
Abstract
We describe a case of severe accidental hypothermia of a kayaker with preserved consciousness and shivering despite a rectal temperature of 22.9°C following a 50-min immersion in 3°C water with an estimated core temperature cooling rate of 10.6°C/h. Based on survival at sea prediction curves and cooling rates from physiology studies, cold water (eg, 0–5°C) immersion is expected to drop core temperature by 2 to 4°C/h. Furthermore, accidental hypothermia classification systems predict that severely hypothermic patients are usually unconscious and not shivering. The patient in this report rewarmed rapidly at 3.6°C/h with only minimally invasive measures and was discharged fully neurologically intact. In 41 similar cases of survival in moderate to severe hypothermia with core temperatures <32°C due to cold water immersion, cold air exposure, or avalanche burial, mean cooling rates were 4.3±3.3°C/h (range 0.4–10.6°C/h). Including the current patient, shivering was reported in only four cases. We found several other cases of rewarming from moderate to severe hypothermia with only minimally invasive measures. The current and summarized cases lead us to conclude that patients may be at risk of severe hypothermia in <60 min of cold water immersion and that it is possible for severely hypothermic patients to have preserved consciousness, close to normal vital signs, and shivering. Minimally invasive or noninvasive rewarming of patients with severe hypothermia is also possible, especially in those who continue to shiver. Hypothermia management should not necessarily be guided by classification systems or core temperature alone but rather by a careful consideration of the entire clinical picture.
Keywords
Introduction
Accidental hypothermia is a drop in core temperature to <35°C. The stages of accidental hypothermia are often defined based on clinical symptoms and core temperature. 1 According to the two commonly used classification systems,2,3 shivering ceases and consciousness is lost at core temperatures <30 to 28°C, and vital signs are often absent below 24°C. Recent work, 4 however, has shown that the measured core temperature does not always correlate with the clinical signs and that there can be significant overlap between the classification groups.2,3 A review of experimental studies 5 and predictive modeling6,7 suggests that patients immersed in very cold water will cool at a rate of 2 to 4°C/h. Some case reports,8–13 however, have shown much faster cooling rates, up to 14°C/h. 14 The potential for major discrepancies between expected and actual cooling rates for severely hypothermic patients is not well recognized. Rewarming rates in a hospital setting are usually 0.1 to 3.4°C/h using active external and minimally invasive methods, 15 but this may be an underestimation for patients who continue to shiver.
We describe a young adult male with severe accidental hypothermia and a rectal temperature (Tr) of 22.9°C after only 50 min of immersion in 3°C water and 30 min of field warming and transport to hospital. The estimated cooling rate was 10.6°C/h, and the patient had preserved consciousness, shivering, and rapid rewarming with only minimally invasive methods. We also summarize and discuss similar patients from the medical literature.
Case Report
The patient was a 31-year-old male kayaker with a weight of 71.6kg, height of 178cm, and athletic build with a body mass index of 22.6 kg/m2. The incident took place in midafternoon in Penticton, Canada, in March 2021. The patient had consumed 4 beers and smoked an undetermined amount of marijuana. He was wearing denim jeans, cotton underpants, a cotton hooded sweatshirt, and a winter hat. He did not have any safety gear or a personal floatation device. Air temperature was 13°C with a wind speed of 20 km/h. He was kayaking alone in a sit-inside kayak without the spray skirt attached. Within 10 min of paddling, he capsized, after which he was initially fully submerged in a slow-moving freshwater, partially ice-covered lake with a water temperature of 3°C. Within 10 min of capsizing, he called 911 from his own waterproof cell phone at 1537h. The phone call lasted 41min, until 1618h. He was immersed to his mid torso and he was holding on to the hull of the kayak with his arms wrapped around a cord on the hull while intermittently trying to kick back to shore.
