
Abstract
Introduction
Ski patrollers face unique occupational risks and may be exposed to traumatic events. This study aimed to determine the relationship between traumatic event exposures and wellbeing among a cohort of U.S. ski patrollers.
Methods
A non-experimental, descriptive, longitudinal design was followed to complete a pilot study. An online survey was employed with repeated measures (1, 2, & 3 months). Participants were conveniently sampled from one ski resort in the Western United States. This study was informed by the stress continuum model.
Results
A total of 29 participants completed at least one follow-up survey and were included as the analytic sample. Participants were primarily White (n = 27, 93.10%), non-Hispanic or Latino (n = 27, 93.10%), and male (n = 19, 65.52%), aged 39.07 on average. Three-quarters of participants reported exposure to traumatic events at Survey 1 (n = 22, 75.86%), and the frequency ranged from 1 to 20 events. Increased frequency of traumatic events by each one event was significantly related to decreased wellbeing levels over 3 months (β = −0.0253, p < .0001, 95% CI: [−0.0364, −0.0141]), after controlling for age, sex, race, ethnicity, marital status, and working hours. When included as an interaction term, resilience was found to buffer the negative effect of traumatic event exposure on wellbeing (β = −0.0068, p < .0001, 95% CI: [−0.0099, −0.0038]).
Conclusions
Findings underscore the need for additional research to identify the most effective ways to support the wellbeing and resilience of ski patrollers.
Keywords
Introduction
Ski patrollers comprise a unique occupational group that is highly skilled, works in extreme weather conditions, responds to traumatic injuries and critical scenarios, and manages avalanche risk to ensure the safety of patrons at ski resorts and in the backcountry. In their roles, they are exposed to certain occupational risks that include both physical injuries and traumatic stress injuries that may arise when caring for others. In particular, evidence has suggested that snow sport resort workers, such as ski instructors, ski patrol, and ski guides, have a high occupational injury rate of 8 incidents per 100 individuals per year of employment. 1 For comparison, the total recordable cases for nonfatal work injury and illness rates across U.S. private industries in 2023 were 2.4 per 100 cases. 2 In one study, nearly half of ski patrollers reported previous serious injury to themselves or someone close to them (n = 36, 49%). 3 There are further physical risks posed by avalanche mitigation. For example, 80% (n = 151) of patrollers previously reported having an avalanche-related accident or near miss. 4 Evidence over a 45-year time period found that out of 440 avalanche deaths, 3.6% were ski patrollers themselves. 5
The majority of U.S. ski patrollers complete fundamental training in the outdoor emergency care (OEC) curriculum from the National Ski Patrol in order to respond to the numerous injuries among skiers and snowboarders.6,7 Some patrollers have additional training as emergency medical technicians (EMTs).8,9 In their roles, they often respond to head injuries and concussions, knee injuries, and fractures. 10 While ski patrollers’ decisions are instrumental for positive outcomes, 7 some rescues unfortunately become recoveries. 11 Across approximately 480 operating ski resorts in the United States, 12 a total of 46 fatalities were reported over the 2022/2023 season, 13 exposing patrollers to potentially traumatic events.
Traumatic events involve experiencing or witnessing serious injury or death, caring for life-threatening injuries, or managing poor outcomes. 14 Such events are major stressors that impact health, often disrupting sleep, 15 which lowers wellbeing. 16 Persistent stress may cause respiratory and cardiac disease and has been associated with exacerbations of autoimmune diseases and excessive inflammation. 17 Chronic stress can also impair decision-making, increasing the risk of avalanche-related accidents. 18 In the professional ski community, psychological stress from a traumatic event may impair coping and is considered a stress injury. 19
Theoretical Framework
Stress injuries can be defined as psychological, emotional, or physical strain 20 stemming from stressful or traumatic events. Stress injuries are common among snow professionals 21 and may influence emotional wellbeing and prosperity. 22 Informed by principles from the stress continuum model, the ability to cope with stress injuries is categorized on a continuum from green to red. This continuum visually represents how one is responding to stress and the impact stress may have on their functioning and wellbeing. If an individual is operating at the red level, their stress may be interfering with their ability to complete their job.23,24 Stress injuries can further lead to post-traumatic stress disorder (PTSD), sleep disturbance, substance use, anxiety, isolation, hopelessness, depression, and thoughts of suicide. 19 Depression and suicide have been noted previously among those living and working in mountain towns and may be due to factors such as isolation, income disparities, substance use, and lower oxygen levels at altitude. 25 Altitude and suicide rates have been positively correlated in the literature, highlighting an increased risk for suicide for those in mountain areas like ski patrollers.26,27 Ski patrollers also work as first responders, who have been found to be at higher risk for suicide when compared to the general public. 28
In order to treat stress injuries before they become critical 21 and to promote overall worker wellbeing, it is important to first understand the worker's overall health status and traumatic risk exposures. Current available evidence has revealed limited scientific literature on the health of ski patrollers generally, highlighting a gap surrounding how their work may impact their wellbeing. Thus, the purpose of this pilot study was to determine how occupational traumatic event exposures may affect overall wellbeing among a cohort of U.S. ski patrollers.
