
Abstract
Introduction
Shoulder dislocations are common ski hill injuries. Rapid reduction is known to improve outcomes; however, advanced providers are not always available to provide care to these patients. In 2017, nonmedical ski patrollers at Sunshine Village ski resort in Alberta, Canada, were trained to perform anterior shoulder dislocation (ASD) reductions. Program success was determined by a chart review after the 2020 ski season.
Methods
This study retrospectively reviewed data on patients who presented to Sunshine Village ski patrol with a suspected ASD and who met the study inclusion criteria from November 2017 through March 2020. Data were collected from ski patrol electronic patient care records regarding general demographics, reduction technique used, analgesia administration, and reduction success rates.
Results
Ninety-six cases were available for review after exclusions. Trained nonmedical ski patrollers successfully reduced 82 of these cases, resulting in an overall reduction success rate of 89%. Sixty-three (66%) of these patients had experienced first-time dislocations. Eighty-two (87%) patients were male, with a median age of 25 y. The most used technique was the Cunningham method (75%), and analgesia was administered to 70% of patients.
Conclusions
This retrospective study documents the results of a quality assurance review of the treatment of ASD at Sunshine Village ski resort. With a success rate of 89%, the evidence supports the conclusion that nonmedical ski patrollers can successfully perform ASD reductions. We believe training ski patrollers to reduce ASD improved patient care in our austere environment by providing early definitive treatment with a high success rate.
Introduction
Skiing and snowboarding are among the favorite pastimes of many outdoor enthusiasts. Unfortunately, injury rates have been reported at around 2 injuries per 1000 rider days. 1 –3 It has also been reported that 7% of these injuries are shoulder dislocations, 4 which ranks this injury in the top 5 for alpine skiers and snowboarders. 5 Approximately 19 million people visit Canada’s 275 ski resorts annually, resulting in a substantial number of recreational users presenting to ski patrol with anterior shoulder dislocation (ASD). Early reduction of ASD injuries can reduce pain, ease evacuation and transport, improve ease and time to reduction, and potentially reduce neurovascular injury and long-term complications. 6 –8 Shoulder reduction is not within the scope of the Canadian Ski Patrol Service, which is the standard of care at ski resorts in Canada, leaving traditionally trained first responders only able to provide supportive care for ASD. Owing to the geographic location of many Canadian ski resorts, injured skiers and snowboarders will often experience significant delays in accessing medical care. Most Canadian resorts do not have physicians available to provide care, nor are they available on transport ambulances. Without consistent physician availability at these resorts, training ski patrollers to reduce obvious ASDs provides an opportunity to improve care among this cohort of patients.
This project was performed at Sunshine Village (SSV) ski resort in Banff, Canada, a large ski resort located in the Canadian Rockies. The resort sees over 550,000 recreational skier/boarder visits annually and has the longest nonglaciated ski season in North America. Resort ski patrol assess and treat all injuries and illnesses that present to the ski resort clinic and treat approximately 1200 patients each season.
Treatment protocols for ski patrol members were adapted to include reduction attempts for clinically obvious ASD in the fall of 2017. The ASD protocol (Figure 1) was developed to provide ski patrollers the option to perform ASD reduction before patient transport to the local hospital and to be used when a physician is not immediately available to provide this treatment. The objective of this protocol was to shorten the time to a definitive procedure, reduce pain and suffering, and reduce complications when faced with prolonged transport times and/or difficult field extrication. This protocol was developed by the ski patrol medical director, an experienced emergency medical services/flight physician. Choice of analgesia, inclusion and exclusion criteria for use of the protocol, training standards, and choice of biomechanical techniques was determined by the medical director based on his personal experience and research.
