
Abstract
Frostbite, a severe cold injury resulting from exposure to subfreezing temperatures, damages the skin and underlying tissues of the affected area and ranges in severity from first to fourth degree. This case report investigates the impact of second-degree frostbite suffered by a marine during winter training on cold-induced vasodilation (CIVD). Comparisons of CIVD before and after the injury revealed significant alterations in CIVD responses. CIVD, a physiological mechanism characterized by blood vessel dilation in response to cold exposure, plays a crucial role in operating in cold-weather environments and enhancing dexterity. The marine exhibited prolonged CIVD onset time, lower finger temperatures, increased pain sensations, and diminished dexterity after the frostbite injury during follow-up CIVD testing. The findings suggest that the frostbite-induced damage possibly compromised the microvascular function, contributing to the observed changes in CIVD. The marine reported persistent cold sensitivity and difficulty in maintaining hand warmth when assessed postinjury. This case underscores the potential long-term consequences of frostbite on CIVD and manual dexterity, emphasizing the importance of understanding these physiological changes for individuals engaged in cold-weather activities, particularly for military and occupational personnel.
Introduction
Frostbite results from exposure to freezing temperatures, causing damage to the skin and underlying tissues. Injury severity is categorized from first to fourth degree based on the depth of tissue involvement. Second-degree frostbite injury is characterized by superficial skin vesiculation along with erythema and edema surrounding the blisters. 1 Although second-degree frostbite does not normally cause permanent skin damage, it can take up to 6 months for skin to heal and may pose significant challenges in terms of management and functional recovery. 2 Several studies report that frostbite injuries can result in long-term vasomotor disturbances, neuropathic and nociceptive pain, and cold allodynia (increased sensitivity to normally nonpainful cool temperatures). 3
Cold-induced vasodilation (CIVD) typically occurs 5–10 min after cold exposure (individual variability is observed), wherein blood vessels in the hands and feet vasodilate and vasoconstrict in a cyclic pattern, allowing periods of warm blood to reach the tips of the fingers and toes. 4 CIVD occurs in both cold air and water; however, CIVD responses are most often measured in laboratory studies during cold-water hand or finger-only immersion. Previous investigations suggest that CIVD may reduce the risk of local cold injuries in certain cold environments 5 as well as improve manual dexterity and tactile sensation during cold-weather exposure. 6 It is plausible that, after incurring a cold-weather injury such as frostbite, the CIVD response could weaken due to damage to the underlying tissues and vasculature, thus increasing the risk for subsequent cold injury. However, no investigations have examined CIVD responses before and after a frostbite injury.
The Naval Health Research Center performed an evaluation of the health, readiness, and performance of U.S. marines engaged in a 3-week winter warfare training exercise. The aim of the study was to identify factors that influence marine resilience during mountain warfare training. Prior to the 3-week field training (pre) and approximately 2 weeks after returning home from the field training (post), participants completed a 30-min hand immersion in cold water to evaluate CIVD responses. Our intent in performing pre- and post-training CIVD assessments was to evaluate how CIVD changed during winter field training. This case report developed from a training accident where a marine, who was also a research participant enrolled in our study, experienced a second-degree frostbite injury during the field training. As such, we were able to measure CIVD responses 15 days following the frostbite injury (as was the plan for all noninjured participants in the study).
This case report presents an analysis of a U.S. marine who suffered a second-degree frostbite injury during a winter training exercise, with a specific focus on the impact on postinjury CIVD. By presenting this case, we aim to enhance understanding of cold-weather injury risk among those who recreate, work, and conduct military operations in cold-weather environments.