Methods
This study followed a non-experimental, longitudinal design using an online survey with repeated measures. Participants were purposively sampled from ski patrollers working at one ski resort in the Western United States with high snowfall and steep terrain. Inclusion criteria involved: those 18 years of age or older, currently employed at the participating ski resort, and currently working as a ski patroller. Those not actively working the season as a ski patroller were excluded from participation. Around mid-point in the ski season in February 2024, a research team member presented an overview of the study to the ski patrollers on site at two of their after-work debrief sessions. Following this presentation, the researcher shared the recruitment flyer via email, which directed prospective participants to the REDCap online survey, and participation began.
This study was approved by the University of California, Los Angeles Institutional Review Board #24-000098. The researchers followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist relating to the title, abstract, introduction, methods, results, and discussion sections to ensure a complete and accurate reporting of this study. 29
Measures
The survey included 55 self-administered questions and is comprised of valid and reliable measures. Traumatic event exposure was measured with two questions: 1) yes/no for exposure and 2) number of events. This variable was informed by the definition of traumatic events 14 and the Experienced Traumatic Events Frequency Score. 30 Research team members established face validity by discussing the phrasing and making suggestions for updates to ensure these questions appropriately reflected the traumatic event variable. 31 Perceived work stress was measured with the 8 items from the Workplace Stress Scale, where scores from each answer are added up for a total score ranging from 8 to 40. 32 Wellbeing was measured with the 18 items of the Employee Wellbeing Scale, 33 where a mean score is calculated ranging from 1 to 6. Physical symptoms were determined by adding up the 15 items from the PHQ15, where symptoms range from 0 to 30. 34 Anxiety and depression comprised the mental health variables and were measured with the 4 items from the PHQ4. 35 Mental health scores were added up to range from 0 to 12. 35 Resilience was measured with the 6 items from the Brief Resilience Scale. A mean score is calculated to range from 1 to 5. 36 Sociodemographic questions were also collected for biological sex, ethnicity, race, relationship status, tenure, hours worked per week, and age. The sociodemographic questions were adapted from the Behavioral Risk Factor Surveillance System Survey 37 and the Survey on Patient Safety Culture Database, 38 tested by investigators for face validity to ensure constructs were measured appropriately. 31
Data Analysis
Study data were collected and managed using REDCap electronic data capture tools hosted at the University of California, Los Angeles. REDCap is a secure, web-based software platform designed to support data capture for research studies. 39 Once data collection was completed, the data was exported, cleaned, coded, and checked for any outliers or missing data. Participants who did not complete at least one follow-up survey were considered to have missing data and were removed from the analysis.
Data was explored for patterns, trends, and distributions using SAS software. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, NC. Descriptive statistics were run to analyze characteristics of sociodemographic data collected at Survey 1 and the outcome variables over 3 months. Regression modeling was then used to explore relationships between traumatic event exposure (binary: yes/no) and traumatic event frequency (continuous) with personal health outcome variables over the three time points. Specifically, generalized estimating equation (GEE) linear regression, with a normal distribution assumption for the continuous nature of outcome variables and an autoregressive correlation structure, was used as an appropriate choice to manage the repeated measures and longitudinal data from the small sample size (N ≤ 50). 40 Quasi-likelihood under the Independence Model Criterion (QIC) was used to select the best-working correlation structure, where a lower QIC value indicates a better fit. 41
Results
The first survey was completed by 38 participants out of the 79 patrollers at the participating ski resort. A total of 29 participants completed at least one follow-up survey, indicating a 76.3% follow-up response rate. Those who completed at least one follow-up survey comprised the sample for analysis in this study. Participants were primarily White (n = 27, 93.10%), Non-Hispanic or Latino (n = 27, 93.10%), and male (n = 19, 65.52%). On average, ski patrollers were 39.07 years old. The majority reported working more than 40 h per week (n = 24, 82.76%), and many worked at this resort for 11 or more years (n = 11, 40.74%). See Table 1 for more sociodemographic characteristics of the sample.
