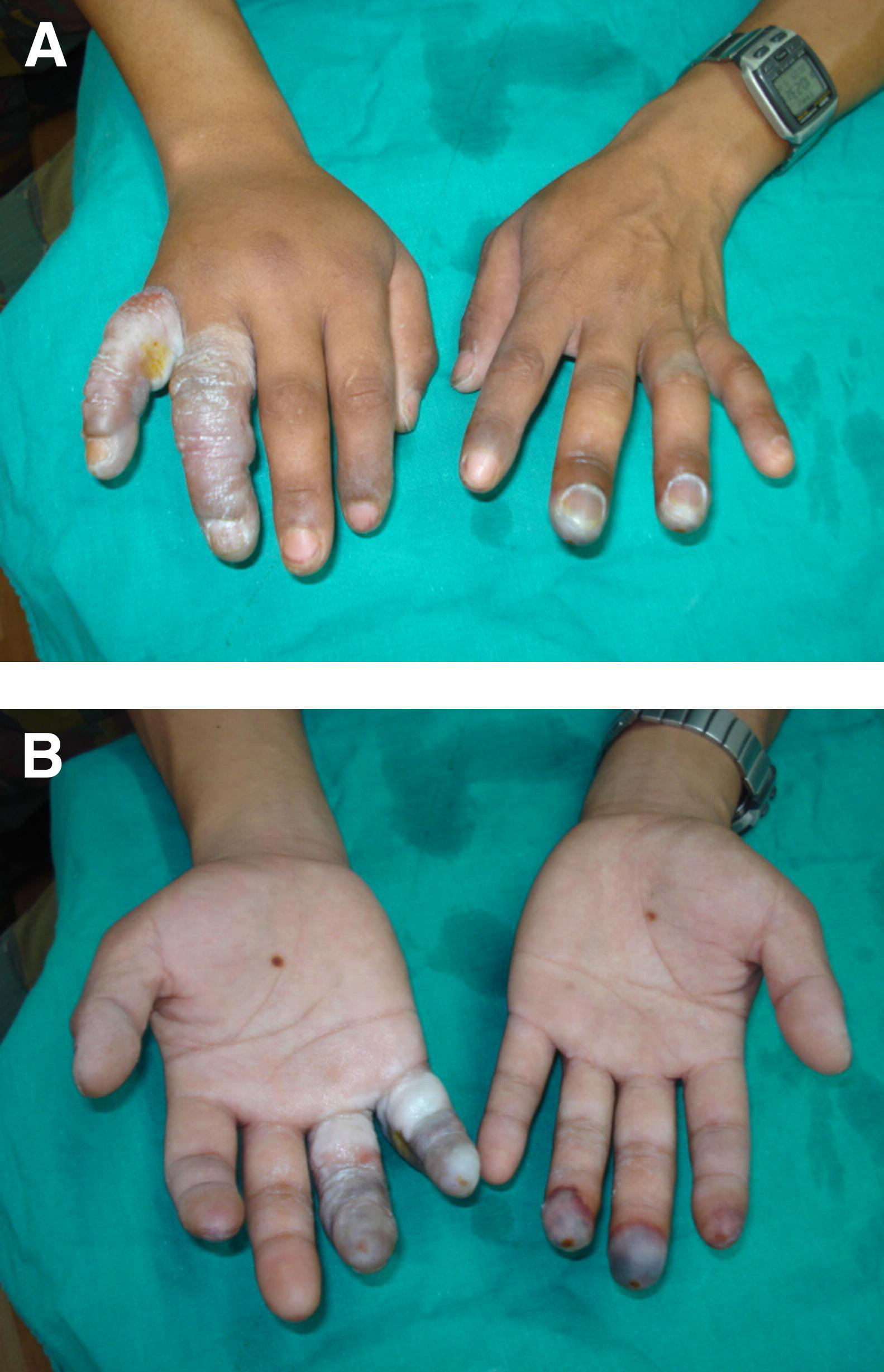
When he arrived at Nepal International Clinic (Travel and Mountain Medicine Center) in Kathmandu, the patient was well oriented with normal vital signs. There was blackish discoloration at the tip of the nose and on both cheeks. His hands and feet were covered in a dirty cloth and some discharge was observed during removal of the bandage from his feet. Examination of the extremities showed swelling and ruptured hemorrhagic blisters of the proximal ring and little fingers of the right hand, as well as blackening of the skin distally (Figure). There was normal joint mobility in the fingers and intact sensation except at the tips. The dorsum of the right hand was swollen and mildly tender. On the left hand the distal third of the middle and ring fingers were swollen with clear blistering and blackening of the palmar aspect. Sensation was absent at the tip of the left middle finger. Swelling and clear blisters were also present in both big toes with black discoloration and loss of sensation at the distal ends.