Case Report
A 25-year-old male (U.S. marine) took part in a data collection session as an enrolled research participant (height: 185 cm; weight: 89.8 kg; % body fat: 20%) while participating in a winter training event. The night before the frostbite injury occurred, the marine and his unit completed a 7.6 km hike with 580 m elevation gain and reached a location where they made camp for the night (2680 m). At 0545 the next day, the Marine awoke after sleeping for 7 h 54 min with a sleep efficiency of 80%, suggesting modestly/mildly fragmented sleep (information collected from the marine's sleep tracking device; Oura ring: Gen 2; ŌURA Health Oy; Oulu, Finland). Upon awakening, he performed a short warm-up hike and learned that, overnight, another marine had accidentally left his mittens outside the tent, where they froze in the snow. Consequently, the marine used a different pair of lightweight (but dry) gloves for a snowshoe hike with his unit later that morning. During the short (20–30 min) snowshoe hike, he indicated that his hands slowly lost strength until he could no longer hold his trekking poles. The marine was evaluated by a nearby corpsman, who diagnosed the marine with second-degree frostbite involving the second through fifth digits of the right hand and the third and fourth digits of the left hand (Figure 1). The mean, maximum, and minimum air temperature that day was −12.7 °C, −2.4 °C, and −21.0 °C, respectively. The marine indicated no history of prior cold-weather injury. After leadership discovered the frostbite injury, he was evacuated from the field and taken indoors, where he was instructed to immerse his hands into warm water. As blisters formed, a corpsman aspirated and bandaged them. His treatment and removal from the field lasted less than 3 days before he returned to the field to continue training with his unit. Blisters continued to form after he returned to the field. At 3 months postinjury, he indicated that feeling had returned to his fingers. However, at 4 months postinjury, he continued to report increased cold sensitivity, difficulty keeping his hands warm, and sensations that his hands were cold to the touch. Additionally, 2–3 nights/week, he reports waking up due to his hands feeling cold.
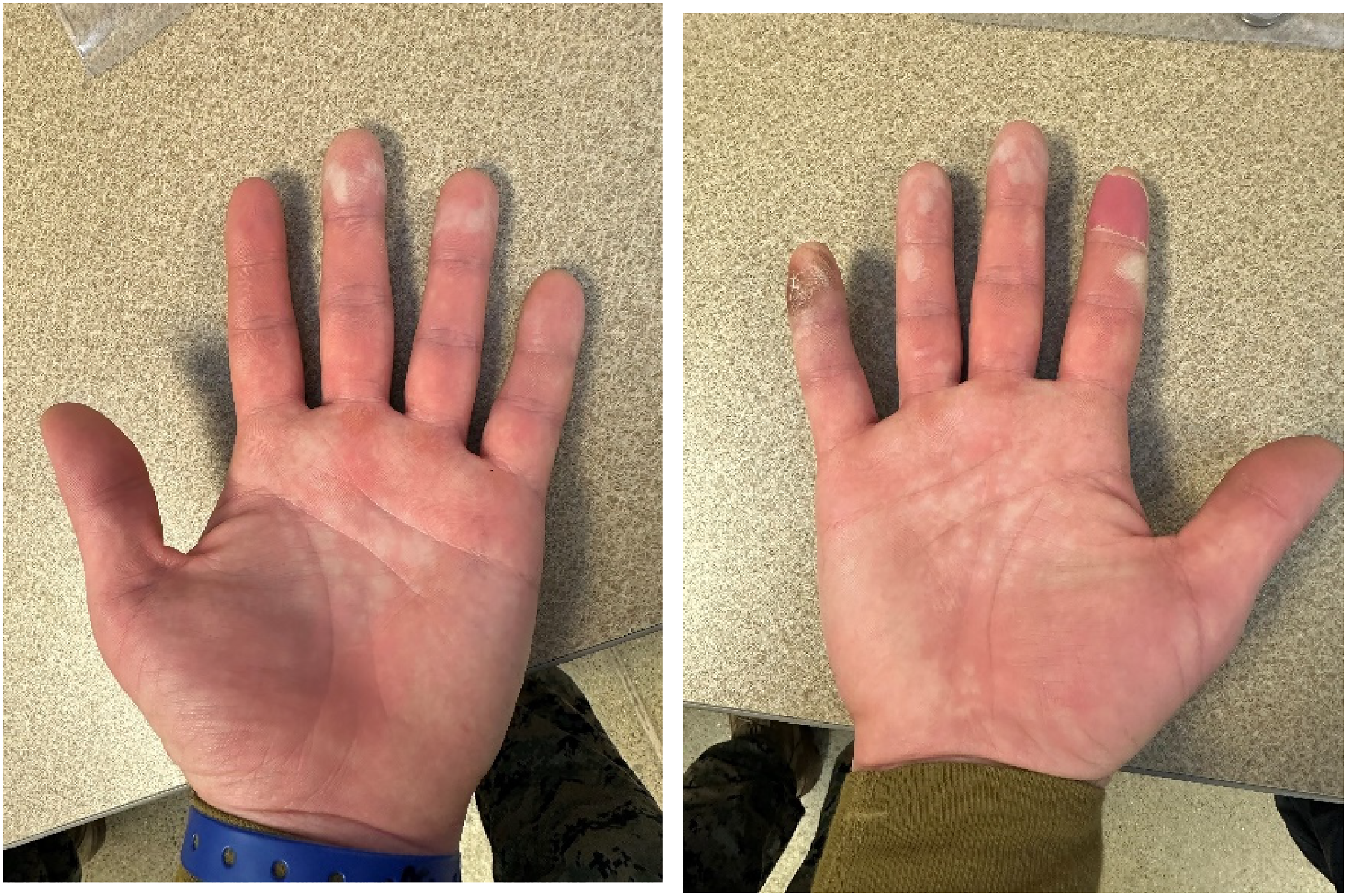
Images of marine's frostbite injury to the left and right hands taken on February 5, 2023 (17 days after injury onset). Photographs courtesy of Naval Health Research Center.
