
Abstract
Introduction
The training practices and the level of medical oversight of search and rescue (SAR) organizations in the US National Park Service (NPS) Pacific west region is not known.
Methods
A database of SAR teams in the NPS Pacific west region was assembled using public sources. SAR team leaders received an electronic survey between May and December 2019. A descriptive analysis characterizing team size, technical and medical training protocols, and medical oversight was completed. Results are reported as median (interquartile range, range).
Results
Of the 250 SAR teams contacted, 39% (n=97) completed our survey. Annual mission volume was 25 (10–50, 1–200). Team size was 30 members (22–58, 1–405). SAR teams most frequently trained in helicopter operations (77%), low-angle rope rescue (75%), and avalanche rescue (43%). Nearly all teams (99%) had members with some medical training: first aid or cardiopulmonary resuscitation (89%), emergency medical technicians (75%), registered nurses or midlevel providers (52%), and physicians (40%). SAR members administered field medical care (84%), often in coordination with EMS (77%). Medical direction was present on a minority of teams (45%), most frequently by a provider specialized in emergency medicine (68%). Expanded medical procedures were permitted on 21% of SAR teams.
Conclusions
SAR teams across the NPS Pacific west region had composition and training standards similar to those surveyed previously in the US intermountain states. Healthcare professionals were present on most teams, typically as team members, not as medical directors. Few SAR teams use medical protocols in remote care environments.
Introduction
Search and rescue (SAR) operations in the United States occur under the auspices of multiple agencies, and to the authors’ knowledge there are no unified protocols for how SAR teams are organized or operate. They are most frequently housed within county sheriff’s offices, although this varies by state. Teams may have affiliations with federal, state, or local government, and unaffiliated, nonprofit groups also exist. Although numerous reports have characterized the demands of National Park Service (NPS) SAR teams, peer-reviewed literature capturing the diversity of US SAR teams outside of the NPS system is limited. 1 -3 The only publication to date primarily evaluating non-NPS SAR organization, training, and mission volume is a regional analysis of the intermountain west SAR services completed in 2013. 4 Our objective was to further characterize the prehospital SAR response system, with an analysis of SAR teams in the contiguous NPS Pacific west region states.
Methods
We assembled a database of SAR teams within the NPS Pacific west region using public Internet sources. This database included all identifiable SAR teams in the states of California, Idaho, Nevada, Oregon, and Washington, organized by both state and county. We searched local government webpages, including those of sheriff’s offices, county clerk’s offices, county and regional SAR webpages, and Facebook pages, to identify publicly listed email addresses for SAR team leaders. Search terms included “county name” followed by “search and rescue,” “SAR,” “mountain rescue,” and “sheriff’s posse.” When a publicly listed team leader or point-of-contact was not available via web search, we made telephone calls to the parent organization, typically a sheriff’s office or office of emergency services, to locate an appropriate email or phone contact. When a SAR organization with multiple specialty teams was encountered (eg, mountaineering team, K-9 team, dive team), each specialty team was considered unique and was represented as such in our database. Identifying information for each SAR team in the database included state, county, parent organization, subspecialty, email contact, and phone contact. After the database of SAR team leaders was compiled, each was sent an initial survey by email (Table 1). After this initial distribution of the team leader survey, we made telephone calls to all nonresponders through directly listed phone numbers that had been previously identified or by contacting the parent organization. Before closing data collection, a final email was sent to each nonresponder. Through this method, up to 3 contact attempts were made for each of the 250 teams identified in our region of interest.
Team leader survey
SAR, search and rescue.
The team leader survey consisted of general questions regarding the specialty of the SAR team, annual call volume, volunteer and paid member count, and specific questions regarding the medical training of members and the role of medical specialists on the team (Table 1). Data collection took place between May and December 2019, with entries cataloged in the research electronic data capture (REDCap) application. Results were both quantitatively and descriptively analyzed using Microsoft Excel. Quantitative analysis included mean±SD or median (interquartile range, range) for team size, call volume, number of volunteers with specific medical training, and the proportion of respondents answering in the affirmative for our categorical questions (eg, proportion of teams requiring members to be trained in first aid). Descriptive analysis was required for free-text responses, including questions regarding training provided by SAR teams and types of expanded medical protocols permitted under medical direction. The University of California San Francisco, Fresno, institutional review board approved the study design and protocol.
