
Abstract
Dr William J. Mills Jr., an Alaskan orthopedic surgeon, helped establish the current protocols for frostbite treatment and changed a dogma used for more than 140 years that was established by Napoleon's surgeon general of the army, Baron Dominique-Jean Larrey. During Napoleon's 1812 siege of Moscow, Larrey noticed the destructive effects of using open fire heat for warming frozen body parts, so he suggested rubbing snow or immersion in cold water. Dr Mills treated many cold injuries during his medical career. After setting up his medical practice in Anchorage, Alaska, he realized the inefficiency of the established protocols and started researching new treatments for frostbite. Dr Mills followed Meryman's method of rapidly thawing frozen red blood cells in warm water. Mills and his colleagues established a treatment protocol for freezing cold injury that included rapid warming in warm water. These studies resulted in the publication of three key papers in 1960 and 1961. These papers were the first clinical studies that described rapid warming as a treatment. Subsequently, rapid warming, with some variation in water temperatures, has been accepted as the standard of treatment. Due to his outstanding contribution to the treatment of frostbite, he has been referred to as “the nation's leading authority on cold injury.” Mills and his colleagues created a new classification system that divided frostbite into two levels, superficial and deep, which was more applicable in clinics than the traditional 4-tier classification. The 2-tier classification is still useful outside of the hospital setting.
Introduction
This journal recently published the Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Frostbite: 2024 Update. 1 Although the guidelines are designed to be as current as possible, it is important to note how much of the content emanates from work started in the late 1950s by Dr William J. Mills (1918–2011). This contribution to Lessons From History documents his influence, both in changing a century-old dogma and establishing treatment principles that still apply today.
Frostbite has long plagued participants in military, commercial, and recreational activities in cold environments. One of the turning points in the history of treating frostbite came during Napoleon's retreat from Russia in the early winter of 1812. Napoleon's surgeon general of the army, Baron Dominique-Jean Larrey, observed thousands of frostbite cases 2 and described the disastrous effects of using a campfire for warming the frozen part: “Those who approached the fires sufficiently near to warm frozen feet and hands were attacked by gangrene in all points.” 3
Thus, Larrey suggested that “instead of submitting it [the frozen part] to heat, which provokes gangrene, it is necessary to rub the affected part with a substance containing very little caloric, but which may absorb a good deal at the moment of their melting and transmit it to the frozen part by rubbing” and then, “should these remedies fail (eg, rubbing the affected part with snow), the part ought to be plunged in cold water.” Due to the authority of his position, this became the standard treatment for frostbite for almost a century and a half. 4 Indeed, during both world wars, rubbing tissue with snow or immersion in a cold bath were the universally recommended treatments for frostbite.
Dr William Mills was one of the main characters in redirecting the treatment of frostbite to warming the tissue rather than cooling it. Dr Mills (Figure 1) was cited as “the nation's leading authority on cold injury” at the Mountain Medicine Lecture Series at the University of California in the 1980s. 5 Born in San Francisco, he left home to attend the University of California at Berkeley, where he said he “majored in Anthropology, Zoology, and Poverty.” 6 He then enlisted in the Navy as an apprentice seaman when Pearl Harbor was attacked. He served as the commander of PT 181 in the U.S. Navy during World War II from 1942–1945. Mills sustained two open fractures in both his lower legs during the Solomon Islands Campaign. Due to the hard conditions on Kolombangara Island at the time, there was no access to proper health care, and one of his legs was amputated because of gangrene. 6 He received his medical degree in 1950 from Stanford University and then completed a residency in orthopedic surgery at the University of Michigan.
Dr William J Mills Jr.
In 1955, he started an orthopedic practice in Anchorage, Alaska, and the following year, he was voted Alaskan Physician of the Year. He was a founding member of the Alaska State Medical Association and first editor in chief of the journal Alaska Medicine. Dr Mills continued his military service by serving in the Naval Medical Corps Reserve from 1956–1978 and retired as a rear admiral. He also served as chief of orthopedic surgery for the III Marine Amphibious Force in Vietnam from 1966–1967. 5 Mills had an active role in writing the State of Alaska Cold Injury Guidelines through numerous revisions from 1982 to 2005, which was the last version in which he participated. 6 Throughout his 40+ year career, Dr Mills continued to advance understanding and treatment of frostbite, and on his retirement, left a number of suggestions for future research.
To facilitate this project, a Medline search was conducted for all publications by William J. Mills. Eighty-five papers were located and exported to the Rayyan QCRI program. Two reviewers independently screened these articles, and 25 were included based on the inclusion criteria (eg, frostbite pathophysiology, characteristics, and treatment). These selections consisted mostly of research and summary papers but also included a technical report and a textbook chapter.
Historical Perspective on the Treatment of Frostbite
In the 1930s, Russian Professor T. J. Ariev challenged Larrey's slow-warming method for frostbite. He and his colleagues warmed frozen rabbit ears and extremities and demonstrated that rapid warming in 30–35°C water produced a significant decrease in the zone of necrosis in comparison to slow warming. Western physicians were not aware of this work until the results were translated into English by Dr Iser Steiman of the Canadian Department of Defense during World War II. 7
Harold T. Meryman, a US Navy medical officer, “became one of the world's leading investigators in cold-related science and cryobiology” in the mid-1950s. 8 His work on cryopreservation of living blood cells provided evidence for rapid rewarming from frostbite. He developed a precise explanation of the effect of the rate of freezing and thawing on cellular damage. 8 Meryman reasoned that as extracellular tissue freezes, ice crystals form and grow. The longer the freezing process takes (eg, the slower the rate), the more water is removed from the cells, resulting in larger ice crystals (causing more physical damage) and higher concentrations of electrolytes and enzymes within the cell (causing chemical damage). 9 As a result, Meryman concluded that rapid freezing and thawing is the best solution for cryopreservation. 10 This logic led Mills to conclude that rapid thawing might also be best for minimizing tissue damage from frostbite.