As part of the research effort, the marine performed two 30-min hand immersions in 8 °C water. These immersions were performed approximately 2 weeks before the marine deployed for winter warfare training (preinjury) and approximately 2 weeks after returning from the training (postinjury). Each test was conducted at the marine's home military base at sea level in an indoor environment (27 °C). Twenty-four hours before each immersion, the Marine was instructed to avoid alcohol, tobacco, caffeine, and vigorous exercise.
Before and after each immersion, the marine's dexterity was evaluated using a Purdue Pegboard Test (Model 32020; Lafayette Instrument Co., Lafayette, Indiana). The test required the marine to place as many metal pegs (25.4 mm length × 3.2 mm diameter) into 3.2 mm diameter holes on a board as quickly as possible within 30 s using only the dominant hand (right). The number of pegs correctly placed was scored and served as a strong indicator of dexterity performance. Following the dexterity test, the marine was instrumented with skin temperature sensors placed on the pads of the second, third, and fourth digits of the right hand. Prior to immersion, the Marine was fitted with a nitrile glove to protect the sensors from water. The marine immersed the hand first in 35 °C water for 5 min (to standardize starting finger temperatures) and then immediately placed the hand (to the level of the wrist) into 8 °C water for 30 min. Skin temperatures of the second, third, and fourth digits were captured each minute, and ratings of pain (0–10) and thermal sensation of the hand (−4 to +4) were collected every 2 min. In addition to assessing CIVD responses during immersion, we also evaluated recovery by allowing the hand to spontaneously rewarm following removal from cold water. Thermal images of the hand were taken before, after, and during rewarming (FLIR E4, FLIR Systems Ltd, Kent, UK). From the finger skin temperature data, we calculated the CIVD onset time (the time from the start of immersion to the first vasodilation episode), minimum finger temperature (lowest finger temperature recorded during immersion), and mean finger temperature (the average finger temperature during immersion from min 5–30). We calculated each of these for all digits and then averaged all three (second, third, and fourth) digits (Table 1). Additional measurements were assessed as part of the research effort, and we have included other relevant data in Table 1.
