
Abstract
The impact and severity of natural disasters and hazards have been increasing in the United States and throughout the world. With our mounting reliance and dependence on technology in our industrialized society, technological disasters also have become more commonplace. Although disasters may occur with little to no warning, these risks are felt to be acceptable despite their ability to impact large populations. Natural and technological disasters disproportionately affect vulnerable populations, including those with end-stage kidney disease (ESKD). The impact of natural and technological disasters on the ESKD community has been closely examined via numerous case studies and through the lens of particular disasters, but there is a paucity of data exploring the impacts of natural and technological disasters on the ESKD community by disaster type. A comprehensive literature search was performed using PubMed and Google Scholar, and relevant articles pertaining to the impacts of natural and technological disasters on the ESKD community were reviewed. More than 50 studies were reviewed in total. This review aimed to identify common patterns and trends observed in the impacts of different disaster types on the ESKD community to better prepare patients and their providers before the next disaster strikes.
Keywords
Introduction
Human populations are increasingly at risk from natural hazards such as flooding, hurricanes, tornadoes, thunderstorms, drought conditions, and wildfires, which are increasing in frequency, severity, or both due to global climate change.1,2 At the same time, human factors such as population growth and urbanization have increased losses due to higher degrees of exposure to these events. 3 The implications for human health are many, including degradation of air quality due to increased surface-level ozone levels in urban heat islands, increased incidence of vector-borne illnesses due to stagnant water, destruction of infrastructure leading to reduced sanitation and impaired water purification, and reduced access to care due to impacts on medical infrastructure and transportation. 1
Natural and technological disasters have not affected all populations equally. Some individuals are more likely to experience injury, death, or property loss from disasters due to their socioeconomic or other situational factors. 3 Considered socially vulnerable, these individuals may belong to special-needs populations, including those with limited access to transportation, people with disabilities, older adults, and people with limited English proficiency. 2 In some areas, vulnerability due to increasing exposure is exacerbated by social vulnerability. For example, Strader et al 4 examined exposure and social vulnerability characteristics of various different county warning areas throughout the United States and found that such areas in the southeastern United States, a region that also is more socially vulnerable,were disproportionately affected by severe weather compared with other regions as measured by social vulnerability index.
Similarly, disasters have not had the same effects on human health for all social groups. 5 Individuals with disabilities, which would include those with medical conditions that require constant or frequent use of life-support systems, may experience difficulties in responding to disasters. 6 The disparate effects of disasters on the health outcomes of our most vulnerable populations have demanded the attention of medical professionals, population health policy experts, and environmental health specialists worldwide.
One population that has a high risk of negative health impacts resulting from natural and technological disasters includes those with end-stage kidney disease (ESKD) requiring dialysis treatment. This community is particularly vulnerable due to its dependence on physical infrastructure and utilities such as clean water, electricity, and other resources to provide life-sustaining therapy. Hemodialysis patients require regularly scheduled treatments that use a machine to remove toxins as well as maintain safe levels of minerals in their bloodstream, a physiologic function that is typically provided by the kidneys, which continuously filter blood and manage fluid balance. Hemodialysis typically occurs in a healthcare facility. Given the critical need for this regular treatment, disasters place dialysis patients at particular risk for morbidity and mortality if the treatment is delayed or stopped due to logistical and infrastructure problems that may ensue following a disaster. 7 Peritoneal dialysis differs from hemodialysis in that patients undergo treatment by using the peritoneal membrane in their abdomen to cleanse the blood of toxins via an indwelling catheter in the abdomen rather than by removing and filtering the blood directly through a dialysis machine. It also takes place at home. A retrospective study conducted by Blum et al 8 found that dialysis patients living in hurricane-exposed counties (including both those who received dialysis at a center and all at-home modalities) were at higher risk of mortality in the subsequent 30 days following the hurricane compared with unexposed patients after adjusting for demographic and socioeconomic covariate data.
Given the susceptibility of these patients to the secondary impacts of environmental hazards and disasters, the field of disaster nephrology has been gaining attention in the nephrology community at large. Numerous case studies have been published documenting both the acute hazards of renal failure that may result directly from particular disasters and the lasting effects of the disasters on delivery of care to patients with ESKD. 9 Much of the existing literature has focused on emergency preparedness. The most commonly prepared-for event is a disaster that leads to an increase in the need for dialytic therapies due to increased incidence of acute kidney injury (AKI) resulting from the disaster, but another important event is one that leads to a degradation of existing resources for those with preexisting ESKD. 10 Another underrecognized adverse health outcome that may negatively impact dialysis patients following a disaster are the deleterious effects on their mental and emotional health. McClellan 11 emphasizes the importance of social workers and mental health counselors to mitigate the emotional trauma that dialysis patients may experience following disasters because this population may be especially vulnerable given their preexisting disease and the need for ongoing dialytic care.