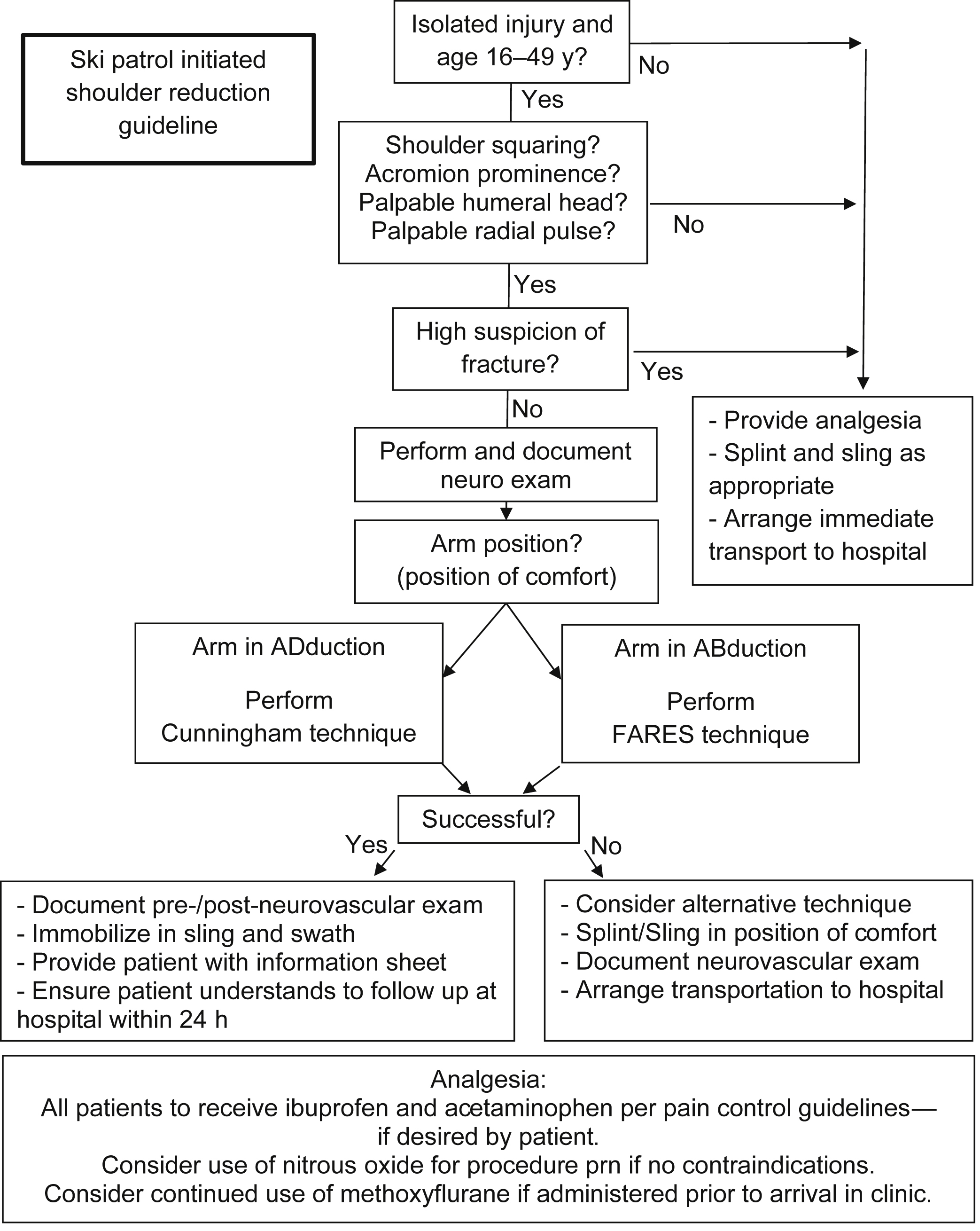
Sunshine Village ski patrol anterior shoulder dislocation protocol. The following is the guideline used by nonmedical ski patrollers at Sunshine Village Ski Resort to assess and treat anterior shoulder dislocations when they occur at the resort.
Searches of the literature on out-of-hospital shoulder reductions by nonmedically trained individuals revealed few results. No evidence could be found on first responders performing reductions as the standard of care in Canadian ski resorts. After the apparent success of the ASD reduction program at SSV, the authors believed the results of the quality assurance review should be shared. The primary objective of this study was to determine whether ski patrollers can be taught to examine and reduce obvious ASDs in a remote hillside clinic.