Blood tests (complete blood cell count, creatinine, blood sugar) and radiographs of the affected hands and feet did not show any abnormalities. We treated him by soaking his hands and feet in warm water and povidone-iodine solution for 30 minutes. Aloe vera was applied to the frostbitten areas. A bulky dressing was then placed over the area. The patient was prescribed cloxacillin 500 mg every 6 hours for 7 days and advised to apply antibiotic ointment twice per day. After 4 weeks of regular warm soaking in povidone-iodine and use of aloe vera dressings, the patient had almost full recovery without any loss of tissue. His only sequela was persistent numbness in the ring and little fingers of the right hand.
Discussion
Frostbite occurs when unprotected tissue is exposed to temperatures well below freezing even for relatively short periods. 2 The tissues in the affected areas freeze. Ice crystals form intracellularly (if freezing is very rapid) or in the intracellular space. This results in water being drawn out of the cell, causing cell damage. 3 Concurrently, there is slowing of blood flow in the affected area, eventually leading to thrombosis and to tissue ischemia. 4 In addition to the acute injury, frostbite is associated with late sequelae that can include altered vasomotor function, neuropathies, joint articular cartilage changes, and, in children, growth defects caused by damage to the epiphyseal plate. 2 -5
Factors that contribute to frostbite include hypothermia, inadequate clothing, wet clothes, wind chill, and dehydration from increased metabolic activity associated with climbing.1,2 In addition, fluid loss, inadequate intake of water, hypoxia due to high altitude, and poor circulation from any cause, such as tight boots, increase the risk of frostbite. Certain medications, smoking, alcohol use, or any systemic or local disease affecting blood vessels may also predispose to frostbite. 2 -4
Initial treatment of frostbite is rapid rewarming of the frozen tissue by submersion in warm water at 37°C to 39°C (just above body temperature) until return of circulation, usually about 15 to 30 minutes. High temperature thawing may be deleterious. Thawing and subsequent refreezing can cause devastating tissue injuries.5,6 Tissue that has already thawed does not benefit from “rewarming.” Rubbing or massaging the frostbitten tissues to rewarm them can be very harmful since excessive movement can cause the ice crystals formed in the tissue to do further damage. 6 Aloe vera dressing, wrapping, and elevation of the frostbitten extremities are often recommended. Aloe vera may aid healing of frostbite. 7 -9 Tetanus prophylaxis and analgesics are routinely recommended.3,6 Antibiotics are not routinely prescribed for all cases of frostbite. However, we decided to use antibiotics, since we suspected localized infection. Use of thrombolytic therapy, either locally or systematically, shows promise. It may improve tissue perfusion and reduce amputations 5 ,6,10; however, this treatment strategy is difficult to implement in medical systems with limited resources in places like Nepal. There are claims that hyperbaric oxygen may improve blood flow in frostbitten areas more than 2 weeks after the injury. 2 ,3,11,12 Debridement of necrotic tissues is generally delayed until there is a clear demarcation from viable tissues, a process that may take up to 3 months. Surgical intervention is reserved mainly for late treatment of frostbite or when guided by advanced imaging such as triple-phase bone scanning or magnetic resonance imaging. 3 ,5,6
Anecdotally, we have noticed that frostbite cases are more common among Sherpa staff than among foreign mountaineers. A major reason for this could be the lack of awareness among Sherpas of the need to keep their extremities well protected and to keep well hydrated throughout the trek. During high altitude treks, it is not unusual for Sherpas to carry insufficient water for hydration, because they believe it is not important. Living in the mountainous regions of Nepal may impart a false feeling of security among the Sherpa staff, leading to use of fewer precautionary measures. In this case, the patient took inadequate amounts of fluid. This may have resulted in dehydration, predisposing him to frostbite. Taking off his gloves to take pictures at the summit when he was already feeling very cold shows a degree of carelessness on the part of the patient that increased his chances of acquiring frostbite in his fingers. The fact that he had frostnip of the tip of his nose and his cheeks, shivering and pain, and numbness of his extremities gives us an indication of the degree of cold exposure 2 -4 our patient experienced at the summit. The hypoxia present at high altitude and the fact that he was not using supplemental oxygen may have contributed to his frostbite. Sherpas often use medical treatment such as simple cleaning, bandaging, and use of traditional herbal medicines. Medical problems other than frostbite in the Sherpa trekking staff have been documented in the literature. 13
Even brief exposure to cold, as in our case where the Sherpa took off his gloves at the summit, can cause frostbite. Those who recognize these problems and take preventive measures like drinking adequate fluids, wearing warm protective clothing, and using supplemental oxygen for mountain climbing are less likely to suffer from frostbite. 2 ,3,14 There is no evidence in the literature that Sherpas are more susceptible to frostbite than foreigners. Simple steps to prevent hypothermia, hypoxia, and dehydration can benefit any climber at high altitude. Fortunately, our patient did not suffer any major sequelae of frostbite. If Sherpa staff and the trekking agencies that employ them were more cautious and undertook these measures during expeditions, perhaps we would see fewer cases of frostbite.