Disasters often can have far-ranging consequences that are not limited to adverse health outcomes. Impacts to dialytic services in disaster-struck areas often can last many years due to the effects on medical infrastructure and healthcare systems and the effects on their nephrologists and other care providers. Individual patients may need to relocate rapidly, requiring abrupt adjustments to their own care while possibly creating a void in demand in the communities they leave. For example, a study by Kleinpeter 12 noted a dramatic decrease in the number of dialysis patients residing in the most affected hurricane-designated parishes in Louisiana following hurricanes Katrina and Rita in 2005. The effects of the hurricanes were found not to be limited to dialysis patients. Permanent relocation of physicians and other healthcare professionals also was observed following the hurricanes due to damage or loss of personal property and damage to their place of employment. Because the timeliness of credentialing practices in hospitals often may impair the ability of providers to practice in other hurricane-affected communities immediately after disasters, the subsequent migration of healthcare professionals can further hinder access to care for dialysis patients. It is necessary to adapt to the changing environment to prevent the reallocation of vital medical resources to this particularly vulnerable population.
Although much of the medical literature focuses either on the broader impacts of disasters on health outcomes of patients with ESKD or on the specific impacts of individual disasters on a select population, there are few studies that specifically examine the effects of disasters on patients with ESKD by disaster type. Thus, we have attempted to fill this gap in knowledge. By reviewing the impacts of disaster type on the ESKD community, we found both commonalities that cut across hazard type and valuable distinctions that exist among the hazards. We also identified hazards about which peer-reviewed literature was lacking. We discuss below how these different events affect ESKD patients in both unique and similar ways.
Classification of Events by Hazard Type
Hazard events are often classified by the rate of the onset of their physical manifestation and distinguished as rapid-onset events, which provide very little time for preparation, or slow-onset events, which have extended lead times or are pervasive but appear to have no fixed beginning or end 13 (Figure 1). Examples of rapid-onset events include tornadoes, flashfloods, and earthquakes. River floods, winter storms, and hurricanes are slower-onset events, whereas climate change and heat or cold waves are examples of events that can be prepared for but may start to have impacts without a clear onset. These are sometimes referred to as pervasive hazards. Other human-caused disasters such as war also fall into this category. For this review, the key distinction is the ability to prepare or respond prior to impact, both by patients and by the medical community.
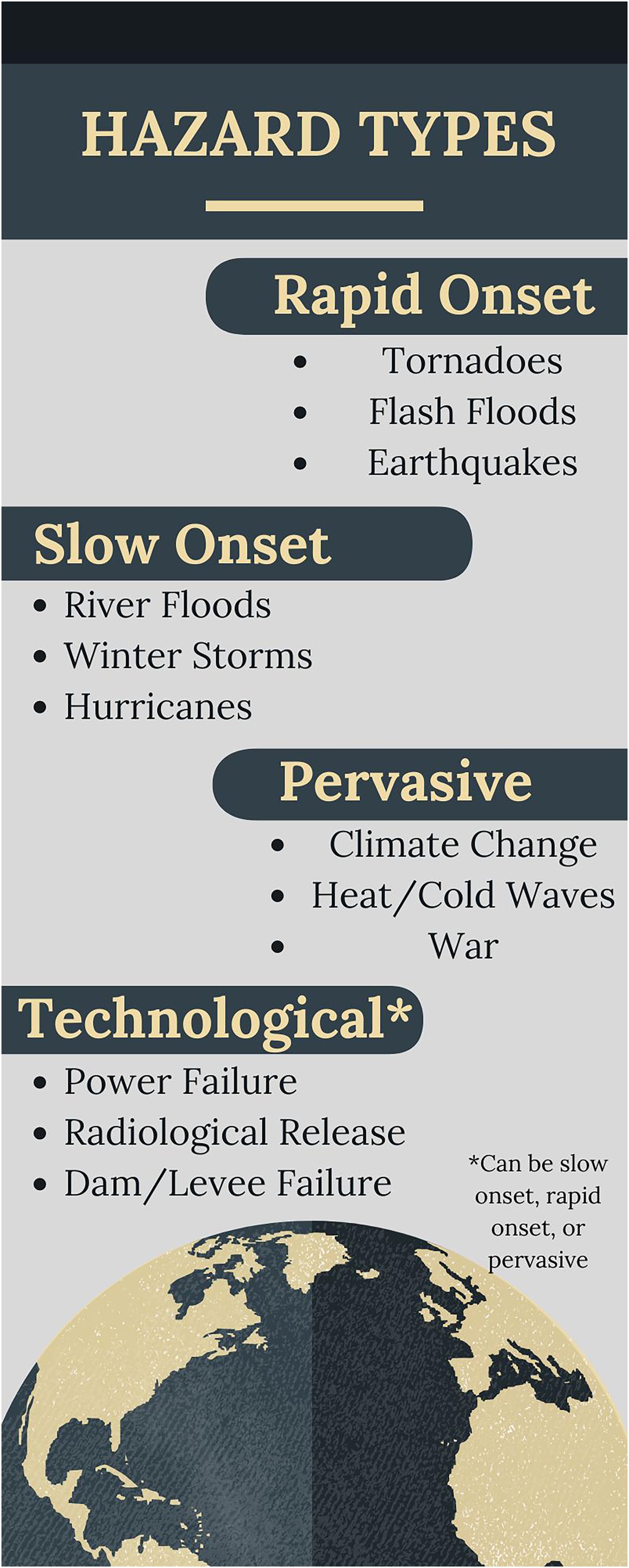
Classification of hazard types.
Rapid Onset Events
Impacts