Sociodemographic Characteristics Among a Sample of U.S. Ski Patrollers at Survey 1.
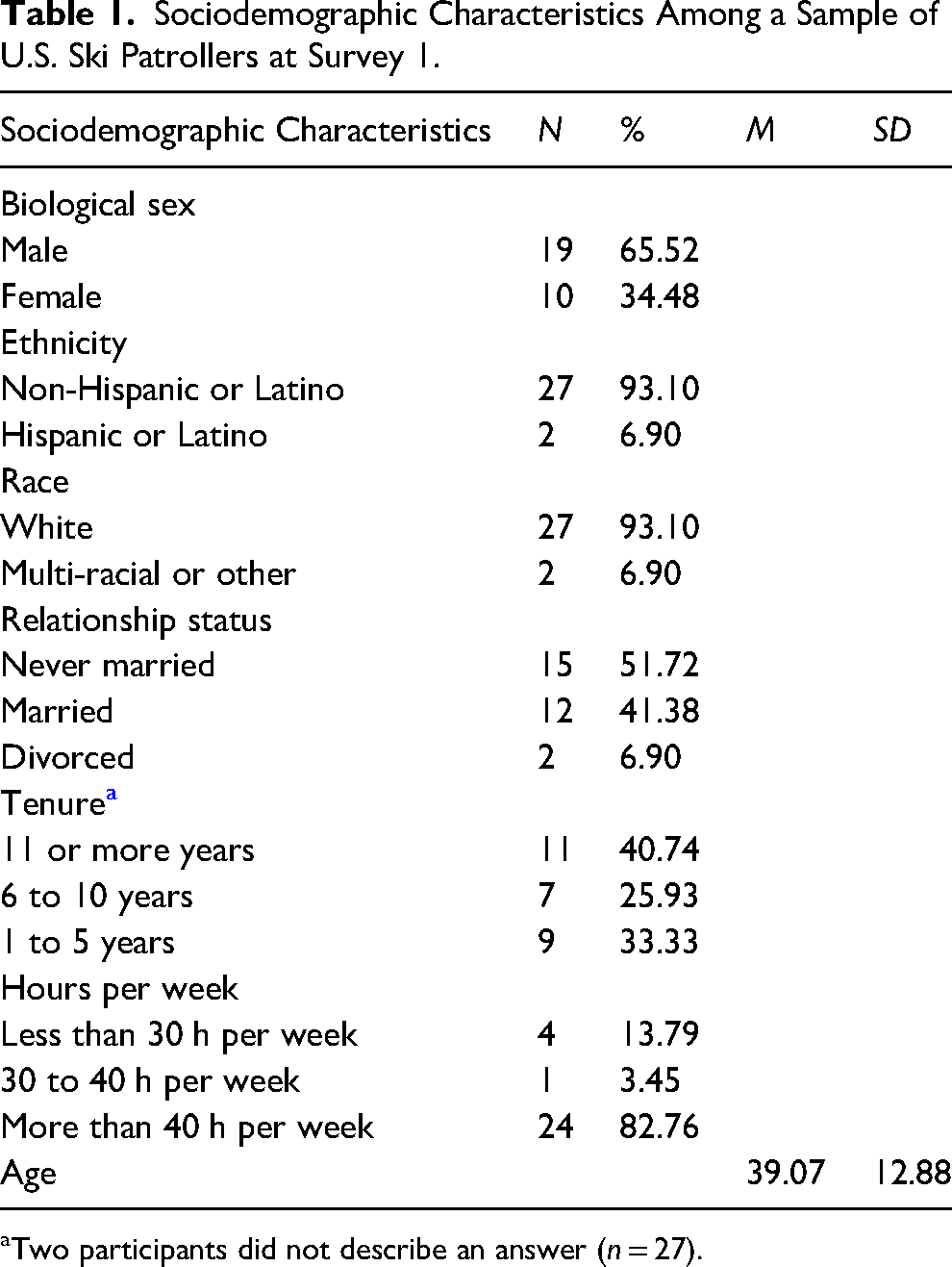
Two participants did not describe an answer (n = 27).