After 50 min in the water, a firefighter rescue boat reached the patient, who experienced loss of consciousness as he was pulled from the water. Transport to shore was done with the patient fully clothed on the back bench of the boat, and this took approximately 10min. A friend who had also been searching for the patient had boarded the rescue boat, took off his own shirt, and attempted body-to-body warming under a blanket. There was a suggestion to direct the boat to a nearby house where the patient could be placed in a hot tub; this suggestion was wisely rejected by the rescue crew. The patient's clothes were removed as he was transferred to a preheated ambulance with an estimated interior temperature of 25°C. Chemical heat packs were placed on his axillae and groin, along with a foil blanket and cloth blankets. In the ambulance, the infrared forehead thermometer read “Low.” Prehospital vital signs and presence or absence of shivering were not recorded.
The patient arrived at a Level 3 trauma hospital at 1650h. At 1655h, Tr was 22.9°C, measured using a Smiths Medical ER400–9 Level 1 Probe Temperature Thermistor 9FR Rectal/Esophageal Probe (Smiths Medical Inc, Minneapolis, MN), which was visually verified by the attending physician to be inserted 15cm past the external anal margin. This corresponds to a cooling rate of 10.6 °C/h. The patient was shivering on arrival. His Glasgow Coma Scale was 8 (E1, V2, M5), and he was agitated and combative. At 1702 h, the patient was given 3 mg lorazepam intravenously. The first full set of vital signs at 1715 h (while the patient was still combative) was blood pressure 120/98 mm Hg, heart rate 90 beats/min, respiratory rate 19 breaths/min, oxygen saturation 