In his clinical practice in Anchorage, Mills saw over a thousand frostbite cases. Although most cases came from urban patients (who were often unhoused or intoxicated), the lessons learned are readily applicable to recreational and wilderness scenarios.
Mills and his colleagues established a treatment protocol for freezing cold injury that included rapid warming of frozen tissues in warm water. These studies resulted in the publication of three key papers in 1960 and 1961, which are referenced later.11–13 These papers were the first clinical studies that described rapid warming as a preferred treatment. This recommended treatment is virtually unchanged in the current Wilderness Medical Society (WMS) guidelines. 1 These three papers were republished in a special issue of Alaska Medicine in 1993. 14 The remainder of that issue consisted of papers with Mills either as solo or coauthor and described further advances in frostbite treatment of the previous three decades.
Over the years, Mills and his colleagues compared the outcomes for frostbite patients who had one of four methods of thawing, which included rapid rewarming in 42–48°C water, slow spontaneous thawing in air at room temperature, delayed thawing with ice and snow, and thawing by excessive dry heat.
The first series of papers reported the results for 51 patients (see Table 1).11–13 The rate of amputation increased from rapid warming (14%) to slow thawing (40%), to delayed thawing (66%), to excessive heat thawing (only one individual was treated with excessive heat, and this individual received an amputation).11–13
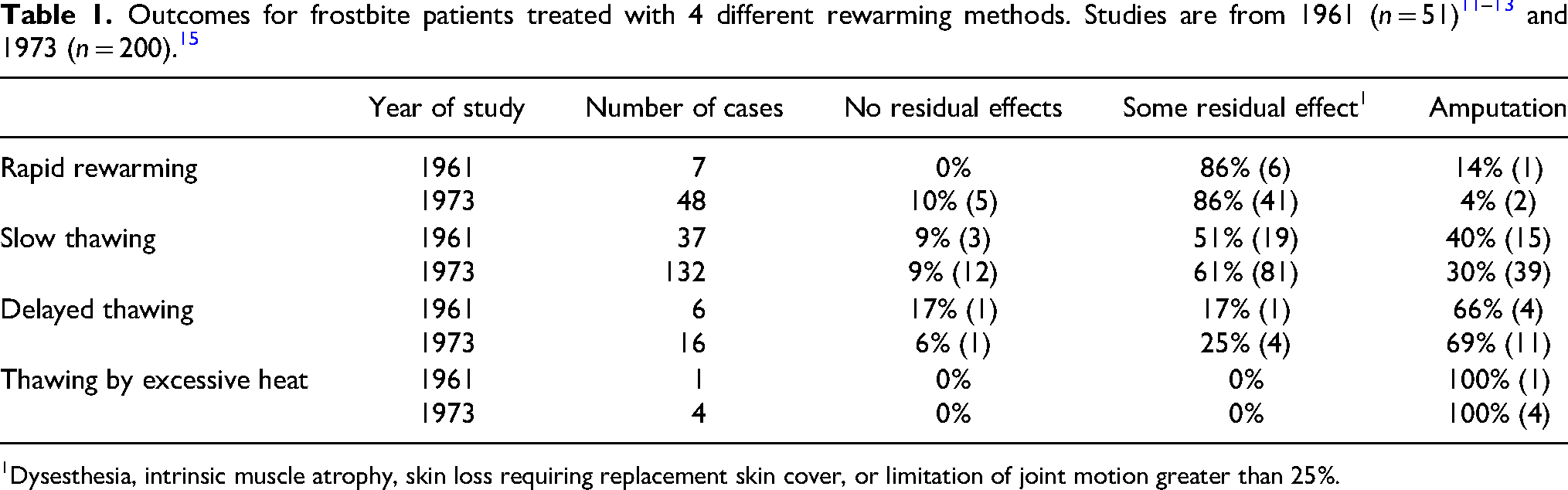
Dysesthesia, intrinsic muscle atrophy, skin loss requiring replacement skin cover, or limitation of joint motion greater than 25%.
The 1993 Alaska Medicine publications were well-known for the many clinical photographs of the injuries themselves as well as diagnostic assessments. For example, time sequences were shown for rapid and slow (spontaneous) thawing (Figure 2) and delayed (ice and snow) and excessive heat thawing (Figure 3).