Methods
This retrospective study was reviewed and approved by the University of Calgary as a quality improvement project. As such, the project was exempt from ethics review by the conjoint health research ethics board of the University of Calgary (Tricouncil policy statement 2018, Chapter 2, Article 2.5).
Our literature search used Medline, BMS Engine, Biomedical Reference Collection, HealthSource: Nursing/Academic, Google Advanced, and CINAHL for “pre-hospital, OR wilderness OR out-of-hospital” AND shoulder reduction AND “paramedic OR rescuer OR EMT OR ski patrol.”
Only ski patrollers with 3 or more years of experience at a wilderness first responder level were permitted to partake in this advanced training. Ski patrollers who were trained as advanced care paramedics (EMT-P), registered nurses (RN), or physicians (MD) were not included in the program or subsequent audit.
The training consisted of 3 phases. First, qualified patrollers attended educational sessions on shoulder anatomy, shoulder assessment, and ASD identification. Next, each patroller assisted an on-hill physician in 6 ASD reductions that presented to the medical clinic. Finally, patrollers performed an additional 6 ASD reductions under the direct supervision of an on-hill physician. All cases during this training were then further reviewed by the medical director and ski patrol director before the patroller was approved to independently reduce ASDs. A total of 10 patrollers were trained and provided care over the study period.
Assessment and diagnosis of ASD was performed by the patroller after adequate history, exposure, and examination of the injured patient in the warm environment of the medical clinic. Diagnosis was made by determining the history and signs and symptoms of ASD, including the mechanism of injury, pain, limited range of motion, and step deformity of the shoulder complex. All patients were examined for neurovascular deficits, obvious associated fractures, and other injuries. Radiologic confirmation was not performed because imaging was not available at the ski resort clinic.
The 2 positioning and muscle relaxation techniques selected for the protocol were the Cunningham and the FARES, which were chosen to account for subglenoid and subcoracoid dislocations. 9 –12 These biomechanical techniques have been described using minimal or no analgesia/sedation, minimal traction and force, and simple positioning to facilitate reductions. Selection of technique was based on patient and arm positioning (Figures 2 and 3).