Results
Of the 250 SAR teams contacted, 39% (n=97) completed our survey. Response rates by state were as follows: California (44%, n=33/75), Oregon (44%, n=24/54), Nevada (38%, n=3/8), Washington (36%, n=29/81), and Idaho (25%, n=8/32).
Team types included mountaineer (66%), off-highway vehicle (7%), K9 (7%), maritime (4%), mounted posse (4%), air (3%), cave rescue (2%), urban (1%), and unspecified (5%). Median annual mission volume was 25 (10–50, 1–220), and median size was 30 volunteer members (22–58, 1–405) and 0 paid members (0–1, 0–25). Large teams were outliers in the data set; only 3 teams were composed of over 300 volunteer members, and 8 teams reported over 100 volunteer members (Figure 1). The remaining teams (85%) reported having fewer than 100 volunteer members. Technical teams were trained in helicopter operations (78%), high-angle rope rescue (62%), avalanche rescue (44%), swift water rescue (41%), and dive rescue (14%) (Figure 2).
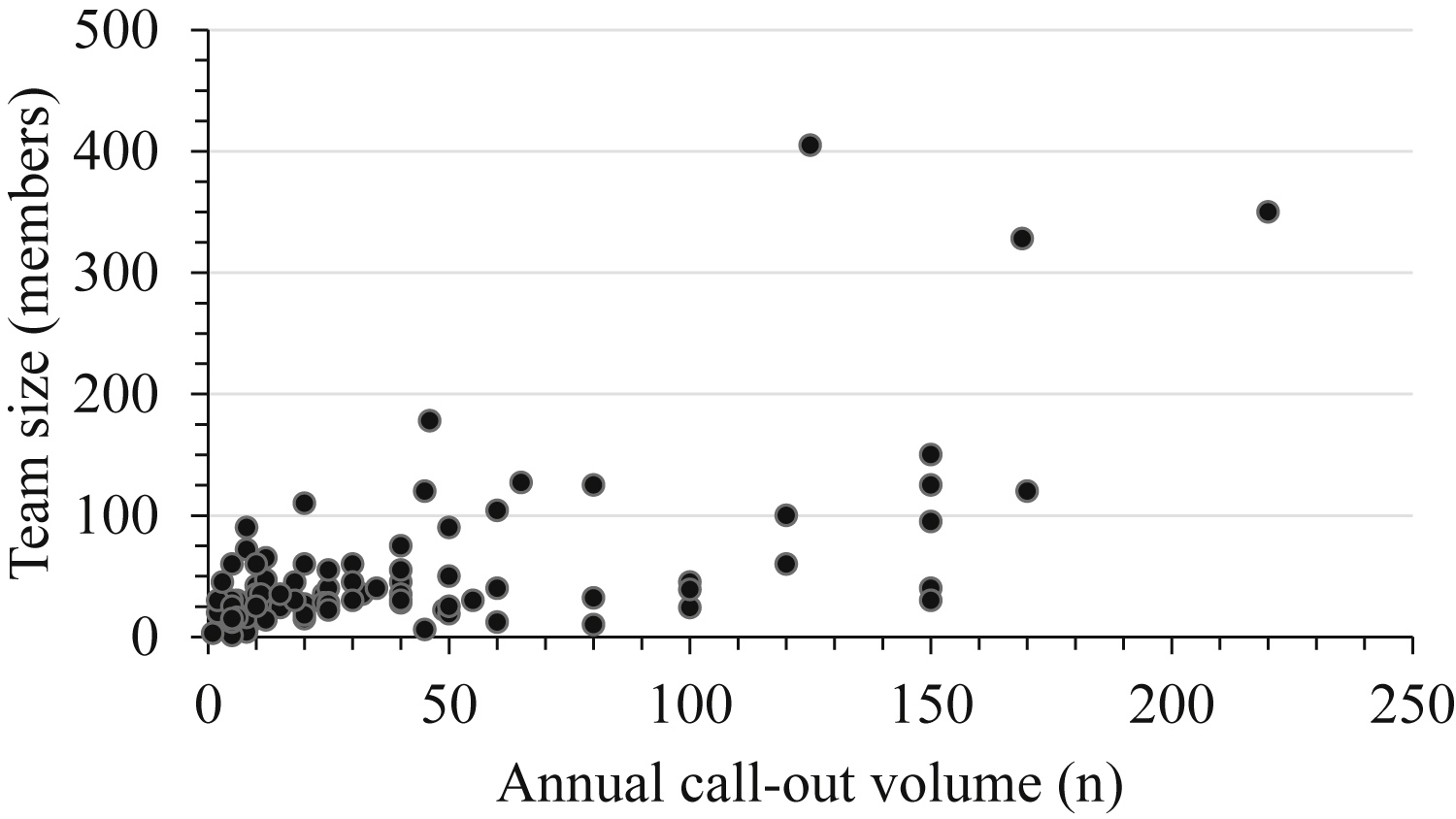
Annual call volume relative to team size. Data are presented using each reporting search and rescue team as an independent point.