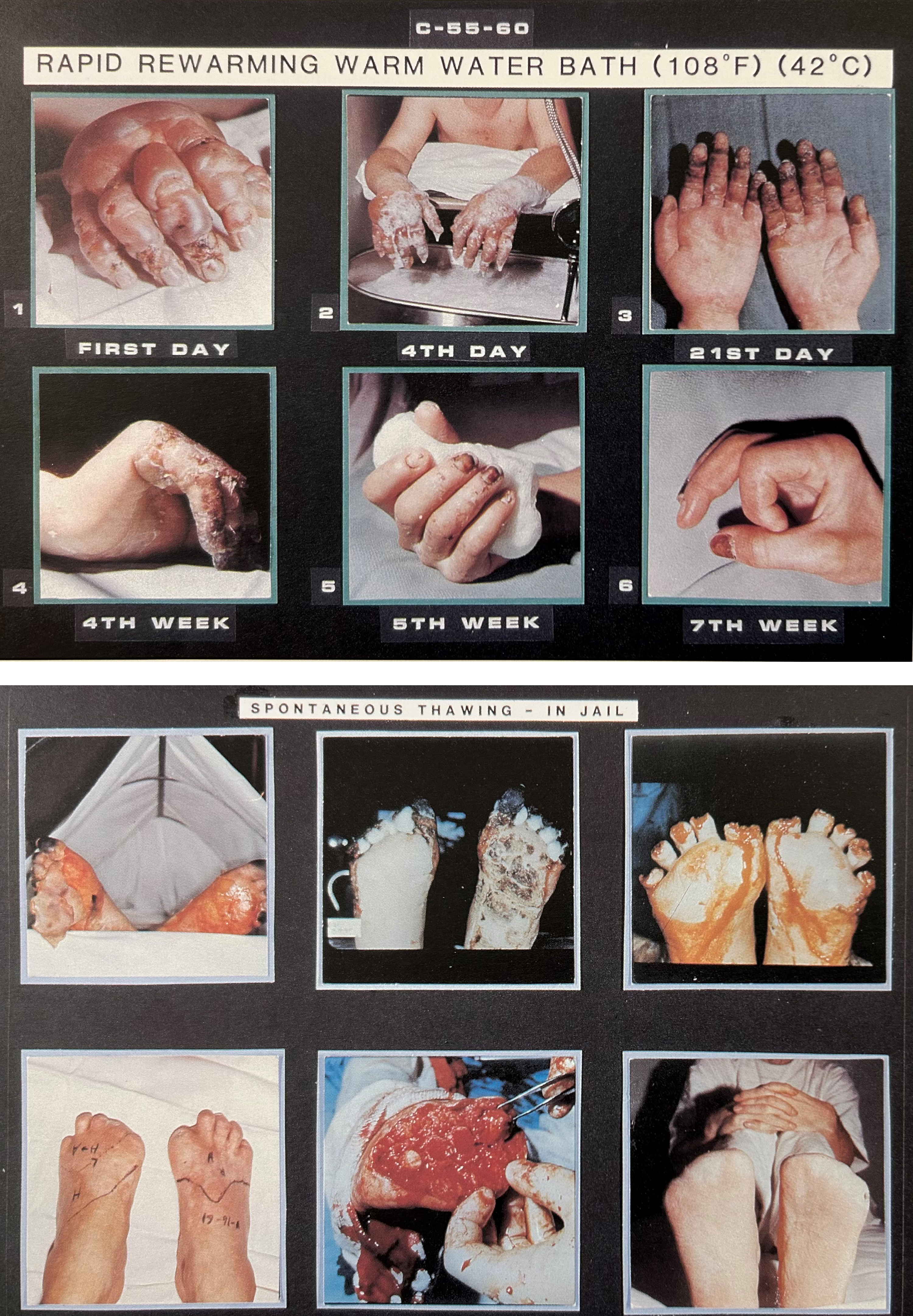
Time sequence photographs of frostbite patients undergoing rapid rewarming in warm 42°C water with full recovery (top), and slow spontaneous thawing in room air with all toes amputated (bottom).
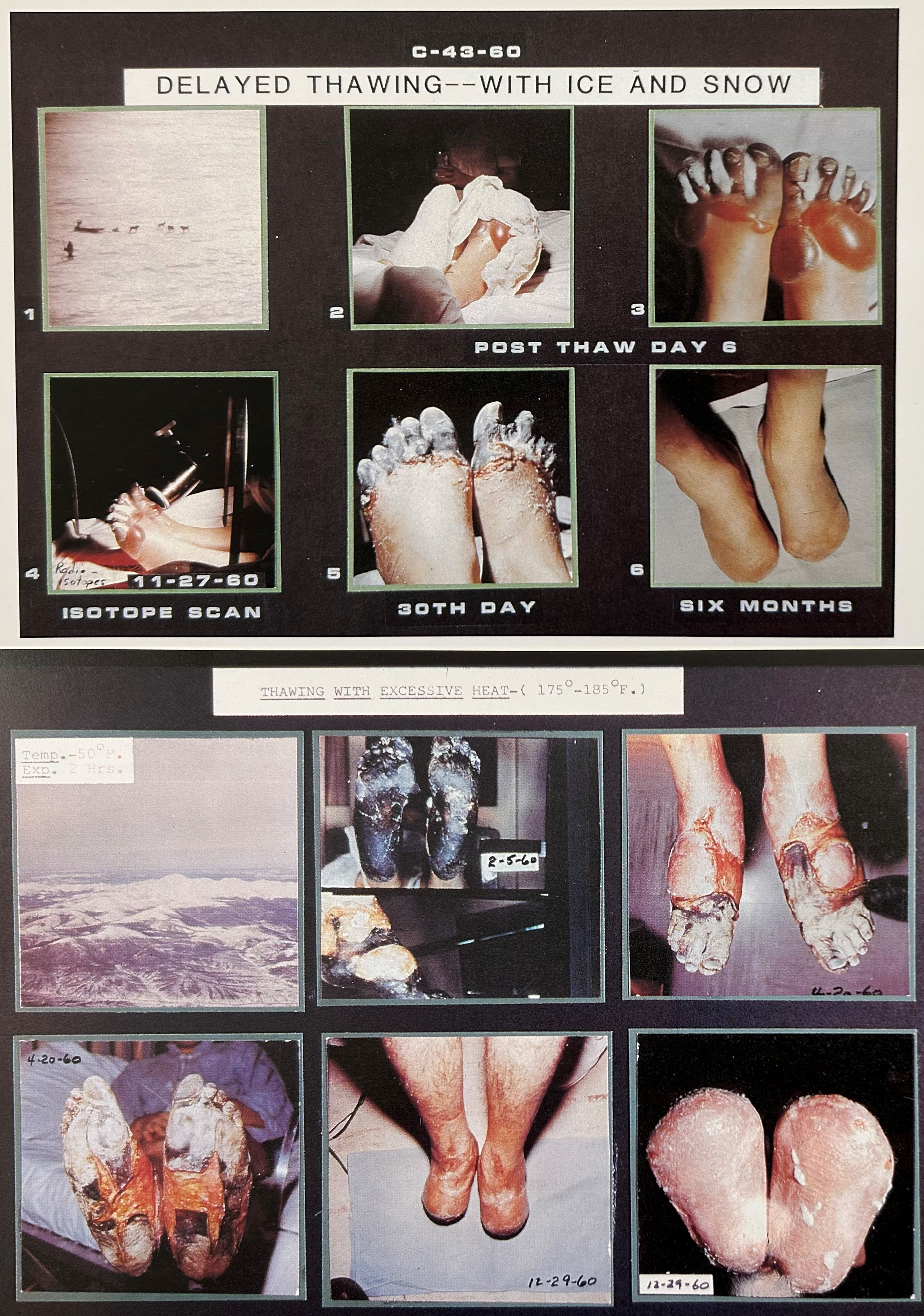
Time sequence photographs of frostbite patients undergoing delayed thawing by immersion in snow and ice water for 8 h, with all toes amputated (top), and thawing with excessive heat by exposing feet to diesel generator exhaust with air temperature 80-85°C, bilateral distal foot amputation (bottom).