Cunningham technique. The Cunningham technique relies on massage with the arm in a neutral position to reduce spasm and allow spontaneous reduction. This technique relies on good communication with the patient and coaching them to relax and maintain good posture with shoulder blades retracted, which is critical for success. Steps: 1. Perform detailed shoulder assessment. 2. Sit patient upright in a chair opposite the practitioner. The hand of the patient’s affected arm should rest on the practitioner’s shoulder. 3. The practitioner can rest their arm in the bent elbow space of the patient’s affected arm. No more traction is necessary. Constantly encourage patient to maintain good posture and relax. 4. The practitioner then massages the affected shoulder in sequence: first, trapezius; second, deltoid; third, biceps; and, fourth, triceps. Use pressure as tolerated. Repeat. Video available at:
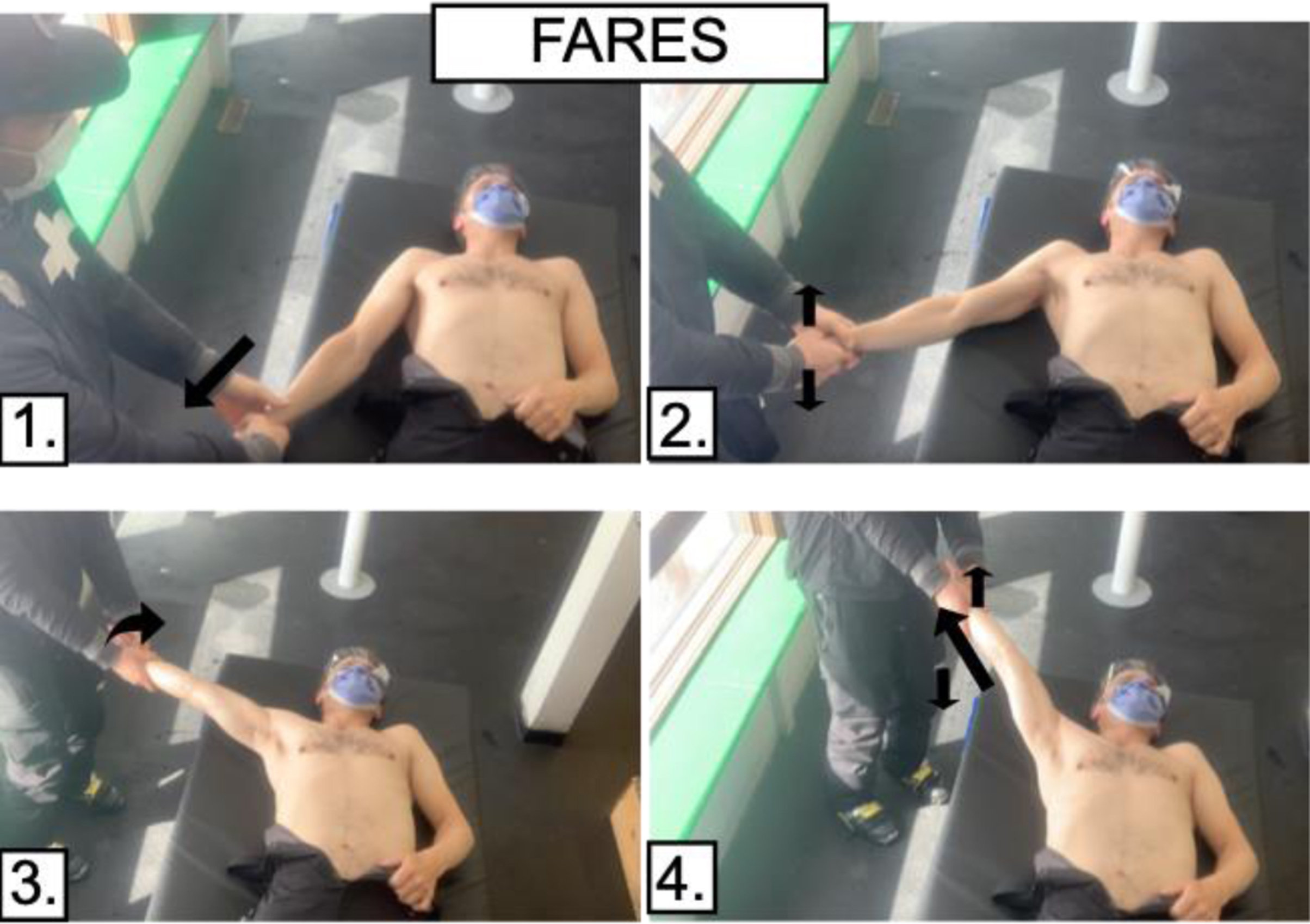
FARES technique. The FARES method requires patients to be supine on an elevated platform for the practitioner to have the mobility to perform the procedure. The oscillations resemble a handshake when performed. Steps: 1. Patient should be lying supine on a raised surface with the affected arm adducted alongside them. 2. Practitioner to take patient’s wrist. While maintaining a gentle, steady longitudinal traction, the practitioner should begin to abduct the injured arm. 3. While abducting and maintaining slight traction, small oscillations of the arm should be made 2 to 3 times a second, lifting and lowering the arm 10 to 15 cm. 4. When the arm is abducted to 90°, externally rotate and continue traction, oscillations, and abducting arm. Reduction usually occurs at approximately 120° of abduction. Video available at:
Success was determined by signs and symptoms, including pain reduction, recovery of normal range of motion, and normal appearance. Patients with unsuccessful reduction attempts by the ski patrol were referred to an on-hill physician, if available, or transferred directly to the hospital after appropriate analgesia and splinting. All patients agreed to immediate post-care follow-up, including referral to a clinic that could provide appropriate imaging and orthopedic consultation.