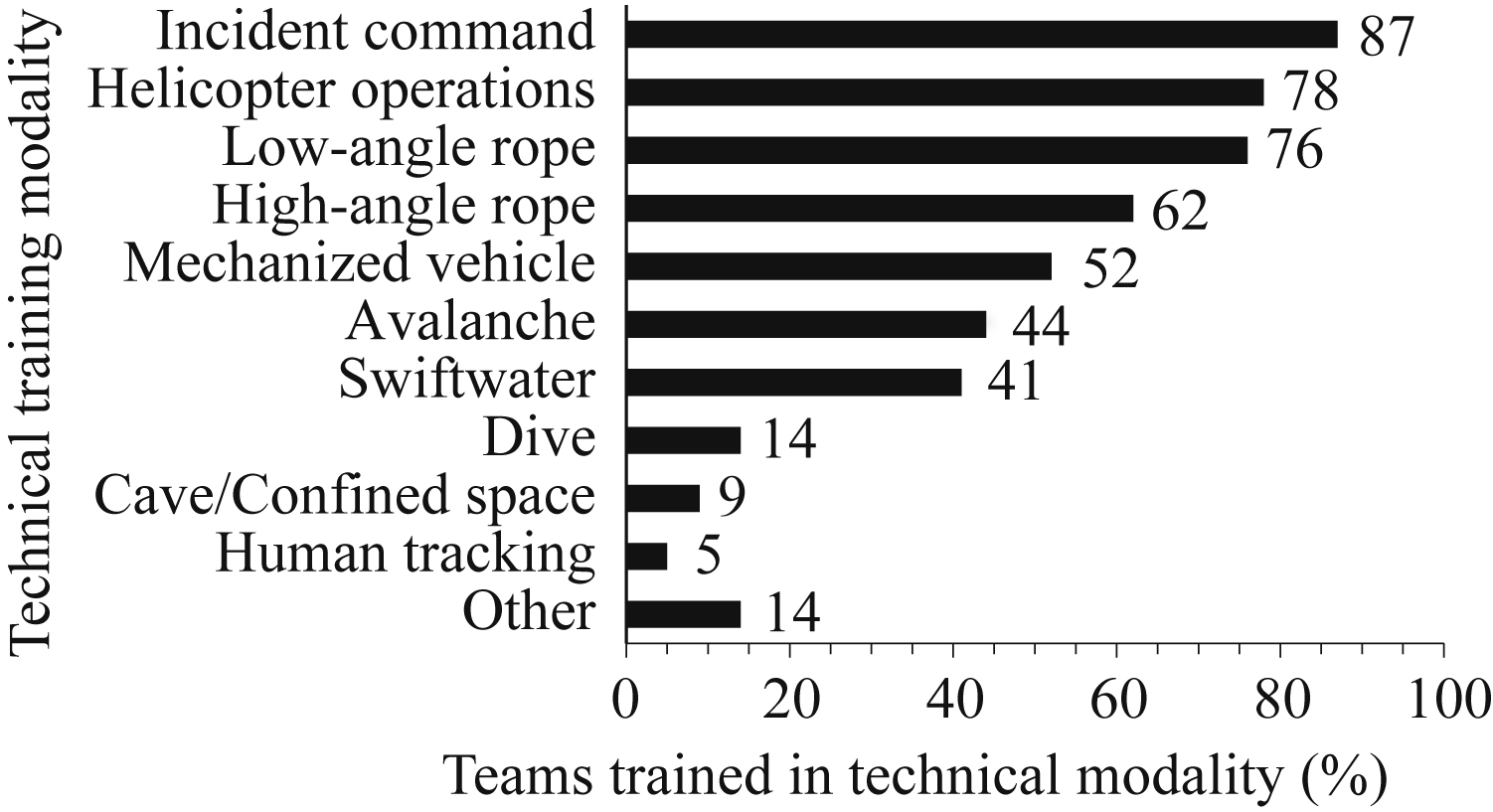
Percentage of teams that trained members in specific modality. The majority of teams reported training members in more than 1 discipline. Free-text responses for other included K9 search, human tracking, equine handing and packing, open water/surf rescue, GPS/compass use, orienteering, and urban rescue.
Among the SAR teams in the NPS Pacific west region that responded to the survey, one-third (34%) required members to have minimum medical training, with first aid or cardiopulmonary resuscitation (CPR) being the most common requirement (29%). Medical training for members was provided by 85% of teams; first aid or CPR was the most common (78%) training provided. Medical training included emergency medical responder (20%), emergency medical technician (EMT) (14%), advanced EMT (AEMT), or EMT paramedic (EMT-P) (4%), and “other” (19%), which included EMT recertification for members who had lapsed EMT certifications, tactical casualty combat care (TCCC), prehospital trauma life support, automated external defibrillator use, wilderness first responder, wilderness first aid, and advanced wilderness life support.
The overwhelming majority of teams (99%) had medically trained members: first aid or CPR (89%); EMT, AEMT, or EMT-P (75%); registered nurses, nurse practitioners, or physician assistants (52%); or physicians (40%) (Table 2). The number of members per team with each type of medical training is shown in Figure 3. Members with wilderness medicine training were present in most teams (57%, n=56). The median number of members per team with completed wilderness medicine training was 2 (0–7, 0–120).
The presence of medically trained members on SAR teams
Data are presented as the number and percentage of teams per state that reported having at least 1 team member with given certification/education.
AEMT, advanced EMT; CPR, cardiopulmonary resuscitation; EMR, emergency medical responder; EMT-B, EMT-basic; EMT-P, EMT-paramedic; MD/DO, physician; PA, physician’s assistant; RN, registered nurse; WFA, wilderness first aid; WFR, wilderness first responder.