Table 1 also includes results from 1973, during which time Dr Mills had accumulated details from 200 frostbite patients. 15 These results confirmed that rapid rewarming was the best method for thawing and that prognosis was poorer for slow thawing, delayed thawing, and excessive heat thawing, respectively. By 1993, Dr Mills had treated 1026 frostbite patients with rapid rewarming. He published a thorough explanation for the treatment of frostbite and affirmed the effectiveness of rapid rewarming in achieving greater tissue preservation. 16
Rapid rewarming was more painful than gradual rewarming in its initial stage; it caused more hyperemia and larger blebs. The pedal pulses often were “pounding” after warming, and the blebs usually extended to include even the terminal phalanges. Because of the extreme reaction, particularly the formation of edema and blebs, Mills stated this method may not be a “trail therapy” for use in the field.13,17
Rapid rewarming continued to be the fundamental part of the treatment of frostbite, with some alterations in water temperature. In their first paper, the water temperature was 42–48°C. 11 Then, they reduced the maximum recommended temperature to a range between 42–46°C. 17 Mills continued to decrease the recommended water temperature in subsequent years. A final water temperature ranging from 38–41°C was recommended in 1983. 18 This remained the recommended temperature range in his following papers.16,19 Little has changed as the WMS currently recommends rapid warming in water ranging from 37–39°C. 1
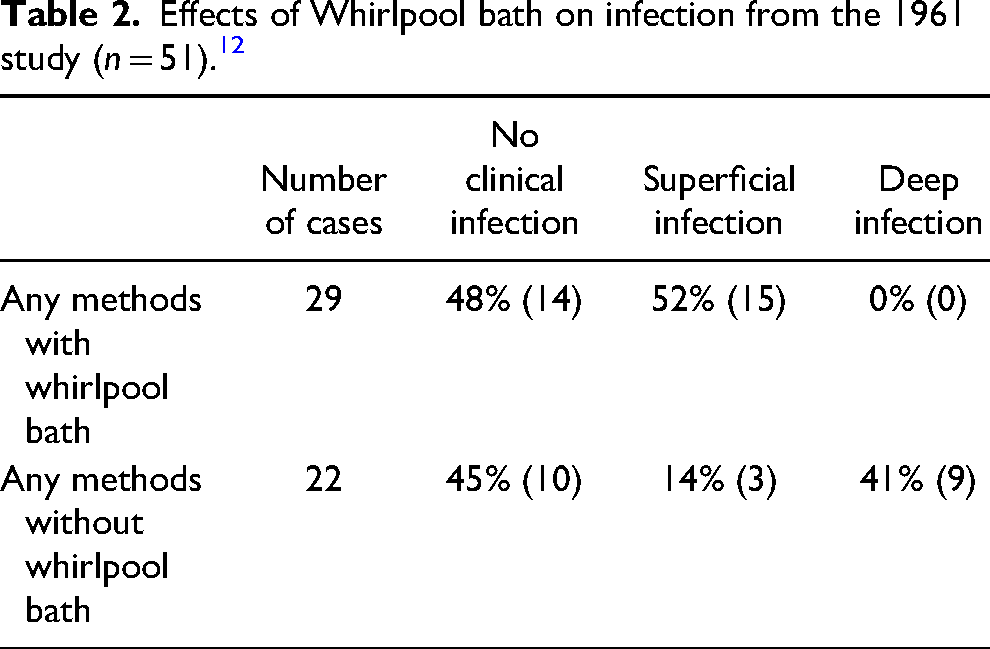
In the first paper, the whirlpool bath was recommended for physiotherapy and applying ultrasound in a water environment. The whirlpool bath, which contained hexachlorophene detergent, was applied twice daily for 20 min, and ultrasound was applied during the bath to improve the circulation in deep structures. In cases of superficial injury, there was subjective evidence of the benefit of the ultrasound. However, it was concluded that the use of ultrasound in deep injuries was harmful.12,13 Therefore, ultrasound was not applied in the following years.
The effect of the whirlpool baths on the prevention of deep infection was impressive. The prevalence of severe infection was reduced to zero (Table 2). In addition, gentle movement of water detached the dead tissues that were ready for separation, thus performing a physiological atraumatic debridement as well as stimulating massage of tissues. It also rapidly reduced edema due to increasing local circulation, and pain was relieved after serial whirlpool sessions.12,13
Effects of Whirlpool bath on infection from the 1961 study (n = 51). 12
Active exercise of digits was recommended as soon as possible after thawing. Patients were encouraged to increase their range of joint motion during both bedside physiotherapy and whirlpool baths. 13
Dr Mills reported that patients were routinely placed on broad-spectrum antibiotics (as occurs with open fractures) for the first 4 years of their study. Subsequently, however, antibiotics were ordered only after definite indications and based on culture and sensitivity studies because the outcomes showed that their use was not necessary for the majority of patients utilizing whirlpool bath therapy.13,20 It was presumed that this occurred because the germicidal agent (hexachlorophene) in the bath reduced the number of bacteria and disrupted their metabolism. They also suggested using an open method during treatment (without dressing) and avoiding early-stage debridement. The general principle of treatment in the current guidelines from the Wilderness Medical Society 1 is to selectively drain clear blebs and leave hemorrhagic blisters intact.