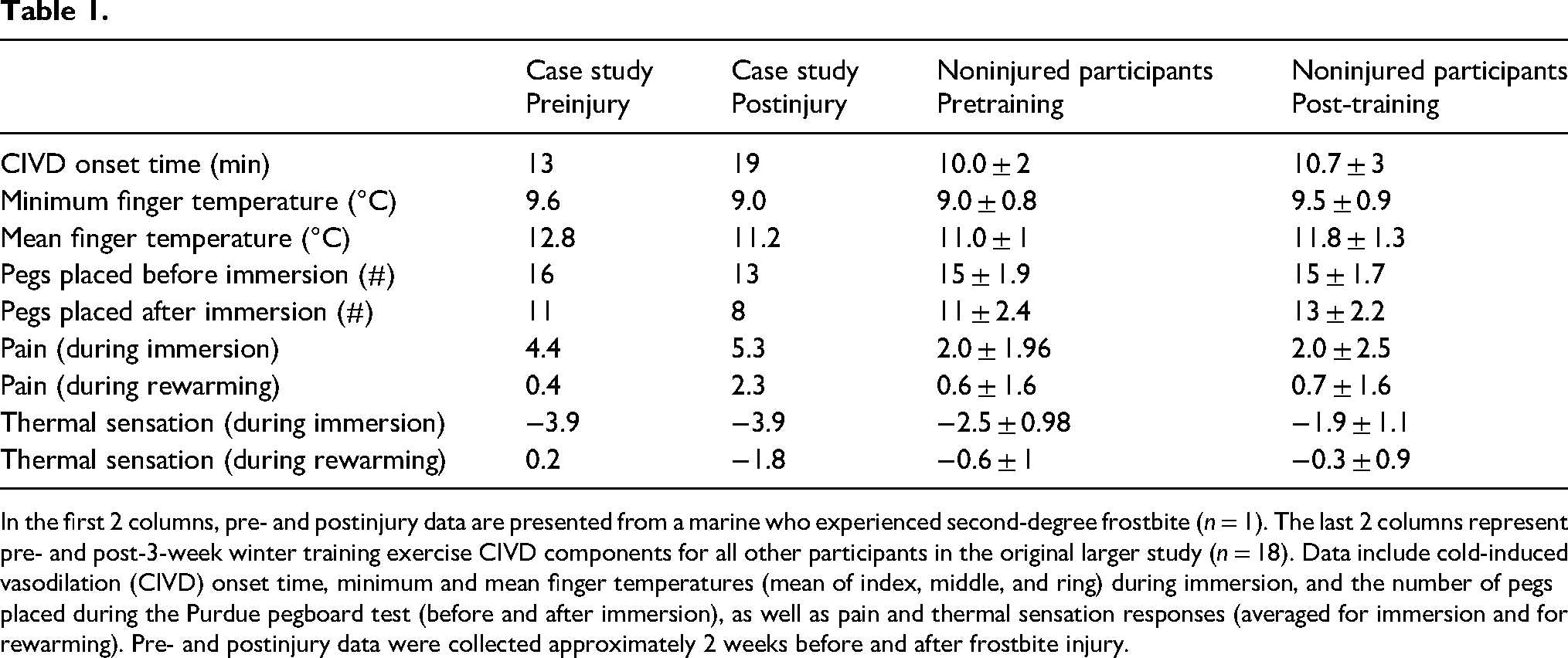
In the first 2 columns, pre- and postinjury data are presented from a marine who experienced second-degree frostbite (n = 1). The last 2 columns represent pre- and post-3-week winter training exercise CIVD components for all other participants in the original larger study (n = 18). Data include cold-induced vasodilation (CIVD) onset time, minimum and mean finger temperatures (mean of index, middle, and ring) during immersion, and the number of pegs placed during the Purdue pegboard test (before and after immersion), as well as pain and thermal sensation responses (averaged for immersion and for rewarming). Pre- and postinjury data were collected approximately 2 weeks before and after frostbite injury.
Comparisons between preinjury and postinjury revealed that, after frostbite injury, the marine experienced a longer CIVD onset time, lower finger temperatures, increased pain sensations, and worse dexterity (Table 1). In the context of the larger study, pre- and post-CIVD values are included in Table 1 for comparison between the case study and the remaining (noninjured) participants. Additionally, the marine indicated that his hand felt colder during recovery when assessed at postinjury. Grip strength, a gross motor skill, remained unchanged (preinjury: 28 kg, postinjury: 29 kg).