94%, and Tr 24.9°C. After the patient settled from the initial interventions, for the next hour he was in sinus bradycardia with a heart rate of 40 to 50 beats/min, and occasionally dipping into the thirties, and blood pressures around 100/60 mm Hg. While awaiting transport to a facility with extracorporeal life support capability, resuscitation was initiated with 39°C intravenous normal saline, a forced-air warming blanket (Bair Hugger, 3M, Maplewood, MN), warmed humidified high-flow nasal air (Airvo2, Fisher&Paykel Healthcare Ltd, Auckland, NZ), 1L bags of 39°C saline to the groin and axillae, and warm blankets. By 1740h, with a Tr of 28°C, the patient was able to answer basic questions. As his temperature rose, transfer to an extracorporeal life support center was put on hold due to his rapid improvement and the risks of transport. Rectal temperature increased steadily to 37.1°C at 2049h, corresponding to an overall rewarming rate of 3.6°C/h. Vital signs are shown in Figure 1. Except for the warmed intravenous fluids, which can be considered minimally invasive, there was no invasive rewarming. Shivering was observed throughout the patient’s admission until a normothermic core temperature was attained and he obtained complete neurologic recovery.
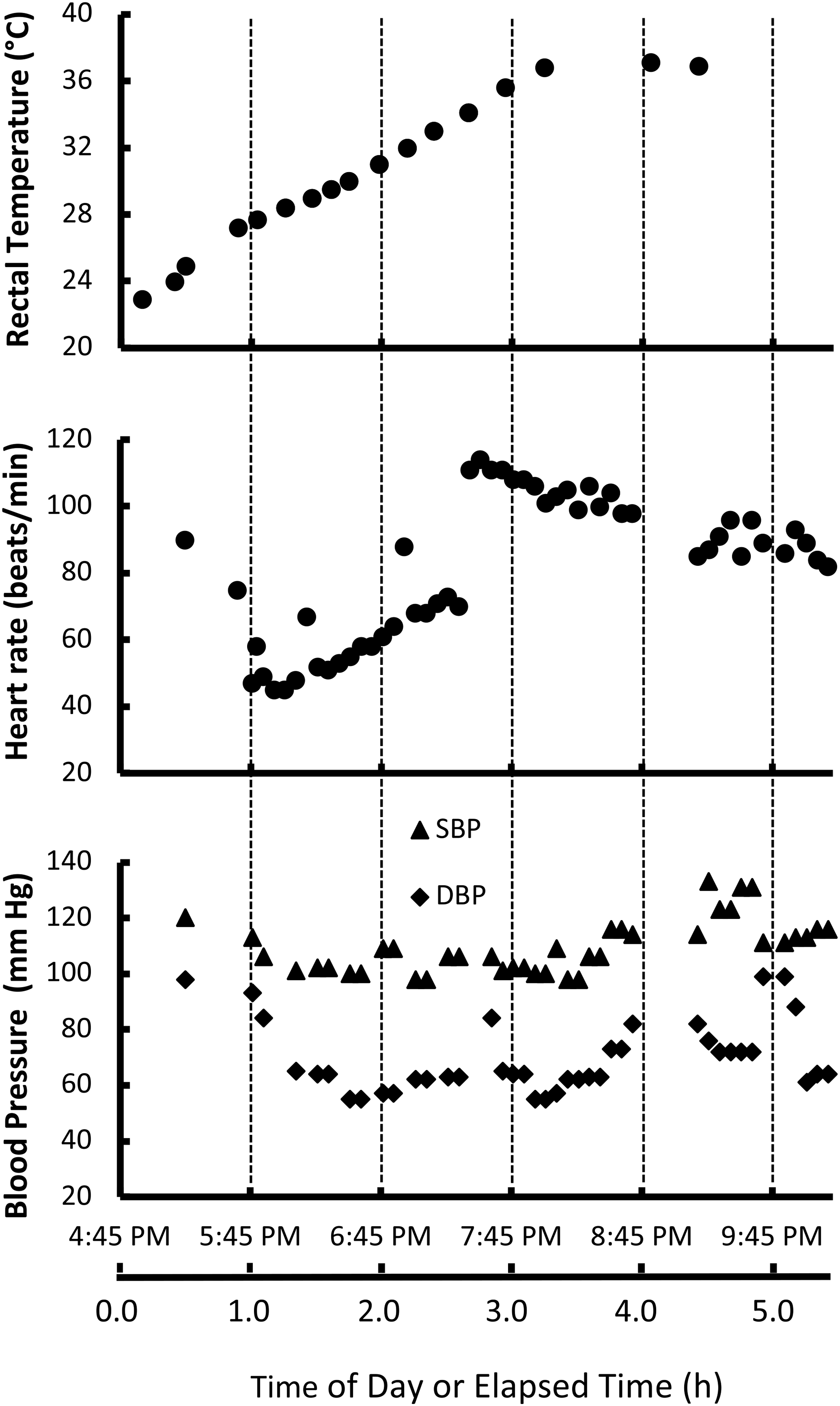
Rectal temperature, heart rate, and blood pressure during rewarming.
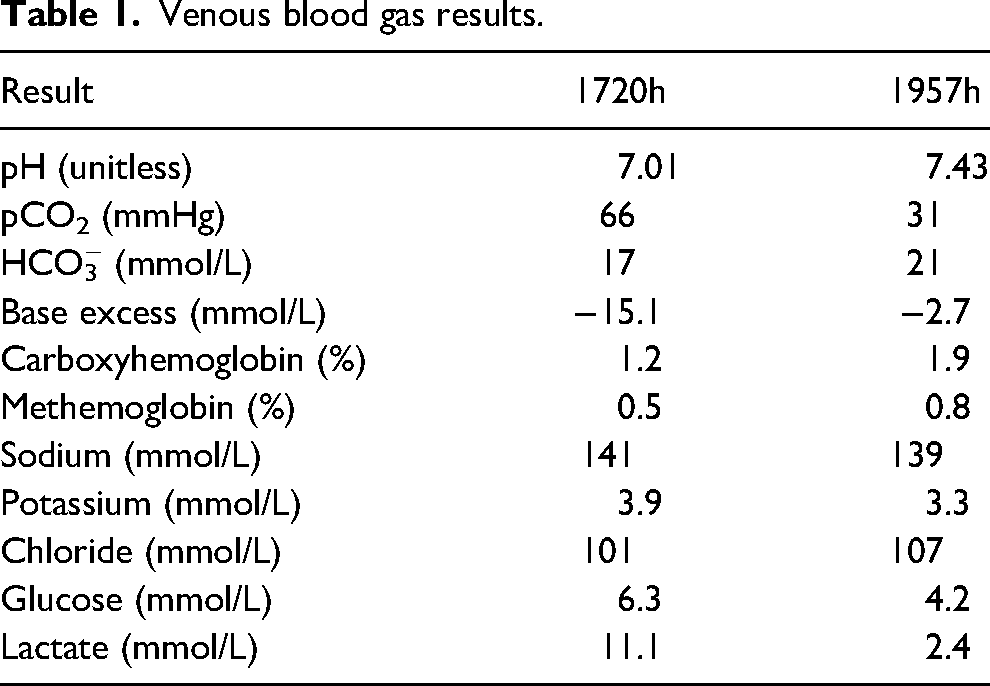
Blood was drawn at 1720 and 1957h (Table 1). A computed tomography scan of the patient’s head revealed no acute abnormalities. There were no adverse events. The patient was discharged from hospital at 2227h, less than 6h after arrival. There were no known long-term sequelae at 1 year after the event.