The results of the first series of patients 12 demonstrated poor outcomes after debridement. The ultimate outcomes were poor in those patients who were infected and debrided or who were debrided and developed infection following debridement (Tables 3 and 4). Mills et al advised that debridement or amputation in the early stages (first to the third week) should be avoided. The only condition in which debridement could be beneficial was when dry eschar retracted and caused necrosis, muscle atrophy, or joint motion restrictions.12,13
Debridement and infection from 1961 study (n = 51). 12
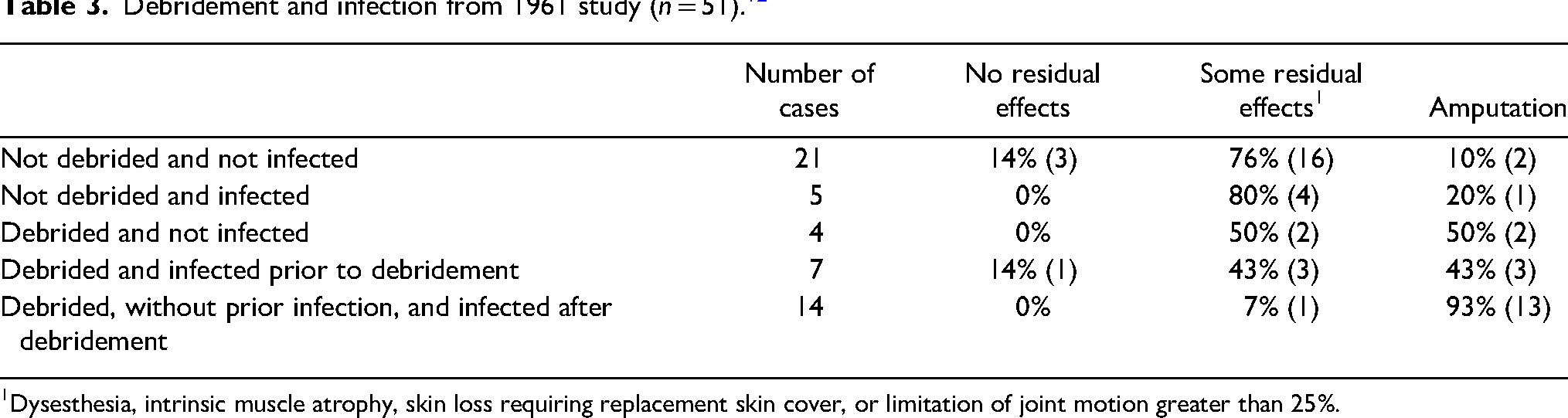
Dysesthesia, intrinsic muscle atrophy, skin loss requiring replacement skin cover, or limitation of joint motion greater than 25%.
Effects of debridement on ultimate results from 1961 study (n = 51). 12

In summary, Mills recommended frozen parts should be protected from trauma. He described three conditions in which thawing should be postponed: 1) if severe freezing occurred and walking on frozen feet was not avoidable, it would be better to leave the limb frozen because travel on the thawed part that is swollen, painful, hyperemic, and blistered is difficult or impossible; 2) he recommended avoiding thawing an extremity if there was the risk of refreezing because the outcome of refreezing is very poor and usually results in amputation. Indeed, he suggested that if severe frostbite occurred, the limb may best be left in its frozen state until the victim is rescued or reaches shelter, and 3) if there was a chance to thaw by rapid thawing within a short time, it would be reasonable to delay thawing until reaching a rapid thawing venue instead of using other slower methods for thawing. 13
Diagnostic Tools and Advanced Care
In 1960, Mills et al demonstrated for the first time the efficacy of radioisotope scans (technetium-99 m) to determine blood flow and to assess the degree of injury, prognosis, and effectiveness of therapy (Figure 4). 13 In 2000, Cauchy et al incorporated radioisotope scans into their globally accepted classification scheme for frostbite severity.21,22
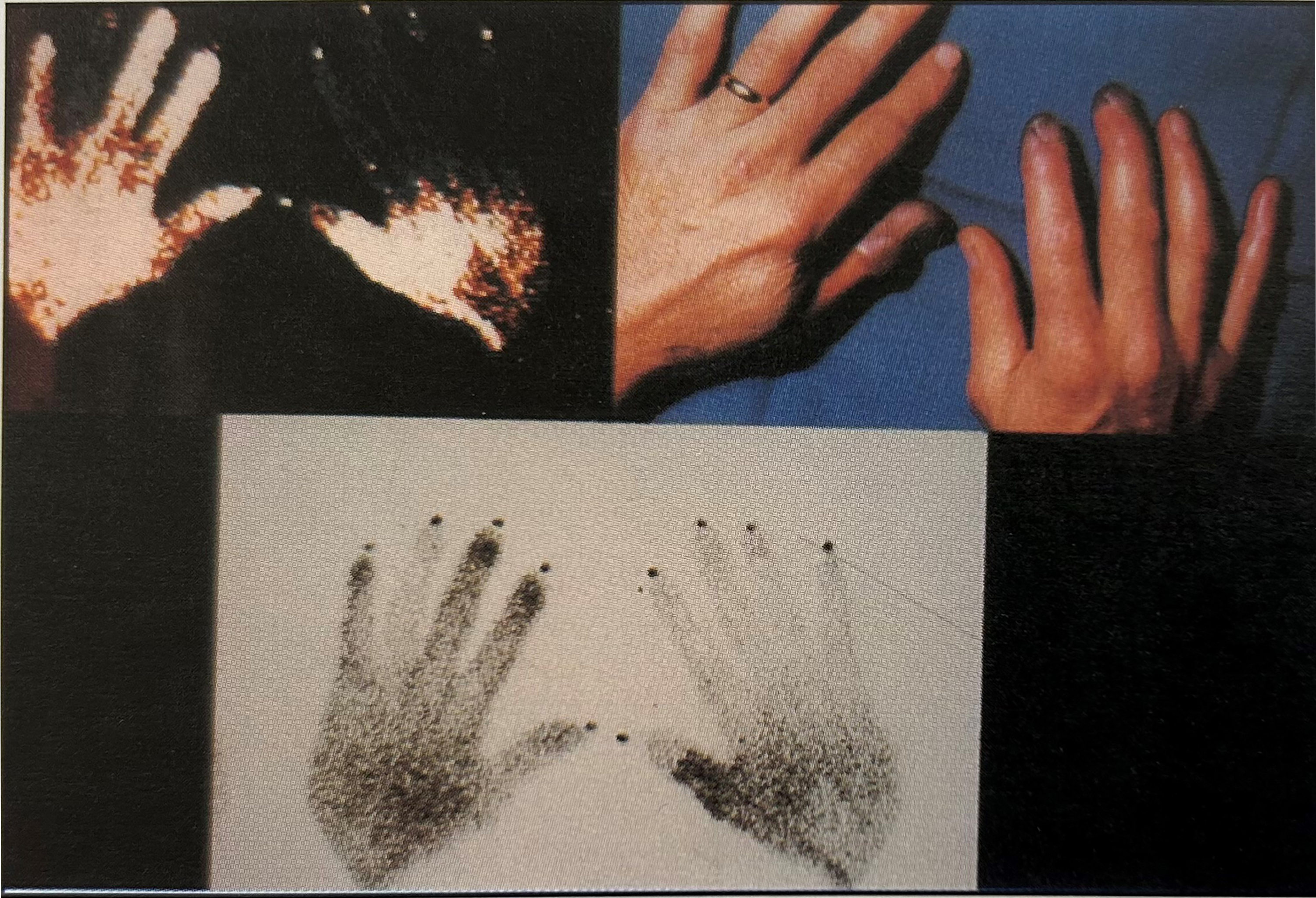
For early prognosis of cold injury, superficial tissues should be evaluated with infrared thermography (top left) and deep tissues with isotope study (technetium-99 m) (bottom).
During this period, Dr Mills and his colleagues also simplified the classification of frostbite from 4 degrees to 2 degrees because the latter system was easier and more practical for field use. Superficial frostbite is limited to the skin and corresponds to the traditional first- and second-degree frostbite. Deep frostbite involves tissues beneath the skin, including muscle, tendon, nerve, blood vessel, and bone and corresponds to the traditional third- and fourth-degree frostbite. 12