At SSV, a computer database (EDGEauditor, Orangeville, ON, Canada) was used to record patient information and accident and treatment details on all patients seen by the patrol service. We retrospectively reviewed all patient visits to ski patrol from November 2017 through March 2020. First, we identified all patients with a chief complaint of “shoulder injury.” Further screening then included all patients specified as having a dislocation. We then excluded patients who met any of the following criteria: shoulder reduction performed on the ski slope suggesting spontaneous reduction, no reduction attempted owing to risk of clinically significant fractures, and no reduction attempted owing to patient refusal to consent to the procedure. These patients were removed from the study because the protocol for ski patrol reduction excluded these patients from a reduction attempt. We also excluded patients who had an ASD reduction performed by an intermediate or advanced practitioner (MD, EMT-P, or RN) or who received intravenous or intramuscular analgesia. Finally, any patient for whom exclusion criteria could not be determined owing to incomplete documentation was also excluded from the study. Included charts were reviewed for the following information: age, sex, type of sport (skier vs snowboarder), characterization of dislocation (first-time dislocation vs recurrent dislocation), reduction techniques used during attempt (Cunningham, FARES, other), and success of reduction attempt.
Microsoft Excel (Microsoft, Redmond, WA, USA) was used for data collection. Continuous demographic data are presented as median [interquartile range] because the sample group was not evenly distributed within the inclusion criteria. Count data are presented as frequency (percentage). Overall success rates of onsite reductions are presented using frequency (percentage [95% CI]). Logistic regression analysis was completed to understand the association between reduction technique and an unsuccessful reduction. Reduction techniques were grouped into 1 of 3 categories: Cunningham, FARES, or other (includes combined Cunningham + FARES, other, Cunningham + other, and combined Cunningham + FARES + other). Associations between technique and an unsuccessful reduction are given using odds ratios (ORs) with 95% CIs. Statistical analysis was completed using SPSS 25.0 (IBM, Armonk, NY). Statistical significance was defined as P<0.05.
Results
A total of 117 patient cases were identified by the ski patrol as having an ASD. After applying the exclusion criteria, we identified 96 patients who had an onsite reduction attempt. Male and female patients were pooled because the total number of female patients included in the study did not provide a large enough sample to be statistically analyzed (Table 1). The median age of patients treated was 25 y (IQR 21–29 y). Males accounted for 86% of patients, and snowboarders and skiers accounted for 62% and 38% of patients, respectively. Sixty-three (66%) patients presented with a first-time ASD injury.
Summary of data collected
Of the 96 reductions performed onsite, 82 reductions were successful using the ASD protocol (89% [95% CI 81–95%]). Reduction success for first-time dislocations and recurrent dislocations was 90% and 87%, respectively, which did not show a statistically significant difference. The odds of a successful reduction were 1.33 times greater in the first-time dislocation group, but with a very wide CI (95% CI 0.3–5.1).
The most common reduction technique used was the Cunningham (75%), whereas the FARES technique accounted for 9%. The success rate of the first attempt was 75% (95% CI 65–83%). The odds of having an unsuccessful reduction were not significantly increased by use of the FARES (OR=2.4 [95% CI 0.2–26.4, P=0.46]) or another (combination) technique (OR=2.4 [95% CI 0.4–15.3, P=0.38]). The odds of failure were not significantly different between techniques selected (OR=2.5 [95% CI 0.2–26.4; P=0.46]).
Analgesia was administered in 66 patients, with nitrous oxide being the most common (61%), followed by a combination of ibuprofen, acetaminophen, and nitrous oxide (14%). No analgesia was administered to 31% of patients.
Discussion
Reduction of ASD is not uncommon in the prehospital environment. However, there is limited documentation of protocols or other support for nonmedical personnel performing reductions when physicians are not available. Our literature search found only 6 peer-reviewed articles pertaining to the topic.7,13–17 All 6 articles report a similar lack of available evidence. This lack of evidence may be a factor in why shoulder reductions have not been widely adopted by medical directors in prehospital settings.