Description
Cold-weather injuries represent a threat to the health of individuals and to military training and operations. In 2021–2022, frostbite was the most common type of military cold-weather injury across all military services, accounting for more than 50% of all cold-weather injuries, both within the United States and overseas. 7 Frostbite severity depends on many factors, such as environmental conditions, thermal protection and clothing, exertion and fatigue, prior history of cold injury, and any underlying medical conditions impacting vascular health. 8 The only known contributing factor to the marine's injury was insufficient thermal protection from the prevailing environmental conditions, which was brought about by accidental circumstances. Additionally, the minimum air temperature was −21 °C at an elevation of approximately 2438 m, and heavy physical exertion was performed the day before; however, no previous cold injury or ailments were reported.
Once the frostbite was discovered, immediate treatment followed standard medical protocol: rewarming the affected site with warm water and early debridement of all blisters. 9 Many patients who incur a frostbite injury experience permanent changes in their microcirculation, a reduced sensation of the affected area, or even hypersensitivity, vasospasm, and/or chronic pain. 10 Given that this marine was also enrolled in a research study, a unique opportunity was available to examine the effects of a frostbite injury on CIVD responses.
Following frostbite injury, several elements of the CIVD response were adversely affected, with onset time the most impacted, suggesting a delayed CIVD response possibly related to damaged microvasculature of the affected fingers. Previous studies examined changes in CIVD during a 2-week Arctic military exercise (although not associated with frostbite injuries) and found similar results: a reduction in minimum and mean finger temperatures and increased CIVD onset time. 11 For the marine in the present case study, the damage to the underlying tissue likely exacerbated the vasoconstrictive response seen during the CIVD test. Figure 2 illustrates the injured marine's CIVD response before and after frostbite occurred and a comparison to the noninjured participants. When cell membranes are damaged, the microvascular function is compromised, and a general increase in vasoconstrictor tone occurs due to the raised vascular reactivity to cold.11,12 Both the immersion period and rewarming were adversely affected by frostbite. Compared to pre-injury, his hand felt much colder after spontaneous rewarming, and pain ratings increased four-fold. Additionally, fine motor dexterity was impacted by the frostbite injury. A reduction in dexterity can hinder performance, productivity, and safety. The participant reported not being able to feel his fingertips until 3 months postinjury, indicating that the injury resulted in a sustained loss of tactile sensation. When tactile feedback is diminished, it becomes more difficult to gauge the force, texture, and shape of objects, making it difficult to control the precise movements required for optimal performance.