Rapid-onset events leave little or no time to prepare, and therefore, the focus of most studies is on the aftermath of the disaster. Of rapid-onset events, the type of disaster that has been most closely examined in its impacts on patients with ESKD is earthquakes. Numerous studies have been published in the literature describing the profound impacts that earthquakes may have on patients with kidney disease.

Mitigating the impacts of disasters on the end-stage kidney disease community.
Earthquakes can lead to structural failures that can both impact patients with preexisting kidney disease and lead to traumatic crush injuries such as rhabdomyolysis, which can cause muscle ischemia and kidney injury. Both increases in acute kidney injury requiring hemodialysis and reduced access to dialytic therapies due to impacts on preexisting medical infrastructure can lead to a strain on available dialysis resources for a particular community. 14 Ikegaya et al 14 observed that following a series of earthquakes that struck the Kumamoto Prefecture in Japan's Kyusu region in April 2016, a significant proportion of the region's dialysis facilities could not continue services.
Hemodialysis patients are not the only dialysis patients that are affected by earthquakes. Although less dependent on certain resources and utilities, continuous ambulatory peritoneal dialysis patients often face different challenges due to structural and supply losses that may ensue following an earthquake. Sakai 15 found that after the Kobe earthquake in 1995, many continuous ambulatory peritoneal dialysis patients had increased flexibility and less dependency on standing hospitals given the lack of need for in-center support with their treatment and the reliability of their supplier that proved advantageous and effective in a contingency.
Another key factor in the occurrence of AKI and access to medical care following an earthquake is the nature of the built environment and rurality of the disaster-affected region. Van der Tol et al 16 compared outcome data of 88 crush-related AKI patients in the Kashmir earthquake of 2005 and 596 crush-related AKI patients in the Marmara earthquake of 1999 to determine risk factors for morbidity, such as incidence of kidney failure and mortality, to assist with future disaster planning. The authors found that the cumulative risk of AKI was higher in Marmara, likely given its urban environment, higher population, and structural density, whereas the time lag between earthquake and admission to the hospital were longer in the more rural Kashmir.
Earthquakes also can impact individual patient-related health factors given the acute stress of the events, leading to worse long-term health outcomes such as high blood pressure or disaster hypertension, resulting in chronic kidney disease (CKD) and earlier onset of hemodialysis. Abe et al 17 conducted a single-center retrospective observational study to compare the number and age of patients initiated on hemodialysis both before and after the Great East Japan Earthquake in 2011 and found that the number of patients initiated on chronic hemodialysis after the earthquake due to hypertensive causes increased over the successive 10 years after the event. The authors suggest that the second-order effects of increased stress, low income, and a sense of loss may lead to sympathetic nervous system activation resulting in hypertension, which, in conjunction with malnutrition and increased sodium intake, may be responsible for the increased rates of ESKD.