The demographics of our patient cohort appeared to be consistent with the ASD literature, although our age range was slightly lower than most.14,16,18–22 Our median age (25 y) corresponded with data indicating that younger males (20–30 y) appear to be most likely to experience ASD injuries.21,23,24 The ratio of skiers and snowboarders in our study, as well as the observation that snowboarders are more likely to injure their upper extremities compared to skiers, is also consistent with other reports.4,25,26 Finally, the number of patients who experienced their ASD as a first-time injury (66%) is comparable with the literature discussing ASD presentations in the emergency department. 22
The 3 phases of training established for ski patrollers to independently reduce ASD were chosen to ensure that correct application of the techniques was understood and performed; improper application could reduce success rates and ultimately prolong treatment. A newly developed commercial task trainer (
We recognize that complete management for ASD should occur in a facility that can provide imaging and orthopedic follow-up. Most of the population lives in urban settings and can access this standard of care in a reasonable period. In remote and rural locations, meeting this goal is often not possible. It has been suggested that prehospital management of ASD could decrease time to reductions by 130 min versus when performed in the hospital. 13 Unfortunately for ASD patients, prolonged time to reduction (>60 min) has been documented to increase complications and make the injury more painful as muscle spasm increases.8,27,28 Although analgesia via ibuprofen, acetaminophen, nitrous oxide, and, recently, methoxyflurane provides some relief and is available to some ski patrol services, the definitive treatment for ASD is joint reduction.
Historically, standard methods for reducing ASD have been traction/countertraction and leverage techniques that require procedural sedation. As a result, they commonly require direct physician involvement for medication administration, monitoring, and postprocedural recovery. 29 –31 Recent literature continues to support moving away from traditional traction/countertraction and leverage methods and moving toward biomechanical techniques such as FARES and Cunningham for ASD reduction.12,16,31,32 These techniques have become popular because they are less painful for patients, require fewer personnel, and decrease the risks associated with conscious sedation.10,12,16,19,29,33 This makes biomechanical reduction techniques ideal for use by nonmedical personnel, or in a low-resource environment.
Results using the Cunningham technique have been extremely varied. Success rates of 35 to 100% exist in the literature.34,35 The FARES has less published data on its success rate, but 1 randomized control trial found a success rate of 89%. 33 A comparison of the success rate of our ski patrol to the ASD reduction success rates in the literature suggests that ski patrollers can reduce ASD consistently.16,29,30,32–35
Although biomechanical techniques may be more tolerable without analgesia, pain management was available for use in this protocol. Administration of over-the-counter ibuprofen and acetaminophen to all patients was encouraged, and nitrous oxide and methoxyflurane were available for patrollers to administer if required. It is noteworthy that none of these medications (acetaminophen, ibuprofen, nitrous oxide, and methoxyflurane) required administration by an advanced practitioner (MD, RN, or EMT-P). Furthermore, most of these medications are available to wilderness first responders, including ski patrollers. Beyond over-the-counter medications such as acetaminophen and ibuprofen, nitrous oxide and methoxyflurane have become popular owing to their quick onset of action and the ability of patients to optimize pain relief in a dose-response manner. Methoxyflurane shows great promise and is only recently available in Canada. Its use by SSV ski patrol as a means of analgesia was introduced halfway through the study period. Because the reduction of ASD may prove more difficult over time, 8 the relatively short onset of action of inhaled analgesia seems to be preferred by practitioners and is anecdotally very effective within the scope of our review.
The results of this study are likely not a surprise; however, there are often perceived barriers for first responders to perform ASD reductions in the field, which we would like to address here. These barriers include the inability to provide imaging and the risk of causing a fracture or worsening the injury.