At Survey 1, approximately three-quarters of participants reported “yes” to exposure to traumatic events over the 2023–2024 season (n = 22, 75.86%). The baseline survey also revealed that the frequency of traumatic events ranged from 1 to 20 occurrences over the season, with most participants exposed 1–3 times (see Table 2). We calculated the sum of the number of traumatic events for each participant over the study and used Pearson correlation coefficients to see if there were any significant correlations between age with traumatic event total and baseline exposure. Age had a marginally significant correlation with traumatic events at baseline only (p = .05). We then used ANOVA to see if there were any significant differences in each subgroup of demographic characteristics with traumatic event total and baseline exposure. Findings revealed no significant differences in baseline or total number of traumatic events based on sex, ethnicity, race, relationship status, hours worked per week, and tenure.
Traumatic Event Exposure Among a Sample of U.S. Ski Patrollers.

Note. All participants completed Survey 1 around mid-point in their season.
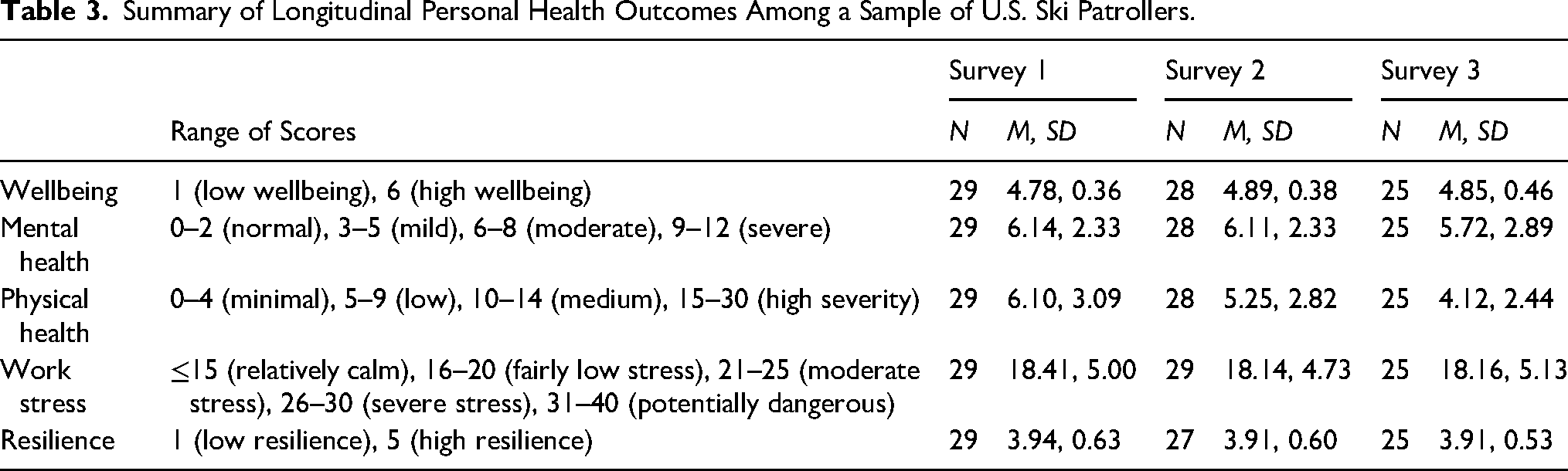
Physical symptoms and mental health scores were at low to moderate severity levels for Survey 1. Resiliency, wellbeing, and work stressors were considered within normal limits over the course of the study. Please refer to Table 3 to discover personal health outcomes across the three time points of the study.
Summary of Longitudinal Personal Health Outcomes Among a Sample of U.S. Ski Patrollers.
Generalized Estimating Equation
Increased frequency of traumatic events by each one event was significantly related to decreased wellbeing levels over 3 months (β = −0.0253, p < .0001, 95% CI: [−0.0364, −0.0141]), after controlling for age, sex, race, ethnicity, marital status, and working hours. Exposure and frequency of traumatic events were not found to be significantly associated with mental health, physical health, work stress, and resilience levels among this sample based on our GEE model, as noted in Table 4. Tenure was not controlled for in this model due to missing data and the risk for multicollinearity. 42
Relationship of Health Outcomes and Traumatic Events Among Ski Patrollers.