The Fukushima Daiichi nuclear power plant accident is an example of a technological disaster caused by a natural event, sometimes referred to as “natech” by disaster scholars. Although there remains a paucity of published reports on the impacts of technological disasters on the ESKD community, it has been one of the better-studied accidents given its recency, size, and scope and the interest surrounding Fukushima. Unlike many disasters in which residents return to the area in hours to days after the threat has passed, residents may be significantly or even permanently delayed from reentering their homes following a nuclear accident. 18 Nishikawa et al 19 described the long-term impact of the earthquake, tsunami, and subsequent nuclear disaster on a 66-year-old male hemodialysis patient who was forced to evacuate and relocate multiple times to receive his life-sustaining therapy. Although he was able to return to his home a year later, he found that the hemodialysis units had been relocated, and he continued to have difficulty with hemodialysis access even years after the event, demonstrating the persistent effects that technological disasters can have on access to care for rural populations. Similarly, Shimmura et al 20 conducted a study of hemodialysis patients residing near the Fukushima Daiichi nuclear power plant to determine the internal radioactive contamination levels using a whole-body counter to detect Cs-137 levels. They found that among the 111 patients they tested, only two had measurable levels above the threshold of detection, suggesting negligible doses of radioactive contamination in all patients.
Tornadoes provide a limited amount of lead time (on average 13 min) and require awareness that the individual affected is under a warning. 21 Very little has been published about the impact of tornadoes on ESKD. This literature may be limited to the impact of one tornado on one dialysis patient. During the 1999 Oklahoma City tornado, a dialysis patient older than 65 years of age died after being found to be connected to a renal dialysis machine during the warning timeline. 22 It was not clear whether the victim had received the warning. People who are elderly, often due to limited mobility, may be less likely to heed tornado warnings.22
Mitigation
One common mitigation strategy is the use of adaptive measures such as reductions in time or frequency or other alterations in dialytic prescriptions to allow for treatment of the maximum number of patients in the setting of limited resources. Haga et al 23 studied the effects of shortening the duration of hemodialysis treatment sessions on laboratory findings of hemodialysis patients following the Great East Japan Earthquake in 2011. This study was undertaken after hospitals located within an 80-km radius of the Fukushima Daiichi nuclear power plant were evacuated. The investigators found that laboratory and clinical findings such as blood urea nitrogen concentrations, hematocrit, and cardiothoracic ratio of chronic hemodialysis patients were not significantly worsened despite the adjustment in the length of their hemodialysis treatments.
The existence of organizational support through the Renal Disaster Relief Task Force of the International Society of Nephrology and Médecins Sans Frontières also have proved invaluable in providing aid to patients with or at risk for kidney disease following earthquakes. Vanholder et al 24 found that the presence of nephrology disaster humanitarian support in the Marmara earthquake in Turkey in 1999 was critical to ensuring strong logistical support, prompt identification of needs, and distribution of resources. The importance of nephrology disaster humanitarian support was confirmed by the experience of the Renal Disaster Relief Task Force of the International Society of Nephrology and Médecins Sans Frontières in both the 2010 Haitian earthquake and the 2010 Chilean earthquake as well despite very different impacts to the population. 25
The importance of well-organized disaster mitigation plans cannot be understated, and such plans can lead to improved outcomes for all patients despite the unpredictable nature of earthquakes. Vanholder et al 26 found that quick responses in the extrication of patients from the rubble following the L’Aquila earthquake in Italy in 2009 saved lives and served as an example of how disaster planning is critical for mitigating morbidity following an earthquake. In addition to the fast extrication of crush victims by first responders, Italian disaster plans included detailed instructions on the management of crush injuries and other nephrologic issues, leading to improved outcomes for patients with AKI. The authors found that due to the well-orchestrated response by the Italian authorities, the ratio of dialyzed patients to deaths far exceeded that of both the Marmara and Kobe earthquakes.
The lessons learned from these prior earthquakes have informed planning preparation in lesser affected parts of the world, such as South Korea. Yoo et al 27 published a review that investigated the responses to earthquakes in neighboring Japan, such as the Kobe and Great East Japan earthquakes, and urged the development of disaster kits and emergency procedures to be undertaken by dialysis patients and staff during disasters following the Gyeongju and Pohang earthquakes in Korea in 2019.