Venous blood gas results.
Discussion
An online search of Medline was made in July 2023 for patients with core temperatures <32°C due to cold water immersion, snow burial, and cold air exposure. Reports of patients who survived the hypothermia and included enough information to calculate a cooling rate are shown in Table 2. Case studies date back to 1967, and there were no restrictions in the search for language or year of publication.
Summary of reports between 1967 and July 2023 of 41 moderate to severe hypothermia patients who survived a core temperature of <32.0°C from any of cold air exposure, cold water immersion, or avalanche burial in which a core temperature cooling rate could be calculated.
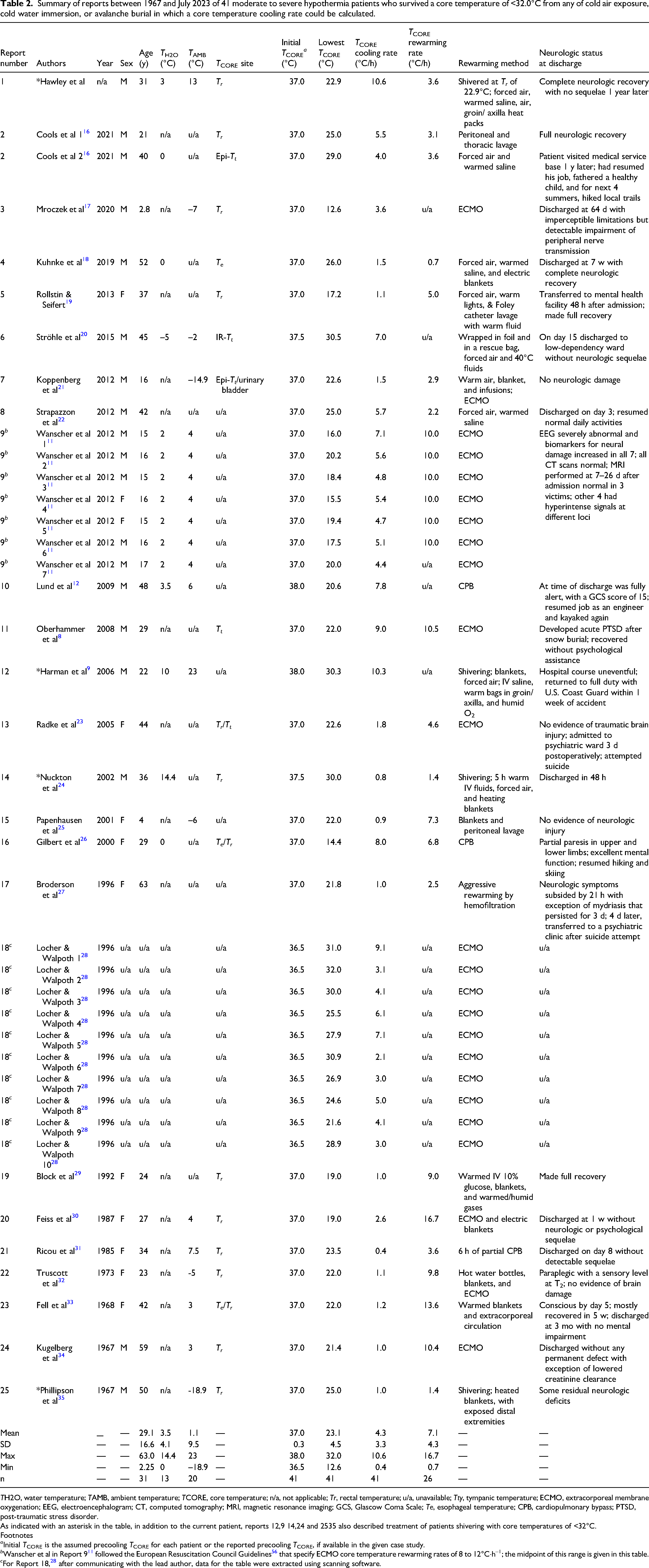
TH2O, water temperature; TAMB, ambient temperature; TCORE, core temperature; n/a, not applicable; Tr, rectal temperature; u/a, unavailable; Tty, tympanic temperature; ECMO, extracorporeal membrane oxygenation; EEG, electroencephalogram; CT, computed tomography; MRI, magnetic resonance imaging; GCS, Glascow Coma Scale; Te, esophageal temperature; CPB, cardiopulmonary bypass; PTSD, post-traumatic stress disorder.