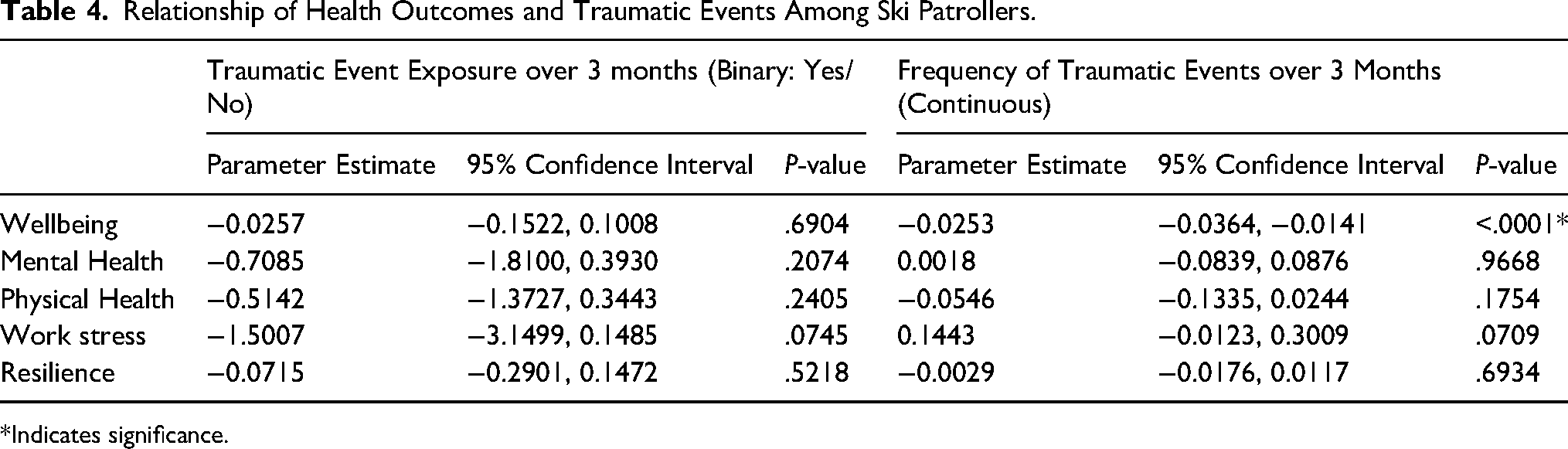
*Indicates significance.
After categorizing the number of traumatic event exposures into ranges of 0, 1–2, and 3 or more, and running an additional GEE, we found that exposure to at least 3 traumatic events was associated with a clinically significant drop in wellbeing, suggesting minimal clinically important difference, which is defined by the change score exceeding a half SD of the respective baseline score. 43 Please refer to Table 5 to view the relationship found between health outcomes and categorical traumatic event exposure. After controlling for resilience both as a covariate and as an interaction term with traumatic event exposure, the results suggest that as resilience increases, the negative effect of traumatic event exposure on wellbeing decreases (β = −0.0068, p < .0001, 95% CI: [−0.0099, −0.0038]). This indicates that resilience may serve as a buffer against the impact of traumatic event exposure on wellbeing (see Table 6).
Relationship of Health Outcomes with Categorical Traumatic Event Exposure Among Ski Patrollers.