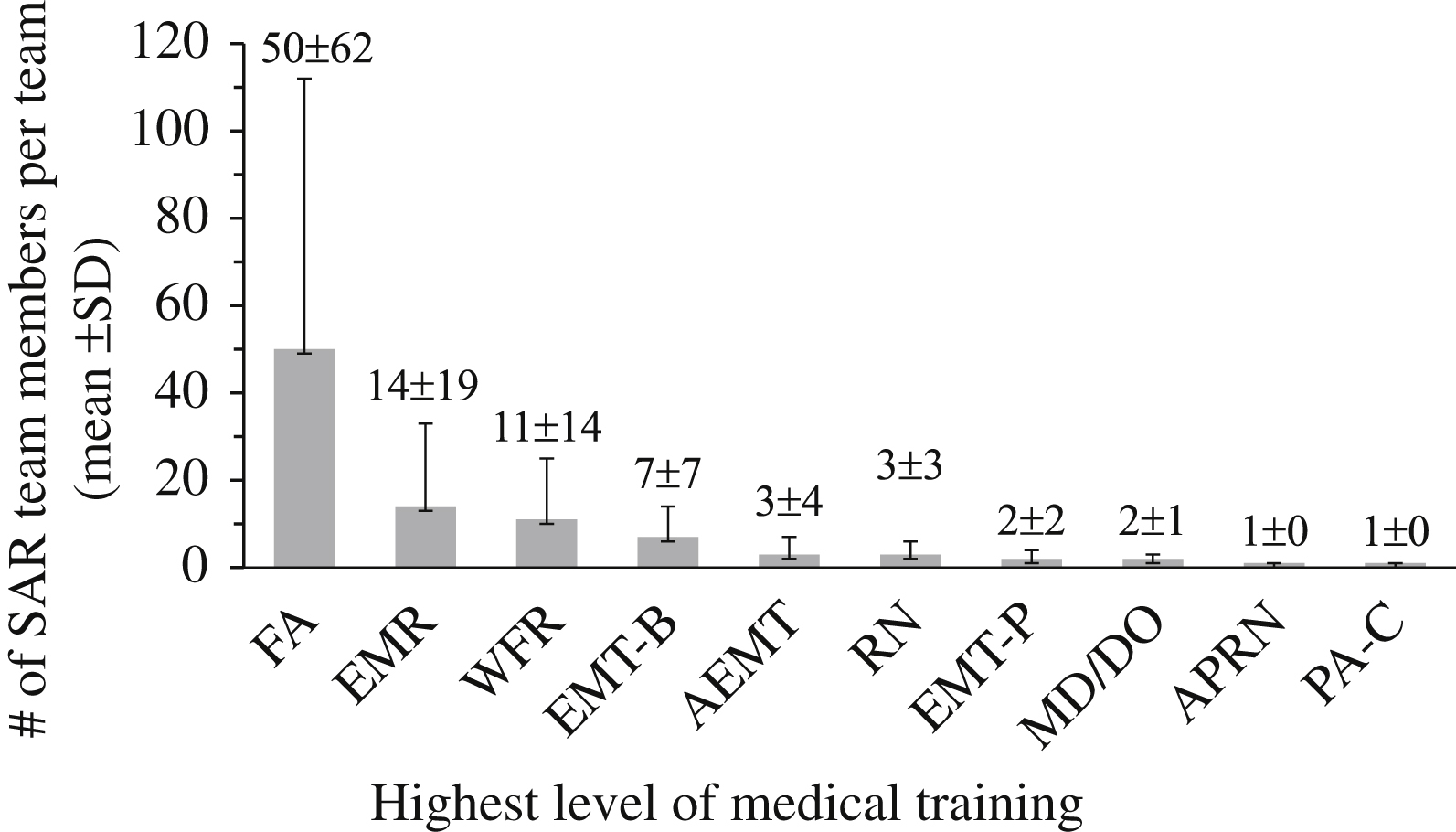
Number of individuals on reporting teams (mean±SD), categorized by level of medical training. FA, first aid; WFR, wilderness first responder; EMR, emergency medical responder; EMT-B, EMT-basic; AEMT, advanced EMT; EMT-P, EMT-paramedic; RN, registered nurse; MD/DO, physician; APRN, advanced practice registered nurse; PA-C, physician’s assistant.
SAR team members provided direct patient care on the majority of responding teams (84%, n=81/97). Local EMS were also involved in direct patient care on 77% of SAR teams. Other organizations involved in direct patient care included air ambulance and air medics. Only 23% of teams reported joint training with local EMS for rescue scenarios (n=22).