As indicated with an asterisk in the table, in addition to the current patient, reports 12,9 14,24 and 2535 also described treatment of patients shivering with core temperatures of <32°C.
Footnotes
a Initial TCORE is the assumed precooling TCORE for each patient or the reported precooling TCORE, if available in the given case study.
b Wanscher et al in Report 9 11 followed the European Resuscitation Council Guidelines 56 that specify ECMO core temperature rewarming rates of 8 to 12°C·h–1; the midpoint of this range is given in this table.
c For Report 18, 28 after communicating with the lead author, data for the table were extracted using scanning software.
Included with the report on this patient are summaries of 41 cases in 25 papers dealing with moderate to severe hypothermia (Table 2). The first measured mean core temperature of patients (n=41) was 23.1±4.5°C (range 12.6–32.0°C), mean age (n=31) was 29.1±16.6 y (range 2.25–63 y); there were 19 males and 12 females, and for 10 patients there was no reported sex or age. Unless an initial core temperature was reported, cooling rates in Table 2 were estimated using an assumed initial core temperature with a mean value of 37.0±0.3°C (range 36.5–38.0°C, n=41) with lower values for resting and higher values for active individuals. Mean cooling rate was 4.3±3.3°C/h (range 0.4–10.6 °C/h, n=41). The patient in this study (report 1 in Table 2) cooled by 14.1°C at a rate of 10.6°C/h over 1.33h. In addition to the patient in this report, shivering was reported in only 4 other cases,9,24,35,36 with 39,24,35 of these cases of shivering at low core temperatures included in Table 2. Shivering was either absent or not documented in the other 38 of 41 cases. The rewarming rate for 26 patients treated with or without extracorporeal membrane oxygenation (Table 2) was 7.1±4.3°C/h (range 0.7–16.7°C/h), with the patient in this report having a rewarming rate of 3.6°C/h over 3.11h.
Cooling Rates
Experimental studies 5 and predictive modeling6,7 suggest that the patient in this report should have had a cooling rate of 2 to 4 °C/h. The patient, however, had a calculated cooling rate of 10.6°C/h. Many factors likely contributed to the rapid cooling rate, such as minimal insulation from a low body fat percentage and light clothing, increased peripheral blood flow from ethanol vasodilation and adrenergic-primed muscle usage, and increased conductive and convective heat loss from trying to kick the boat to shore. Although kicking would increase heat production, with minimal insulation it would appear that there would be minimal (if any) contribution to core temperature. A similar core temperature cooling rate of 10.3°C/h was reported in another patient who survived. 9 A very high core temperature cooling rate of 14°C/h also was reported recently, 14 although this patient subsequently died from accidental hypothermia.
Shivering
The presence of shivering at low core temperatures was reported in 4 other cases.9,24,35,36 The patient in this report was visibly shivering at his initial Tr of 22.9°C. Both ethanol and tetrahydrocannabinol were complicating factors in this case. Ethanol has been shown to delay the onset and magnitude of shivering, 37 as do other anesthetic or hypnotic agents, as shown in a comprehensive review on the effects of ethanol. 38 Smoking marijuana is not thought to have a significant impact on overall core temperature but may increase heat transfer from the muscles used for shivering. 39 Regardless, neither ethanol nor tetrahydrocannabinol appeared to impair the patient's shivering.