Prior to the 2011 tornado in Joplin, Missouri, health officials activated an existing plan in which providers instructed dialysis patients to create and then implement a 3-day emergency plan. 28 With these prior experiences and lessons learned, the ESKD community and their providers will be better equipped and prepared for the next earthquake that will strike.
Slow Onset Events
River flooding, coastal hazards, and hurricanes typically provide longer lead times between the forecast or warning and the impacts. Although much of the literature on the impacts of earthquakes has highlighted the increased demand for acute dialysis due to crush injuries and the reduced access to dialysis for chronic dialysis patients due to loss of medical infrastructure, the displacement of dialysis patients from their communities and reduced access to care are a recurring theme in hurricane disasters.
Impacts
The impact of Hurricanes Irma and Maria in 2017 on the US Virgin Islands highlights all these themes. Due to widespread damage to the medical infrastructure and transportation systems in the US Virgin Islands following landfall of Hurricane Irma, the damage sustained to the limited dialysis resources required most dialysis patients to be evacuated to Puerto Rico for treatment. 29 Following the evacuation, many of the patients received fragmented care due to the lack of a universal health system, with many such patients having complications due to shortened/missed treatments or vascular access issues, illustrating a need for improved advanced disaster preparedness.
Despite the established importance of advanced disaster planning, patients with ESKD still lack sufficient knowledge regarding disaster preparedness and awareness. A cross-sectional survey study conducted by Murakami et al 30 before and after the landfall of Hurricane Sandy in Manhattan, New York, found that while individual dialysis-specific disaster preparedness was associated with fewer missed dialysis sessions, there was a need to improve dialysis preparedness for dialysis patients overall. Further planning for such events that could produce power outages should include a variety of options for patients and centers to include coordination with alternative centers for dialysis sessions, on-site backup generators, or delivery of generators to providers to ensure uninterrupted care. 31
Additionally, ESKD patients are also at added risk from disasters such as hurricanes because these patients are typically more socially disadvantaged, have fewer financial resources, and may be more likely to live in disaster-prone areas than those without kidney disease. 32 Moreover, Anderson et al 33 conducted a telephone survey of ESKD patients following Hurricane Katrina in 2005 and found that individuals who lived at home alone, frequently missed dialysis sessions prior to the storm, had initiated dialysis less than 2 y prior to the event, waited to evacuate until the day of the storm, or were unaware of their dialysis unit's emergency plan were more likely to miss 3 or more dialysis sessions in the immediate aftermath of the storm. The authors conclude that added emphasis on disaster preparedness for dialysis patients may be of potential benefit.
There are very few studies that examine winter storm impacts. As with other disaster types, ice storms may be associated with significant power outages. Winter Storm Uri in Texas in 2021 caused widespread power outages and frozen water pipes that led to closure of many outpatient dialysis units, causing patients to miss appointments. 34 There is also a noted increase in hospital admissions for CKD patients, with a drop of 8°C associated with an increased relative risk of admission. 35
Mitigation
Some of the effects of displacement from hurricane disasters can be mitigated successfully by advanced disaster planning on the part of ESKD patients and their providers. Lukowsky et al 36 found that by using comprehensive disaster plans, Manhattan Veterans Affairs Medical Center dialysis patients were able to use alternate VA and non-VA sites to continue their treatment despite months long closure of the Manhattan Veterans Affairs Medical Center dialysis unit following Superstorm Sandy. Early dialysis also has been used routinely to mitigate the risks of delayed or missed dialysis as a result of an impending disaster. Given the lead time associated with many hurricanes and the advances in hurricane forecasting, early dialysis has been used with success in reducing complications and improving patient outcomes for ESKD patients in hurricane-affected regions. A retrospective cohort study by Lurie et al 37 found that ESKD patients in New York and New Jersey who received early dialysis prior to Hurricane Sandy had significantly lower odds of having an emergency department visit and hospitalization in the week of the storm or of dying within 30 days of the storm.
The impact of Hurricane Katrina on the Gulf Coast resulted in delays and disruption to dialytic services in the region for months to years. Kleinpeter 38 found that following Hurricane Katrina, half of all peritoneal dialysis patients returned to the Gulf Coast, whereas only 25% of hemodialysis patients returned within 6 months. She suggests that rather than rebuilding dialysis units in hurricane-prone regions and hemodialysis patients continuing to reside in those regions, use of peritoneal dialysis and referral for transplantation should be prioritized because they may offer advantages over hemodialysis. Just as Sakai 15 observed with the experience of his peritoneal dialysis patients following the Kobe earthquake in 1995, peritoneal dialysis as a modality for improved hurricane preparedness necessitates consideration (Figure 2).