In 1973, Mills published treatment results for 200 patients (included in Table 1). Although rapid rewarming remained the most effective acute treatment, he added new elements to the treatment of frostbite. He noted that in some cases, edema could increase tissue pressures to the point of compromising distal blood flow. He performed fasciotomy in these patients with positive results (Figure 5). 23 Mills also reported improved healing with skin grafts if rapid rewarming had occurred. Results were less successful following spontaneous or delayed thawing by snow or ice. The procedure of grafting could be considered in many cases to prevent exposure and consequent necrosis of tendons and underlying fascia and joints.15,18 Mills studied the effect of silver nitrate 0.5% by applying it to one side of bilateral hand or foot injuries of similar magnitude. He reported that this treatment decreased pain and infection but that epithelialization was similar to that produced by the surgical soaps. 23
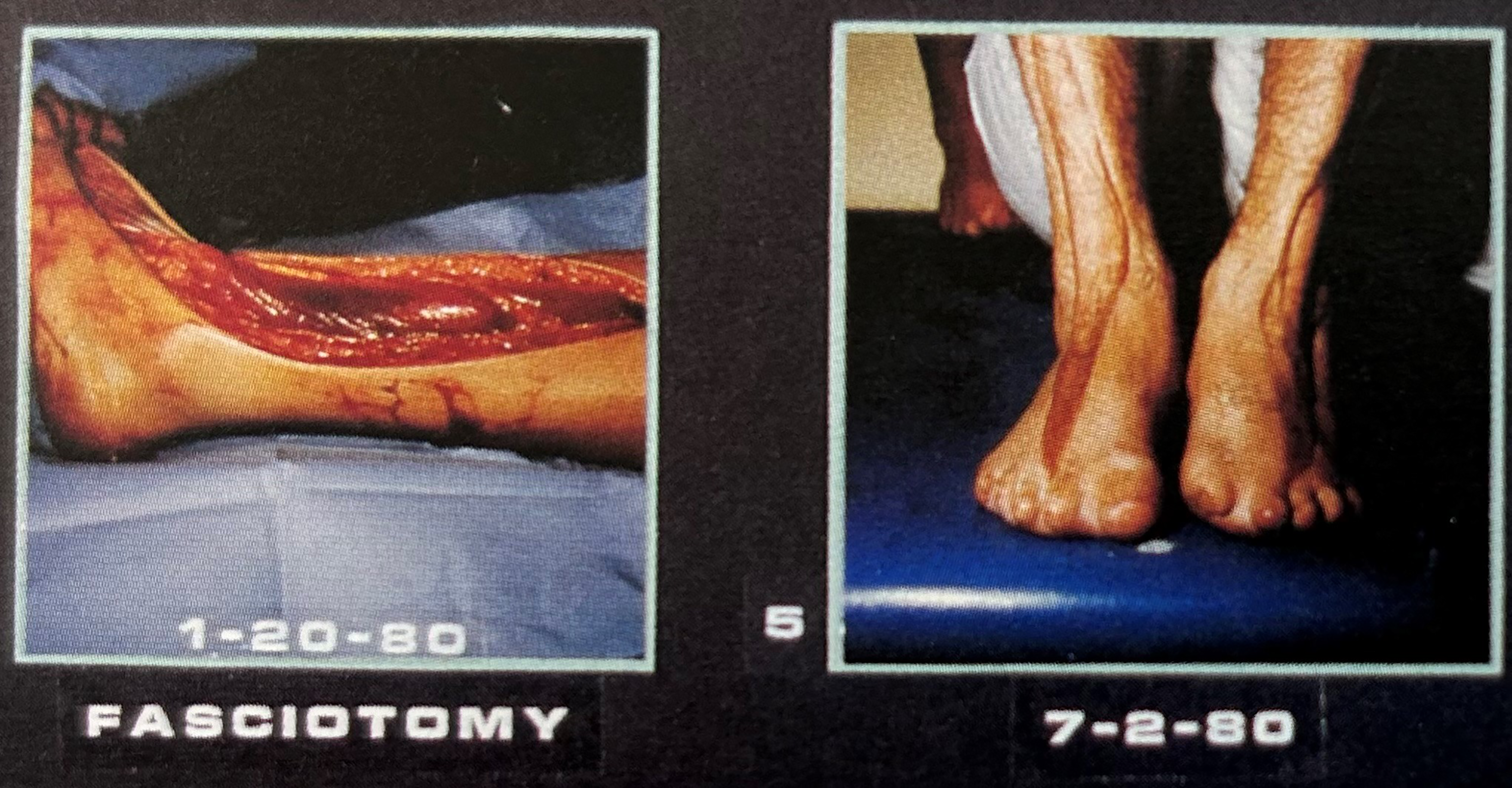
Fasciotomy process for patients with frostbite superimposed on immersion injury. Subfascial tissue pressures in the feet were >100 mm Hg.
In 1983, Dr Mills summarized the treatment of frostbite from 800 cold injury cases, confirming the efficacy of rapid rewarming. He also described new modalities that had been studied. 18 He described three types of post-thaw injuries: 1) vasoconstriction after thawing; 2) arterio-venous-capillary thrombosis after injury; and 3) cell destruction. 18
Mills studied vasodilating agents (tolazoline hydrochloride); anticoagulants (heparin), vasodilators (priscoline), hypotensive adrenergic blocking agents (guanethidine, reserpine), sympatholytic drugs (dibenzyline), hemorheological agents (oxpentifylline); calcium blocking agents (nifedipine); sympatholytic agents (phenoxybenzamine hydrochloride); and dimethyl sulfoxide (DMSO). He also proposed that the use of thrombolytic enzymes (streptokinase, urokinase) for deep thrombosis should be evaluated. He explained, “The risk of hemorrhage and lysis of fresh fibrin may limit the use of these drugs with associated trauma, especially in head trauma where the cerebral vascular bleed may be of concern.” He suggested that the administration of these drugs needed special considerations. 18
Mills recommendations that are still accepted today include: low molecular weight dextran (a plasma volume expander); tissue plasminogen activator (tPA) (a thrombolytic enzyme); and NSAIDs such as ibuprofen. 16