The mechanism underlying shivering at such low core and presumably even lower peripheral tissue temperatures remains enigmatic. Shivering requires significant energy expenditure.6,7,40 The patient in this case was young and physically fit, and his exposure time was relatively short. He had been consuming food and beverages and was well hydrated prior to the accident, which may have helped him maintain shivering.
Current guidelines1,41, 42 suggest failure of spontaneous shivering at core temperatures <28 to 32°C. It should be noted that these are general assumptions for most cases. In contrast, shivering has been reported in the literature (Table 2) at core temperatures of 21, 36 25, 35 30.0, 24 and 30.3°C. 9 This suggests that the utility of shivering for clinical staging of hypothermia severity should be viewed with caution. A proposed revision to the Swiss System addresses this issue but has not yet been formally validated. 42
Core Temperature Measurement
Rectal temperatures generally remain within 0.5 to 1.5°C of other sites of core temperature measurement but can be falsely low if the probe tip is not inserted by 15 cm or if it is embedded in fecal matter, and this measurement may lag behind esophageal or heart core temperature measurement during both cooling and rewarming.5,15 During the transition from cooling to warming, there is a paradoxical period that often occurs when the patient arrives at the hospital. During this period, heart temperature is increasing while rectal temperature continues to decrease. Thus, reliance on rectal temperature may falsely lead the medical provider to consider more intrusive methods than necessary. If airway management is required, consideration should be given to using esophageal temperature because it is the most accurate minimally invasive measure of heart temperature. 5
Use of Sedative Medications in Accidental Hypothermia
Hypothermic patients may be confused, uncooperative, or even combative, and sedation may be required to facilitate transport and care. The ideal sedative would maintain appropriate shivering, vasoconstriction, airway reflexes, and intrinsic heat production while rendering the patient calm and cooperative. An exhaustive literature search did not uncover data on the safety or efficacy of commonly used sedation medications such as benzodiazepines or ketamine in moderate or severe hypothermia patients. Opiates, particularly meperidine (Demerol), are used to blunt the shivering response postoperatively and during hypothermia physiology studies.43,44 In this case, it appears that a 3 mg of intravenous lorazepam was successful in calming the patient to facilitate care while maintaining shivering and airway protection.
Rescue Collapse and Consciousness
Rescue collapse, also known as circum-rescue collapse, describes a deterioration in patient condition around the time of first contact or during rescue from a dangerous or stressful environment. The spectrum ranges from physical collapse to loss of consciousness to cardiac arrest. In the present case, the patient was presumably severely hypothermic by the time of his rescue, and he transiently lost consciousness without cardiac arrest while he was being pulled from the water. Mechanisms for this phenomenon are not completely understood, but some factors include reduced adrenergic tone in response to mental relaxation, decreased venous return resulting in hypotension, and decreased core temperature.5,45 Decreased adrenergic tone reduces heart rate, total peripheral resistance, cardiac output, and blood pressure while also reducing myocardial and skeletal muscle contractility. The loss of hydrostatic pressure when a patient is removed from the water, combined with a vertical lifting position, can decrease venous return dramatically. Collectively, these factors appear to have contributed to the rescue collapse in this patient.
To decrease the risk of rescue collapse, it is important to avoid rough handling, maintain horizontal positioning as much as possible, and attempt to prevent mental relaxation until the risk of collapse is determined to be low (for example, when hypothermia is mild or the patient is rewarmed). Any rescue team should be aware that the time required for dispatch, deployment, and arrival to the scene is long enough that rescue collapse is a very real possibility as they approach the patient.