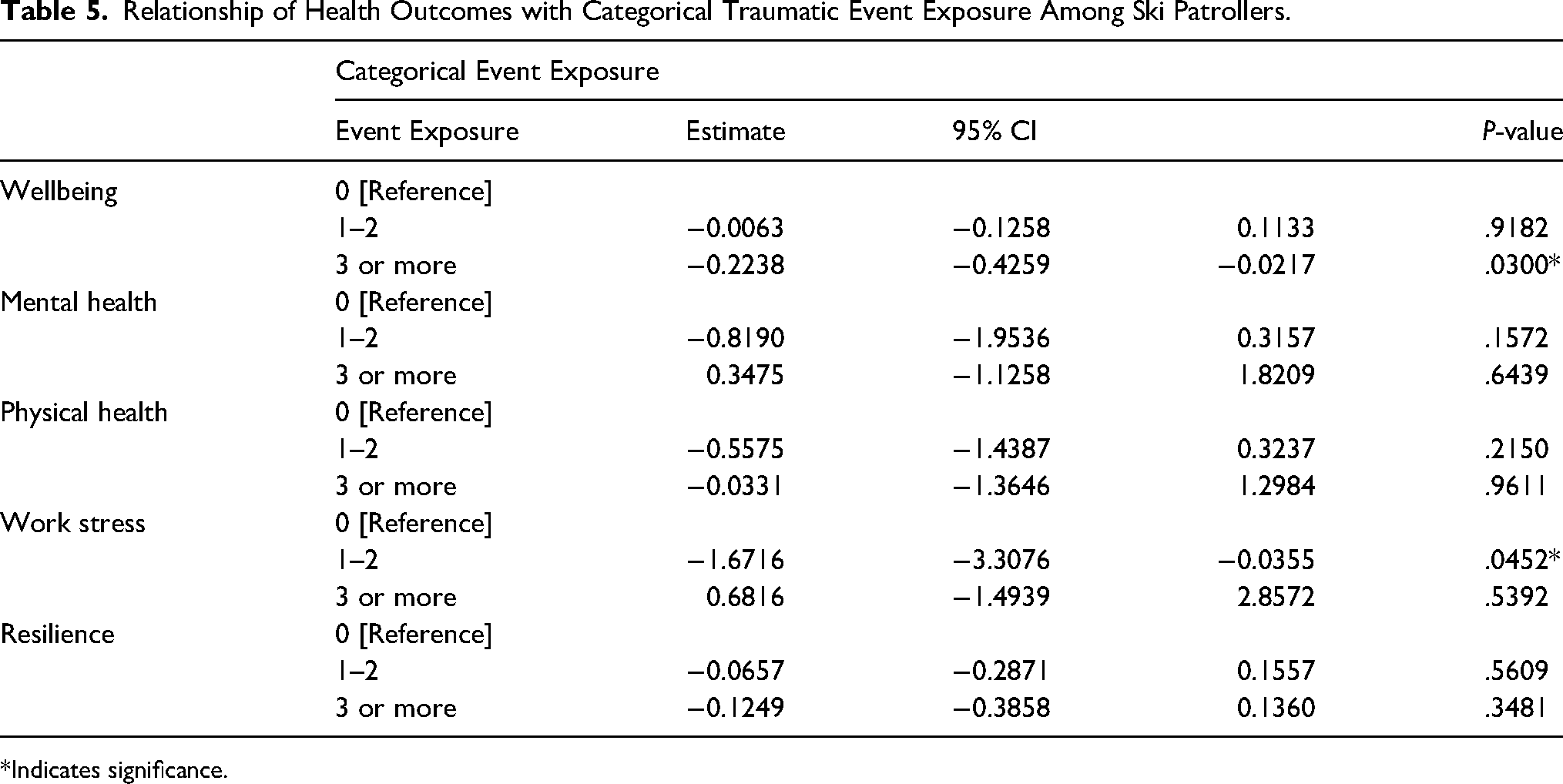
*Indicates significance.
Relationship of Health Outcomes with Traumatic Events Among Ski Patrollers, Accounting for Resilience and Its Interaction with Traumatic Event Exposure.
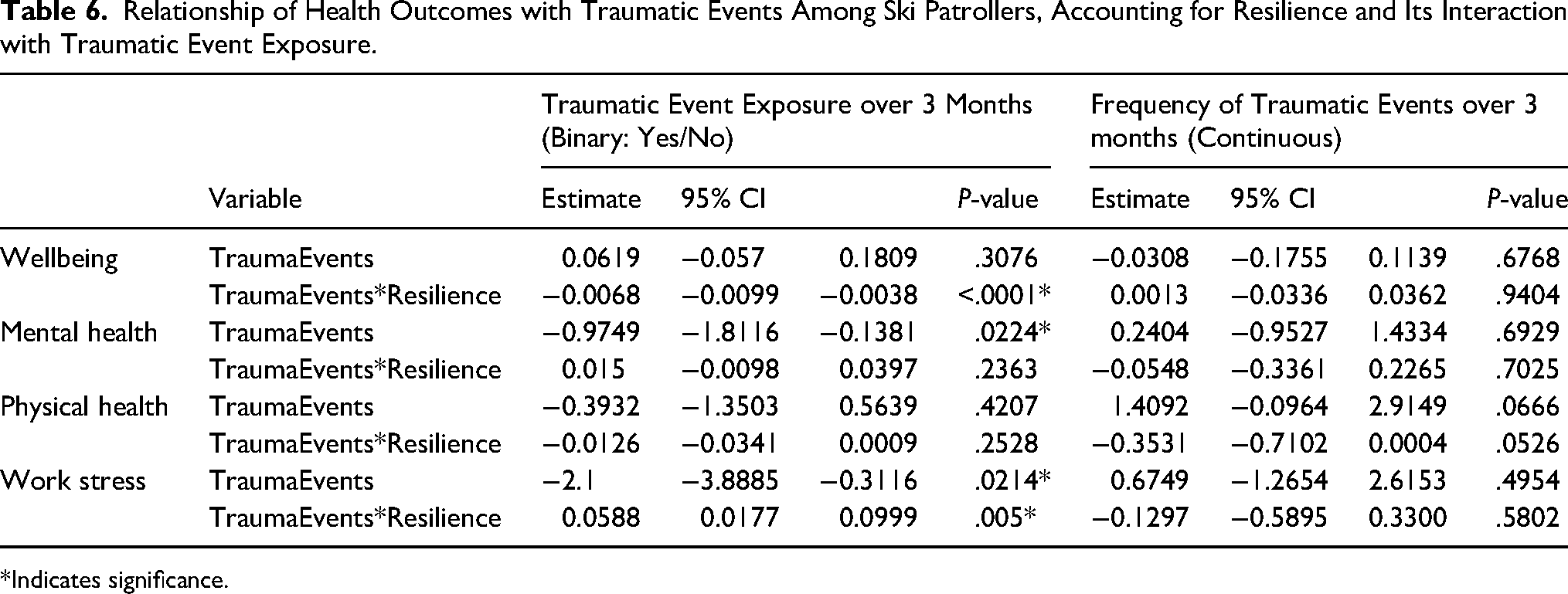
*Indicates significance.
Discussion
Results from this work show that ski patrollers are exposed to traumatic events in their roles, and a statistically significant relationship exists between their wellbeing and the frequency of traumatic event exposures over 3 months. The exposure to traumatic events among ski patrollers is similar to the frequent exposure found among rescue workers in the literature. 44 Additional evidence supports how high trauma exposure among emergency personnel places them at higher risk for adverse mental health outcomes.45,46 Although mental health contributes to overall wellbeing, the lack of a significant relationship with traumatic events in the GEE model may be due to the core aspects measured by each scale. Specifically, the wellbeing scale used in this study comprises three constructs: 1) personal wellbeing, which includes personal emotions and family life issues; 2) workplace wellbeing, covering work arrangements, compensation, and benefits; and 3) psychosocial wellbeing, which focuses on learning, growth, and self-actualization. 33 In contrast, the factors of mental health that were measured mainly pertain to depression and anxiety. 35
Although mental health was not significantly related to traumatic events, findings revealed worse mental health outcomes among participants across the study duration. Evidence from search and rescue volunteers suggests a continued stigma surrounding mental health and the potential for under-reporting concerns due to risks of breach of confidentiality or fear of how that may impact their careers.47,48 Thus, the self-reported moderate levels of mental health reported in this pilot study may actually be an underestimate. Additionally, some workers may not know of the available resources or have scheduling conflicts when seeking help, 47 highlighting the need for organizations to ensure mental health supports are accessible and well-advertised. Workplace-based interventions of knowledge development, leadership development, communication and team building, stress management, and workload and time management were found to improve healthcare workers’ mental health in one review. 49 The review also underscored the importance of employee engagement, so future research is warranted on exploring what types of mental health support may be most helpful among the population of ski patrollers.