Dr Mills used biofeedback training for labile vasomotor changes and intermittent vasoconstriction cases starting in 1976. Based on thermal biofeedback training, the skin temperature could be an indicator of vasodilatation. The average dorsal digital surface skin temperature at rest for healthy females was 31°C and for healthy males was 33°C. Patients with frostbite, thermal disorders, or distressed individuals had lower extremity skin temperatures ranging between 15–21°C. It was demonstrated that most of these patients could increase digital skin temperature by 10°C after 10–15 half-hour training sessions of biofeedback (total of 5 to 7.5 h). 24
These techniques were applied in warming some post-thawed frozen digits and continued to be part of the Providence Hospital frostbite treatment protocol. 25 Dr Mills reported that biofeedback training could be an option for the prevention of stress and providing vasodilatation on demand for people who are in danger of cold injury, especially in very stressful circumstances (eg, military operations). 25
By 1993, Mills was able to provide results from a total of 1026 cases of cold injury. While this paper did not provide any new treatment options, it did report on long-term follow-up with X-rays. Mills reported that significant changes in bone and cartilage were observed long after freezing injury (Figure 6). Radiographic changes appeared after 6-18 months. Changes ranged from large areas of avascular necrosis of bone to small punctate, lytic changes in affected digits. Mills recommended that every frostbite patient should have serial X-rays from early to late stages to identify any lesions that were due to freezing. The X-ray file would help to rule out other diagnoses in the future if those lesions were discovered independently. 16

X-ray of previously frostbitten foot. Left image, 7 weeks post-injury reveals no definite degenerative changes. Right image, after 14.5 years, several chronic sequalae include narrowing of all joints, fibrin filled destructive lesions in periosticular joint areas.
In 1993, Mills summarized factors that predict the prognosis of freezing injury. Factors favoring a good prognosis included: short duration of freezing, superficial depth of injury, freezing without any other insult (fracture, hypothermia, immersion injury, or other trauma), the existence of large and distal clear blebs after thawing, and early return of perfusion after thawing (Mills typically detected this by technetium 99 radioisotope studies). 16
Factors predicting a worse prognosis included: long duration of freezing, superimposing frostbite on other traumas (fracture or dislocation, or soft tissue trauma), and association with an existing medical condition (eg, vascular deficiency, hypovolemia, or hypoxia).