Pervasive Hazards
Finally, human conflict and war pose significant risks to the ESKD community by producing additional burdens for patients seeking medical care and placing resource constraints on already depleted medical personnel and supplies. Novakivskyy et al 39 described the challenges of providing dialytic support for the ESKD community in the midst of war in Ukraine. In addition to disruptions in utilities such as water and electricity through shelling and human-made damage to infrastructure leading to delayed treatment, providing consistent shelter, medical care, and food to patients also was a challenge that providers faced in Ukraine during the war.
Increases in global population density and the subsequent increase in greenhouse gas emissions such as carbon dioxide have led to climate change.40,41 The World Health Organization in 2023 attributed 24% of deaths to risks in the environment, including climate change, and the Centers for Disease Control and Prevention even created a framework for which health departments can anticipate, prepare for, and deal with climate change.42,43
Given the risk of extracellular volume depletion and subsequent decrements in renal function, patients with CKD are at particular risk when exposed to hot weather. Analysis of hospital admissions in Cook County, Illinois, during the heat wave of 1995 showed statistically significant increases in admission for renal dysfunction, including a more than 300% increase in acute renal failure. 44 Furthermore, analysis of heat impacts on emergency renal admissions in Texas, known for both high ethnic diversity and high temperatures, showed that a 1°C increase in temperature was associated with an overall 1.73% increase in hospital admission for all types of kidney disease, with the largest effect on those 18 to 65 years of age. 45 A similar effect on this age group was noted during heat waves in Adelaide, Australia, where a 10% increase in renal admissions was seen. 46 Additionally, a trend toward a greater effect of heat on morbidity and mortality in African American and Hispanic populations also was observed, which was more prominent in ESKD patients with coexisting congestive heart failure, chronic obstructive pulmonary disease, or diabetes.45,47
Over the past few years, the predominance of data linking hot weather with adverse renal outcomes has led to growing concern in the medical community about the risk of heat on patients with CKD. A meta-analysis in 2021 of 82 studies addressing adverse outcomes in CKD patients with heat exposure noted increased kidney-related morbidity and mortality associated with hot weather, with a 1°C increase in temperature being associated with a 1% increase in kidney-related morbidity and a 3% increase in kidney-related mortality. 48
Conclusion
Disease burden from CKD continues to be on the rise, with deaths from chronic kidney disease having doubled from 1990 to 2016. 49 A combination of the strength or intensity of a hazard event and the characteristics of the population affected determine the level of impact. Although the actual impact of an event varies based on the social and physical characteristics of the location affected, stronger events are likely to produce more significant impacts to health infrastructure and health outcomes. Additionally, kidney disease tends to disproportionately affect racial minority groups such as African American and Hispanic individuals, which may further exacerbate health disparities following disasters. 50 Events also can be distinguished by the amount of lead time patients and the medical community have to prepare. There are also differing impacts on populations, with lower socioeconomic and marginalized populations more likely to be negatively affected. Countries in the developing world with lower socioeconomic status and worse access to medical care have a higher CKD burden and tend to be the same countries that experience the highest mortality burden from most disasters.