Level of consciousness in accidental hypothermia is a clinical sign often used to predict core temperature when its measurement is not available. The patient's maintenance of consciousness with a Tr as low as 22.9°C was an important “abnormal” finding. However, it may have helped predict the favorable outcome because consciousness may be a better prognosticator than core temperature. 4 Alcohol may have been a protective factor. As summarized in a comprehensive review 38 on the effects of ethanol, it is noteworthy that hypothermic patients with a moderate to high blood alcohol level have been observed to maintain consciousness at lower than expected core temperatures despite a faster cooling rate versus nonintoxicated control individuals.46–49 In addition, the patient in this report was a chronic cannabis user, which provides an increased tolerance to hypothermia. 50 as does chronic ethanol consumption. 38 For ethanol-intoxicated patients, their increased level of awareness differs from the unconscious state typically evident during profound states of hypothermia. Intoxicated patients release more heat when metabolizing ethanol from an increased proportion of lipid oxidation in skeletal muscle, which possibly contributes to their preserved mental state. 38 Although alcohol and cannabis may be advantageous in maintaining consciousness at low temperatures, their use likely increases the risk of death from accidental hypothermia due to factors mentioned previously as well as cognitive and motor impairment.
Rewarming Rates
The patient in this case rewarmed at 5.0°C/h in the first hour and subsequently at 3.1°C/h with only active external and minimally invasive measures. This gave an overall rewarming rate of 3.6°C/h. This is greater than the expected rewarming rate of up to 3.4°C/h. 15 Shivering, however, may have played a role in the patient's rewarming. Shivering can increase heat production by up to 5 times the resting metabolic rate5,40,51,52 and can raise core temperature at a rate of 3 to 4°C/h.43,52,53 Similarly, some of the patients in the reported cases demonstrated rewarming from severe or profound hypothermia with minimally invasive methods.9,16,18–20,22,24,25,29,35 Within this summary (Table 2), three other cases9,24,35 reported shivering. These cases had rewarming rates of 1.4°C/h,9,35 whereas the current patient's rewarming rate was 3.6°C/h. Similar to the current victim, who had no known sequelae at an informal 1-year follow up, each patient with shivering9,24,35 had good neurologic outcomes, as did the majority of the other patients with minimally invasive rewarming methods.
Limitations and Future Research
A possible limitation for this case report is a reporting bias. Cases of moderate to severe hypothermia that follow the guidelines are often not published and therefore would not be included in our literature search. Another limitation is the possibility of inaccuracy in the reported core temperature. Accurate measurement of core temperature in the most appropriate and safest way possible is a constant challenge in real clinical scenarios, especially in a prehospital environment or at smaller centers, including this hospital, with limited resources. Only rectal core temperature measurement was available in this case, and core temperature measurement can vary significantly from site to site. 54 Although studies5,55 of therapeutic hypothermia indicate that rectal temperatures are usually within 0.5 to 1°C of pulmonary artery temperatures, data from severely hypothermic patients or those who cooled rapidly are lacking. Accurate core temperature measurement is difficult and has many limitations. Management should not necessarily be guided by core temperature measurement or classifications systems alone but by a careful consideration of the clinical syndrome and response to treatment.
Further study focused on improving the prehospital triage, classification, and management of patients with accidental hypothermia have the potential to decrease the morbidity and mortality associated with this common environmental illness. The patient in this report would be classified as Hypothermia Stage 1 or 2 based on both the original Swiss System and the Revised Swiss System. The patient would be classified as Moderate by the Wilderness Medical Society Classification based on clinical features. Neither of these classifications based on clinical presentation accurately reflected his core temperature. While the current accidental hypothermia staging systems will apply to most patients, outliers and evidence to the contrary should be reviewed, and other factors potentially could be considered in future updates to the staging systems, including, but not limited to, the rate or mechanism of core temperature cooling.
Conclusions
The patient presented in this case report had preserved consciousness and shivering with a Tr as low as 22.9°C. This case report and similar reports from the literature should be considered in the currently employed staging systems for accidental hypothermia. On rare occasions, consciousness, close to normal vital signs, and shivering can be preserved in patients with moderate to severe hypothermia. Core temperatures can drop more rapidly than expected, and these levels of hypothermia cannot be excluded in awake patients, particularly if they are immersed in very cold water. Last, accurate core temperature measurement is difficult in real-life scenarios, and outliers do exist. Management should not necessarily be guided by core temperature measurement or classification systems alone but rather by careful consideration of the entire clinical picture and response to treatment.
Footnotes
Author Contribution(s)
Consent
The patient in this study gave written informed consent for its publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.