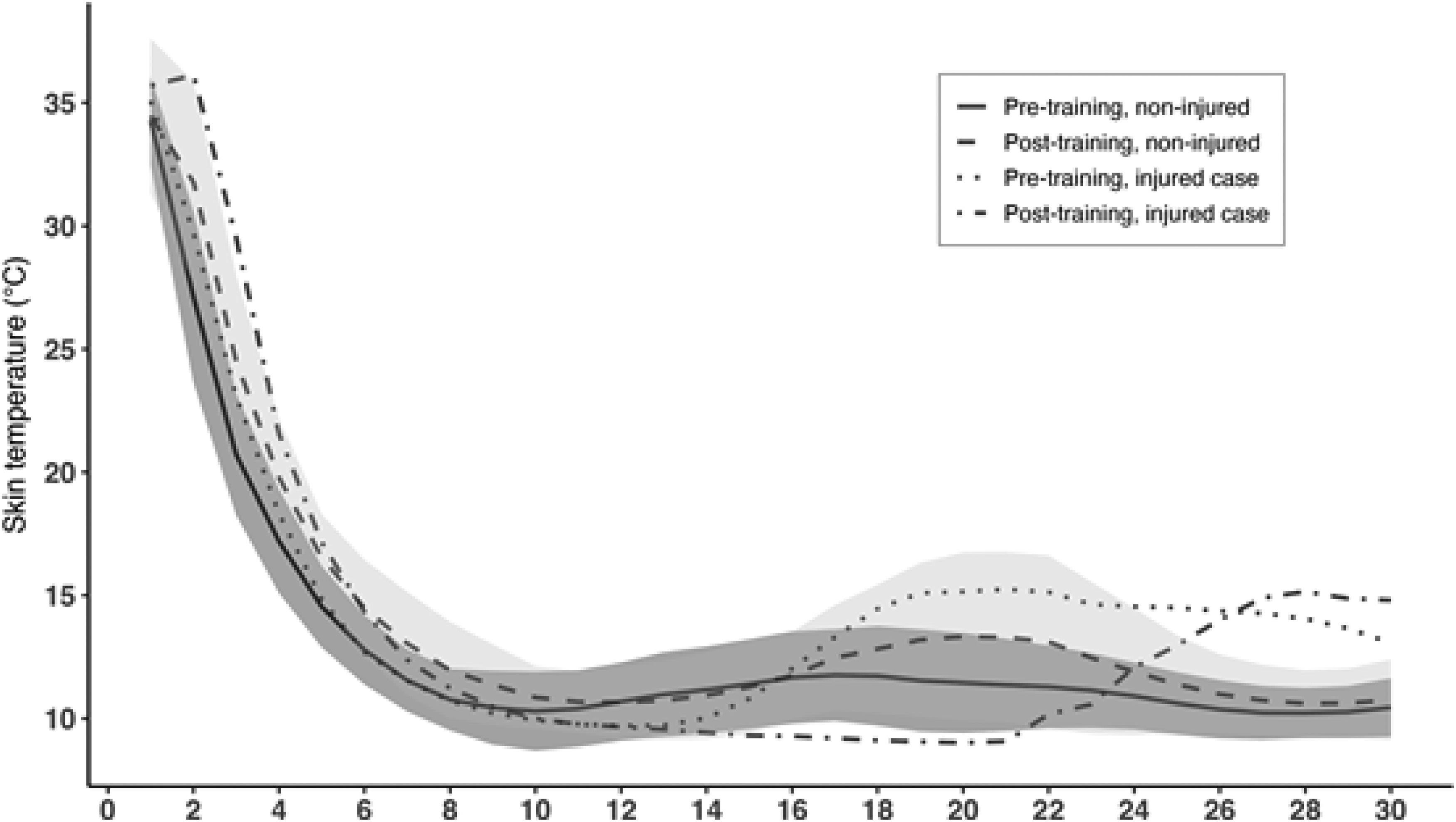
Noninjured (n = 18) participants average compared to injured (n = 1) pre- and post-training event CIVD responses. Standard deviation error bands are included for minute 1 to 30. Standard deviation lines are limited to the negative side for the “pre-training, non-injured” group and to the positive side for the “post-training, noninjured” group.
A major limitation of the case report is the unknown long-term outcome of the marine since we were unable to perform additional CIVD assessments to gauge whether the delayed CIVD onset was transient or more long lasting. Additionally, there were several uncontrolled factors that could impact the CIVD response, such as diet, cold acclimatization, and mental state, all of which could influence the response to cold stress. We cannot be certain that frostbite is solely responsible for the delayed CIVD response, but this does offer an intriguing point of discussion in that CIVD testing could possibly be used as a tool to assess frostbite injury recovery, albeit this requires further investigation.
This case study demonstrated that a delayed CIVD response following cold injury may be present for this individual marine, which could be problematic for the risk of future cold injuries if this response is persistent. Additional investigations in this area would benefit individuals with a high risk of frostbite injury.
Footnotes
Acknowledgments
We gratefully acknowledge the data collection support from Joseph Cuellar, Max Smith, Timothy Dunn, Brandon Schrom, and Pinata Sessoms.
Author Contribution(s)
Disclaimer
I am a military service member or employee of the U.S. Government. This work was prepared as part of my official duties. Title 17, U.S.C. §105 provides that copyright protection under this title is not available for any work of the U.S. Government. Title 17, U.S.C. §101 defines a U.S. Government work as work prepared by a military service member or employee of the U.S. Government as part of that person's official duties. This work was supported by the Office of Naval Research under work unit no. 62417. The views expressed in this research are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. Government. The study protocol was approved by the Naval Health Research Center Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human subjects. Research data were derived from an approved Naval Health Research Center Institutional Review Board protocol, number NHRC.2019.0007.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Office of Naval Research.