The authors acknowledge that reductions without prereduction imaging are controversial. Although common practice may vary, it is still recommended that care of sports-related shoulder dislocations in the emergency department include prereduction x-rays.24,28,36,37 It is not uncommon, however, for physicians experienced with shoulder reduction, or those in resource-limited settings, to choose to reduce obviously dislocated shoulders before imaging. This practice is also supported in the literature.16,18,28,38,39
One stated concern for attempting reduction without prereduction imaging is the presence of a dislocation-associated fracture. Indeed, the frequency of ASD-associated fractures has been reported as high as 30%. 22 However, most of these fractures (which include Bankart lesions, Hills-Sachs lesions, and greater tuberosity fractures) do not affect acute management of the shoulder dislocation.22,34,40 Although these associated fractures may increase the risk of dislocation recurrence,8,30,40 they are generally not considered for treatment by orthopedics until after the initial injury has been reduced. 37
In addition to concerns regarding ASD-associated fractures, concerns such as causing neurovascular or other injury during reduction appear to be unfounded when nontraction, biomechanical-style techniques are employed.14,28,34,38 To our awareness, there are no case studies or other reports in the literature that indicate biomechanical techniques have been associated with neurovascular or other injuries. In addition to these newer biomechanical techniques being safe, they have also proven to have great first-time-attempt success, even without analgesia or sedation.12,16,19
The ASD protocol attempted to ensure patient safety by screening, and subsequently excluding, any patients at high risk of clinically significant fractures. These injuries, which include humeral neck, clavicle, and scapula fractures, significantly increase the difficulty of performing closed reductions without conscious sedation. Providers used the following signs, symptoms, and mechanisms for screening: report of direct trauma to the shoulder, severe disproportionate pain, age over 50 y, crepitus in or near the joint, or obvious deformity not consistent with a “squared shoulder” or Sulcus sign. These criteria are like those in other prehospital reduction studies. 16 Screening assessment tools such as the Quebec rule or the modified Fresno-Quebec rule do not apply well in our context because they automatically exclude any sports-related cause of injury.36,41 To the authors’ knowledge, no validated assessment tool has been developed to determine if a fracture exists. Evidence does demonstrate, however, that trained personnel who have a high clinical suspicion of uncomplicated ASD are often shown to be correct after x-ray confirmation. 18
Limitations
There were several limitations to our data, including, most importantly, the study design. As a retrospective chart review, we were unable to compare our results to a control group, compare success rates of reductions on first-time ASD versus recurrent ASD, or investigate the effectiveness of 1 technique after the failure of another. In addition, we were unable to review medical charts from the hospital to determine if any complications were noted. Inconsistent charting was also problematic, resulting in difficulty in determining the precise time from initial injury to reduction, changes in pre- and postreduction pain, and neurovascular examination results. Improved reporting standards now implemented by the SSV ski patrol will hopefully help to answer these questions in the future.
Age exclusion criteria (<16 y and >50 y) may have limited the collection of data from a broader age group. A further limitation is that the ASD injuries included in the study were not confirmed with x-ray imaging and were instead confirmed by practitioner assessment. As a result, we cannot definitively conclude that each shoulder reduction attempt was performed on a true ASD. With regard to data collection, the initial database search criteria for “shoulder injury” may have also failed to capture ASD injuries that had been labeled differently when initially recorded in ski patrol patient records.
In terms of practitioner demographics, there were no female patrollers within the group of 10 patrollers initially trained to reduce ASD. Although patrollers were selected based on factors such as years of experience, this lack of female practitioners may have led to unconscious gender bias when female patients were treated by male practitioners. Furthermore, the small number of female patients included in the study limits the ability to assess any differences in outcome between males and females. As such, future studies will need to have a larger sample size to ensure these data can be captured.
Conclusion
This retrospective study documents the results of a quality assurance review of the treatment of ASD at SSV ski resort. A success rate of 89% supports the idea that nonmedical ski patrollers can successfully perform ASD reductions. We believe training ski patrollers to reduce ASD improved patient care in our austere environment by providing early definitive treatment with high success rates. Overall, more research is still needed to better document: 1) the actual time saved between initial injury and reduction when performing prehospital reductions, 2) complications of prehospital reductions, and 3) the patient experience of ski hill shoulder reductions compared to traditional hospital management.
Footnotes
Acknowledgements
Acknowledgments: We thank Sunshine Village ski resort, Covenant Health library services (Edmonton, Alberta), Bree Roberts, the SSV ski patrollers, and medical volunteers. Finally, we acknowledge Andrew Walker, who was instrumental in our data analysis.
Author Contributions: Study concept and design, analysis of the data (JM); drafting of the manuscript (JM, KP); acquisition of the data, critical revisions of the manuscript, approval of the final manuscript (JM, IC, KP).
Financial/Material Support: None.
Disclosures: None.