Of the 97 responding teams, 45% reported having SAR medical directors (n=44). These individuals were mostly physicians (77%, n=34) and trained in emergency medicine (68%, n=25) or family medicine (15%, n=5). Forty-four teams reported having a medical director who was typically involved in updating medical protocols (84%, n=37), training with the SAR team (69%, n=29), and participating in SAR missions (50%, n=22). When available, the SAR medical director participated in medical consultation on 56% of reporting teams (n=25) and prescription of medications for use in field-based patient care on 23% of teams (n=10).
SAR medical protocols allowed for expanded scope-of-practice on 21% of reporting teams (n=20), permitting members to perform medical care that exceeded individual team member credentialing. Dislocation reduction (n=14) and epinephrine administration (n=8) were most frequently reported, but SAR teams also had expanded protocols for airway stabilization (n=2), establishing intravenous access (n=2), and analgesia administration (n=1).
Discussion
The majority of teams responding to our survey of NPS Pacific west region SAR organizations were relatively small (<50 members). They typically trained for a diverse range of rescue scenarios and basic first aid care, similar to teams operating in the US National Parks and Canadian National Parks.1,5,6 Although a large proportion of organizations had professional medical providers among volunteer members, far fewer reported having physicians (MD or DO) as team members or serving as established medical directors. Respondents reported frequent coordination with local EMS, but joint training experiences were more limited. These findings suggest that opportunities to improve care in remote and austere environments where long transit times are anticipated could be achieved through expanded medical oversight of responding SAR teams and improved coordination of care with EMS.
The results of our survey among NPS Pacific west region SAR teams were largely consistent with the earlier findings of the intermountain region survey. 4 Although these surveys were not contemporaneous, SAR teams that responded to our survey had slightly higher rates of minimum medical training among volunteers (basic first aid or CPR) compared to responding teams in the intermountain region (89 vs 79%). Our responding teams were more likely to report having members with wilderness medical training, including wilderness first aid, wilderness first responder, or advanced wilderness life support (57 vs 23%). This difference may be due in part to growth in the availability and popularity of wilderness medicine training in the past decade. Based on anecdotal experience, we think that opportunities for training in wilderness medicine have increased, but we are not aware of any studies that support this perception. The NPS intermountain and Pacific west surveys reported that teams operated under established medical direction at similar rates (45 vs 41%). In both regions, medical directors most often specialized in emergency medicine. Expanded medical protocols were more common among intermountain teams (45 vs 21%), which may reflect a need that accompanies longer transport times in more remote areas of the intermountain region.5,7,8 Local EMS was involved in care during most missions in both regions; however, there were low rates of EMS/SAR joint training in both regions (35% NPS intermountain and 23% NPS Pacific west regions).
The need for medical care during SAR missions varies greatly by mission.5,7 Reviews of EMS in NPS units found that the acuity and severity of injuries in the field are generally low, suggesting that using volunteers, as seen in the NPS Pacific west region, is likely appropriate.2,3,9,10 Volunteers with more advanced medical training, including physicians, often chose to limit their practice to first-aid level interventions; in other cases, scope of practice was restricted by the SAR parent agencies.