Factors predicting the worst prognosis included: delayed thawing (ice, snow, friction massage); thawing by excessive heat (higher than 49°C); the existence of proximal, dark, hemorrhagic blebs after thawing; early necrosis with early mummification within 4 to 5 days; perfusion deficiency (detected by technetium 99 studies on early and repeated views); and freeze-thaw-refreeze injury. 16
As Mills neared the end of his storied career in investigating frostbite, he proposed future research on the topic. He recommended investigating the involvement of oxygen free radicals, activated neutrophils, and other inflammatory and immune responses in cold injury damage. 26 He also suggested further study of how cold injury of the endothelium affects flow patterns, alters permeability, and causes the release of substances that enhances clot formation. 19
Conclusion
Dr William J. Mills was instrumental in changing the treatment of frostbite from delayed thawing with ice and snow, which had been standard practice for 140 y. Starting in the late 1950s, he clearly demonstrated the value of rapid rewarming in warm water and established many procedures for long-term care and prognosis. Over a career of 40+ years, Mills treated or consulted in more than 1500 cold injuries including more than 1000 frostbite cases. His publications have been cited in numerous guidelines and textbooks.
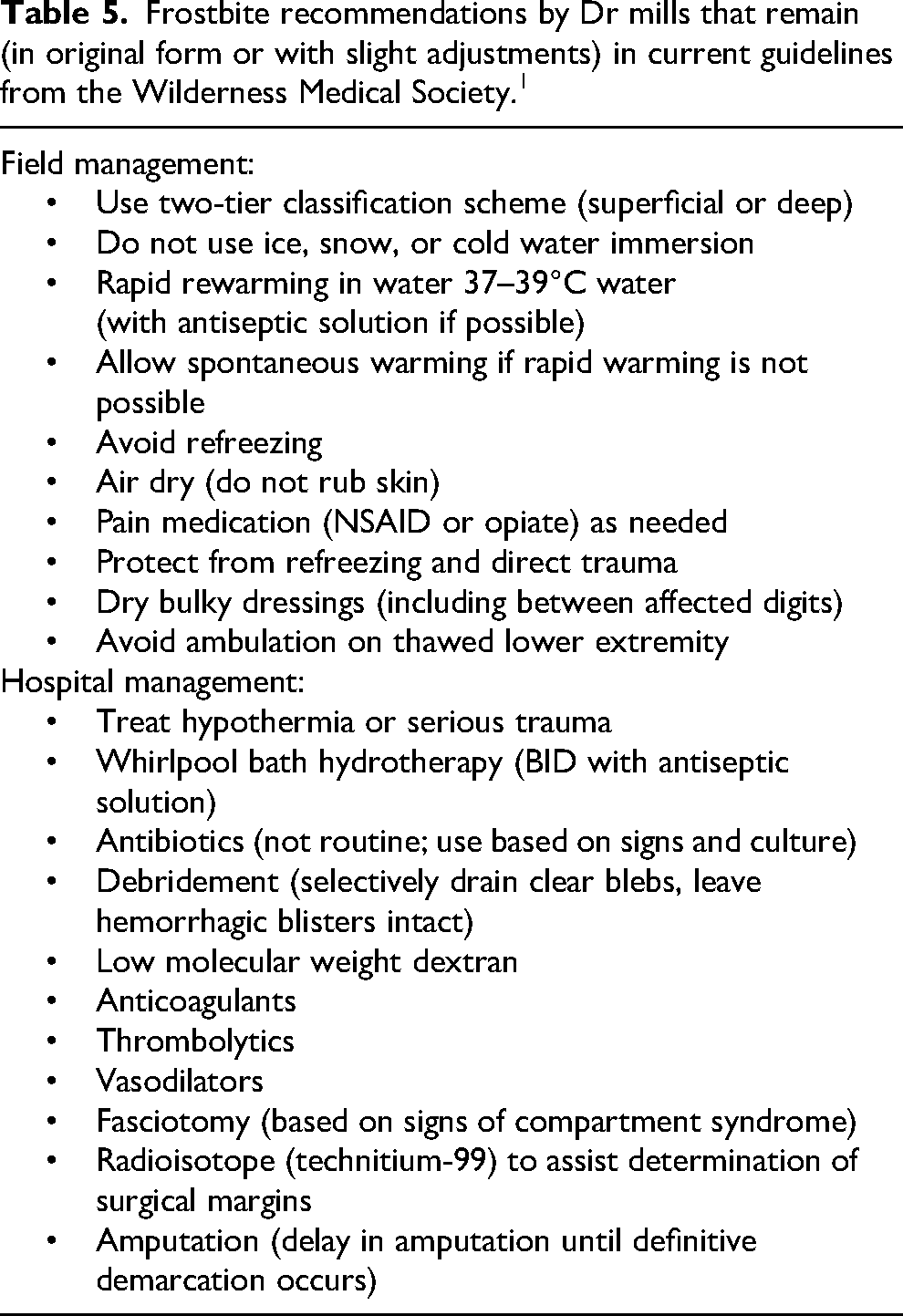
Isaac Newton wrote in a letter to Robert Hooke, “We stand on the shoulders of giants” (author's paraphrase). This sentiment certainly applies to our present understanding and recommendations for the treatment of frostbite. William Mills is indeed a giant in the area of frostbite treatment because of his influence both in changing a century-old dogma and establishing principles that still apply today. As a final testament to this fact, Table 5 summarizes results and recommendations from Dr Mills that have survived the test of time and appear in the current WMS frostbite guidelines. 1
Frostbite recommendations by Dr mills that remain (in original form or with slight adjustments) in current guidelines from the Wilderness Medical Society.1
Footnotes
Acknowledgment
This study was partially funded by the Natural Sciences and Engineering Research Council of Canada.
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Sciences and Engineering Research Council of Canada.