Having discussed these risks posed by natural and technological disasters to the ESKD community, efforts are being made to better plan and be prepared for the next one, whenever that may be. Following the catastrophic 2005 hurricane season, the US-based Kidney Community Emergency Response Coalition was formed from 50 different government organizations and agencies to minimize disruption to dialysis and transplant services and to help develop response guidelines for dialysis patients, units, and providers. 51 As a result of these efforts, numerous informational resources have been produced, including the Centers for Medicare and Medicaid Services’ “Emergency preparedness concepts for dialysis facilities,” 52 which describes detailed strategies for hazard mitigation for a variety of different hazards. Additionally, the aftermath of Hurricane Katrina and its impact across multiple state borders highlighted the need for fundamental changes in disaster management within the United States given the complexity of the disaster response and the need to coordinate efforts across diverse agencies and personnel. 53 The subsequent restructuring that occurred as part of the National Response Framework in 2008 has emphasized the importance of locally led coordination of emergency resources, empowering local authorities and agencies to assist and provide support where need is the highest. 54
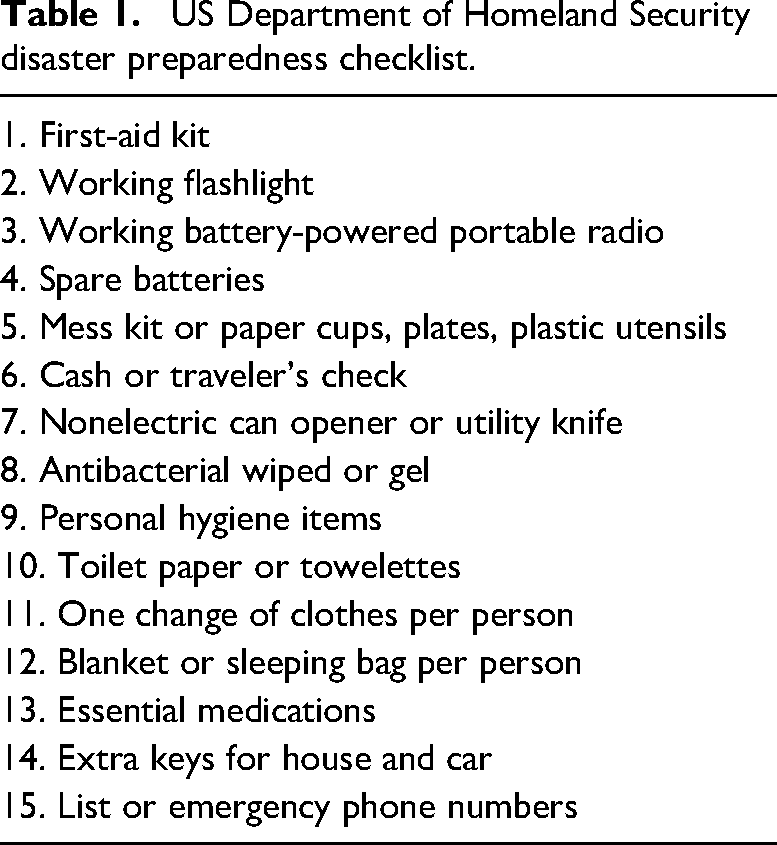
Despite the best efforts of the dialysis community to implement these hazard-mitigation strategies and develop guidelines for disaster emergency preparedness, the reality is that many dialysis patients remain woefully unprepared for the next disaster. Several studies have shown that peritoneal dialysis patients appear to be better prepared and more self-sufficient than hemodialysis patients, but the use of peritoneal dialysis as a treatment alternative for individuals living in disaster-prone regions remains underexplored. A prevalence study of 311 dialysis patients that surveyed general disaster preparedness based on US Department of Homeland Security recommendations found that irrespective of sociodemographic characteristics, most patients were unprepared for a disaster. 55 Although just over half had ample food and water, fewer than half had most of the US Department of Homeland Security checklist items (Table 1). Specific to dialysis preparedness, fewer than half knew of alternate dialysis centers, had sufficient medical information to provide for treatment, or had a wearable identifier to alert healthcare providers about their condition. The results of the survey led to efforts being made to improve awareness of dialysis patients’ needs, including the creation of the emPOWER Program by the US Department of Human and Health Services to identify patients requiring electricity-dependent medical equipment.56,57
Fortunately, progress in disaster preparedness for the ESKD community is being made. Receipt of early dialysis, a commonly used strategy that has been employed as a protective measure in advance of a natural disaster, was as high as 60% in ESKD patients prior to Hurricane Sandy in 2012, suggesting that efforts to educate patients on the importance of this intervention have been successful. 58 Efforts to improve patient education on the need for disaster preparedness likely will continue to prove beneficial in improving outcomes in patients with ESKD who are at risk from natural and technological disasters.
Although disasters each have different characteristics, many of these hazards pose similar risks to patients with ESKD. As unpredictable as many of these hazards may be, we must remain vigilant in how we prepare and systematically plan our responses should the time come when disaster strikes. We have a duty to protect our most vulnerable populations. The time is now.
US Department of Homeland Security disaster preparedness checklist.
Footnotes
Acknowledgments
The views expressed are those of the authors and do not reflect the official views of the United States Air Force, nor the Department of Defense. Mention of trade names, commercial products, organizations do not imply endorsement by the U.S. Government.
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.