Although acuity of illness and injury in the wilderness setting is typically low, examples of expanded medical protocols being implemented in the field by civilian SAR teams show that these interventions are feasible and can play an important role in stabilizing critically injured patients when transit times are prolonged. 11 Standardized expanded medical protocol models exist in both military and NPS wilderness settings and have been shown to save lives in the prehospital environment. 12 The TCCC model uses tourniquets, hemostatic agents, nasopharyngeal airways, analgesia, and antibiotics in the battlefield. 12 The NPS Parkmedic program is similar, training first responders as AEMTs and expanding scope of practice through additional procedural and pharmacologic training.3,13 The additional training with offline medical protocols and online support via radio communications with local emergency departments allows Parkmedics to provide an expanded level of care in the backcountry during SAR missions, without requiring the presence of advanced providers on site. Parkmedic and TCCC protocols are used by well-trained professionals (EMTs and soldiers, respectively), but there are more manuals and guidelines for expanding medical protocols under medical direction in civilian EMS and SAR systems. The Washington State Department of Health prolonged prehospital emergency care course and the International Commission for Mountain Emergency Medicine multiple trauma management guidelines promote evidence-based practices for civilian rescuers in remote environements.14,15 Similarly, the Wilderness Medical Society (WMS) has clinical practice guidelines for current, evidence-based care in remote environments. 16
The adoption of evidence-based, expanded medical protocols similar to those described by WMS and other sources may be limited by the scope of practice under which US first responders have historically operated. The results of our survey suggest that within the NPS Pacific west region, basic first aid is commonly employed by SAR volunteers until EMS can be reached and the patient transported to definitive care. Advanced life support may be delayed when teams operate without expanded medical protocols. The results of a 2018 study conducted in the central Pyrenees suggested that providing advanced life support in the field when transport times are prolonged may improve patient outcomes. After the addition of physicians and nurses to provide advanced prehospital care to mountain rescue teams, there was a significant decrease in mortality rate during SAR missions (9 to 3%). The author predicted cost savings over the next 15 y to be in excess of $203 million per year. 17 A similar professionalization is not currently feasible in the United States for numerous reasons, including relatively low population density and inadequate funding for similar interventions. However, many NPS Pacific west region SAR teams have advanced providers. The intervention in the Pyrenees supports the notion that providing advanced care in prehospital settings might decrease mortality.
Our survey found that there was limited medical director oversight among NPS Pacific west region SAR teams. Few teams reported having expanded medical protocols for their volunteer members. The experiences of TCCC, NPS Parkmedics, and mountain rescue organizations in the Pyrenees suggest that that addition of medical protocols suited to the unique environment might promote the provision of advanced prehospital care. This view aligns with the National Association of EMS Physicians position statement. 18 Teams can use existing clinical practice guidelines, such as those provided by the WMS or by local and state jurisdictions to expand prehospital emergency care.
Limitations
Our survey had a response rate of only 39%. The intermountain region survey had a higher response rate at 56%. 4 This is a major limitation that provides significant room for error in our characterizations. The research team was unable to identify specific patterns for nonresponse to our survey, which may represent a flaw in our methods for collecting SAR team leader contact information. Our survey assumes that SAR team leaders have the resources and time to maintain accurate and current records about their active membership, which may not be the case in all circumstances. The validity of the data collected in our survey depends on respondents being specific in their responses. Our survey relied on free-response fields for respondents to describe expanded medical protocols. This presents opportunities for mischaracterization or misinterpretation of responses by the research team. Survey methodology is subject to bias. Survey respondents may misinterpret questions, enter data incorrectly, or be subject to nonresponse bias, which occurs when people are unwilling to respond to a survey owing to a factor that makes them differ greatly from people who respond.
This survey only queried organization and training of SAR teams and did not study mission-specific demands or outcomes. We did not collect data on the medical certifications of rescuers on specific missions. This limits discussion of mission-specific outcomes before and after implementation of expanded medical protocols.
Conclusions
SAR organizations in the NPS Pacific west region were typically trained for a variety of rescue scenarios according to local geography, including high-angle rope rescue, whitewater rescue, and avalanche rescue. The composition and training standards of teams was similar to the composition and training standards of teams in the intermountain region. Fewer SAR teams in the NPS Pacific west region had medical directors compared to teams in the intermountain region, despite the presence of medical professionals as members. Few SAR teams in the NPS Pacific west region used expanded medical protocols. Clinical practice guidelines and models are available to teams that wish to expand medical protocols under appropriate medical direction.
Footnotes
Acknowledgements
Acknowledgments: We thank the SAR team directors who participated in our study and acknowledge the countless acts of Good Samaritan medical care provided by their members.
Author Contributions: Data collection (all authors); manuscript preparation and revision (all authors); approval of the final version of the manuscript (all authors).
Financial/Material Support: None.
Disclosures: None.