Physical symptom levels among the sample in this pilot study were higher at baseline (Survey 1) when compared to Survey 3 but were considered low throughout. This may be due to the timing of when the last survey was completed, where the season had ended. In addition to the timing potentially impacting results, findings were also generally positive for levels of resilience, wellbeing, and work stress. This may be because skiing as a leisure activity has been shown to reduce anxiety 50 and improve health.51,52
Resilience levels may have been higher, and work stress lower, due to ongoing efforts to promote resilience and stress injury education in the ski industry.53,54 Since our results suggest that resilience can serve as a protective factor mitigating negative impacts on wellbeing, maintaining and supporting such programs could be beneficial. For example, the 3-3-3 protocol, developed by the Responder Alliance as part of the Incident Support Framework, assists in checking in with patrollers at 3 key intervals: 3 days, 3 weeks, and 3 months after an incident. 55 The process involves identifying a potentially traumatizing event based on criteria such as extreme exposure, incidents involving children, mission-related injury or helplessness, incident complexity, and first-time exposure. At each time point, participants complete a self-check-in using the stress continuum and are encouraged to take steps to return to baseline in the green zone. Patrollers can also be directed to the psychological first aid training program, which aims to assist with experiences of distress and trauma on the job. 56 Various psychological first aid programs have been found to improve mental health outcomes in one systematic review. 57 However, the review also highlighted how the studies had a high risk of bias and inconsistent intervention components, which made it difficult to evaluate the efficacy of such programs. Therefore, continued exploration of these programs is warranted.
Despite the lower levels of perceived work stress reported in this study, evidence continues to support how search and rescue participants are exposed to many psychological and physical stressors. 47 Ski patrollers in particular have also been shown to encounter acute and chronic stress in their roles in the literature.21,58 Due to the direct impact stress has on health, including sleep and heart health, it may be valuable to monitor levels of sleep and heart rate with biometric health screenings to establish baseline levels and appropriately evaluate any changes in response to traumatic events. 59
Future research may focus on determining which specific initiatives would best support patrollers’ health and wellbeing. As some patroller unions have advocated for increased wages, 60 potential initiatives include improving pay and worker benefits to alleviate the financial strain of high costs of living, gas, groceries, and the need to work additional jobs. 61 Organizations may also promote team-building activities to enhance collegiality and foster a sense of community support with an open culture around wellbeing and mental health.43,62,63 As one narrative review highlighted how first responders receive a variety of essential social support from family members, spouses, and /or friends, 64 encouraging such personal and community supports may be an important element to enhancing their wellbeing. Organizations can further ensure they provide adequate operational training for the job and explain potential risk exposures with transparency to assist in managing expectations and ultimately promoting wellbeing.65,66 Taking such steps may assist patrollers in operating in the green or “ready for work” zones on the stress continuum model.
Strengths & Limitations
One major strength of this work is the longitudinal study design, which allowed us to observe traumatic events and outcome variables from baseline to the follow-up period, supporting inferences from this study. 31 One limitation for this study was the small sample size and recruitment at only one resort in the United States over one half of the season. However, this pilot project collected valuable baseline evidence that may be leveraged to expand this project to a national study that enrolls a larger sample at additional sites, providing adequate power for the results. Data collection for the pilot study began in February 2024, which was around mid-point in the season for this resort, so data was not obtained at the start of the season. All respondents were also finished with their work by the time they completed the last survey (Survey 3) and so efforts should be taken to collect data over a full work season.
Additional limitations include the potential for recall bias, as survey questions asked about the prior month, and the use of self-reported data for traumatic events rather than objective measures. However, a previous study using 5 different samples found that self-reporting is a valid and reliable method for assessing trauma exposure. 67 Also, due to the long tenure of this particular sample working at this resort for over 11 years, we cannot separate the potential effects of cumulative traumatic exposures on participants’ health, which may have influenced our results. Another limitation is the lack of distinction between specific types of traumatic events, such as pediatric deaths or specific traumatic injuries, as this study focused on quantifying overall exposure. Future research could explore how different types of events influence wellbeing and other health outcomes of ski patrollers.
Conclusion
Results from this work highlight the need for continued evaluation of ski patrollers as a unique occupational group facing various physical and mental risks, as well as the importance of identifying ways to support their wellbeing. This study's finding that resilience protects against the impact of traumatic event exposure on wellbeing underscores the importance of continued research into fostering resilience in ski patrollers. Future work may also focus on recruiting ski patrollers at multiple sites, gathering data across their whole season, and collecting in-depth information on the types of traumatic events they experience.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Requests to access the deidentified dataset should be directed to Dr Elizabeth Keller (kellere4@g.ucla.edu).
Ethical Considerations
This study was approved by the University of California, Los Angeles Institutional Review Board (#24-000098).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the American Association of Avalanche Professionals (Record # 20242248). Dr Keller is also supported by the Targeted Research Training Program of the Southern California National Institute for Occupational Safety and Health Education and Research Center, grant agreement number T42 OH008412, from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the Centers for Disease Control and Prevention.
Informed Consent
A signed informed consent was waived by the IRB. Instead, participants read through the information sheet, detailing study procedures. By clicking “continue,” participants indicated their consent in this online research survey.