
Abstract
Introduction
Pain management for trauma in the extreme environment is vital for both casualty comfort and aiding safe extrication. However, adequate pain management in a resource-limited environment can be challenging and is often limited. We conducted a scoping review of the use of regional anesthesia in the prehospital environment, evaluating which regional anesthetic procedure was performed for various indications, their efficacy, and the type of healthcare provider delivering the anesthetic.
Methods
A PRISMA-guided systematic literature review was conducted of Medline, Embase, and Cochrane databases for studies reporting the use of regional anesthesia in the prehospital environment published before June 30, 2022.
Results
Thirty studies met the criteria and were included in the review. The most common types of regional anesthesia were fascia-iliaca compartment block (n = 317, from 12 studies) and femoral nerve block (n = 210, from 8 studies), along with various other blocks for a range of indications. These blocks had good efficacy and a low-risk profile and could be delivered by a wide range of healthcare providers.
Conclusions
Regional anesthesia is an effective and non-resource-heavy pain management tool in prehospital environments, which may be applicable to austere settings. It can cover a wide range of injuries and can avoid systemic complications for casualties that may already be challenging to manage in out-of-hospital settings. Additionally, regional anesthesia can be effectively delivered by a wide range of providers. This review provides a holistic summary of pain management using regional anesthesia in the prehospital environment, with a discussion on its potential use in more extreme settings.
Introduction
Remote or extreme environments are places where access to advanced medical care can be difficult and challenging. 1 In these environments, the responsibility for dealing with injury and illness lies with the individuals present, who may have varying clinical backgrounds; from lay people with first aid training to enhanced prehospital clinicians. This type of medical practice can be described as expedition or wilderness medicine. Over the past centuries, expeditions have developed from hazardous voyages seeking new countries to claim to the enormous industry of adventure travel, as well as scientific research trips, military missions, and more. Despite the improvements in equipment safety, communication methodology, weather forecasting, and rescue services, the hazardous and unpredictable nature of the natural world remains, and despite preparation and understanding, trauma in extreme environments still occurs. Trauma is the most common presentation in extreme environments that require urgent care. The Royal Geographic Society study in 2000 found that in 246 expeditions with 2381 participants, 5.9% developed orthopedic injuries. 2
With reduced access to advanced care, adequate pain management for trauma in wilderness or remote environments is incredibly important but clinically challenging. An injured casualty will not only require adequate pain control for their primary trauma, but will frequently require evacuation, which may compound the need for anesthesia. Without good analgesic control, extrication to advanced care may become more hazardous or even impossible without casualty cooperation.
Often, the approach to pain management of trauma consists of simple pharmacological analgesics, for example paracetamol in combination with immobilization or splinting or wrapping of any injured extremity. In patients where these methods are not able to achieve sufficient pain relief, systemic opioids are commonly used in addition, if available. 3
Systemic opioids can not only have unwanted side effects for the patients, such as dizziness, nausea, and vomiting, but they can also have adverse physiological effects, such as hypotension and respiratory depression leading to hypoxemia. They can, therefore, worsen outcomes in trauma. 4 This can also create complications in the extrication process that may make it more hazardous. Additionally, depending on location, obtaining and transporting controlled drugs, including opioids, can be challenging and may lead to complications if this is not taken into account.
Here, peripheral nerve blocks can provide an alternative approach to pain management. Peripheral nerve blocks involve the direct injection of anesthetic agents to block nerves supplying the particular area of injury. These techniques are widely used in managing intra- and postoperative pain. 5 They can provide fast and long-lasting pain relief to the extremities without the potential side effects of a systemic medication.
Since limb injuries account for over half of the injuries (lower limb 27%, upper limb 25%) in the wilderness, peripheral nerve blocks have the potential to be valuable techniques to consider for pain relief and management. 6 The use of regional anesthesia in extreme environments is not a novel idea; digital nerve blocks, hematoma blocks, fascia iliaca compartment blocks (FICB), axillary nerve blocks, and spinal anesthesia are described in the Oxford Handbook of Expedition and Wilderness Medicine (2015). However, it is unclear to what extent and efficacy these blocks or other regional anesthetic techniques have been utilized by prehospital clinicians. This review will explore which types of regional anesthesia have been carried out in extreme environments, by whom, and to what effect.
Methods
A scoping review was conducted based on the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines.
Eligibility Criteria for Inclusion
All studies included examined the use of regional anesthesia in an out-of-hospital environment. Studies focusing on regional anesthesia delivered in hospitals to be utilized during interhospital transfers were excluded. All studies that met these criteria, including case reports, were included. Studies in languages other than English were translated into English for analysis. There were no date restrictions applied. The scope of the search was widened to include all studies in the prehospital setting, and not just specifically the extreme environment setting, due to the paucity of literature within the extreme environment, with the aim of attaining transferable findings for the extreme environment.
Primary and Secondary Outcomes
The primary outcome was to establish which regional blocks have been conducted in the prehospital environment. Secondary outcomes were the qualifications of those conducting regional blocks, the safety profile, and the efficacy of regional blocks conducted.
Search Strategy
A systematic literature search was conducted on EMBASE (Ovid), Medline (Ovid), and the Cochrane Library of controlled studies on June 30, 2022. The search strategy is described in online Appendix 1. All identified papers were collected in an Excel spreadsheet, and the duplicates were removed. Two reviewers (NA and LP) screened all papers by title and abstract independently. Papers deemed relevant from this screen were then assessed for inclusion by reading the full text. Any discrepancies were solved by consensus with a third reviewer (SB). This search was supplemented through hand-searching citations and reference lists from relevant articles.
Data Collection
The following details were entered into a standardized spreadsheet: author, study type, number of patients, type of regional block, qualification of the provider, number of adverse outcomes, and efficacy of the block performed.
Results
The initial database search identified a total of 5293 papers (Figure 1), and 634 duplicates were removed. The remaining 4659 articles were screened by two independent reviewers who excluded 4540 articles. After a full text assessment, another 90 articles were excluded. One paper was added from referenced studies, resulting in a total of 30 papers for inclusion in the final analysis (Table 1). Of those 30 studies, only 3 were conducted in a true austere environment.
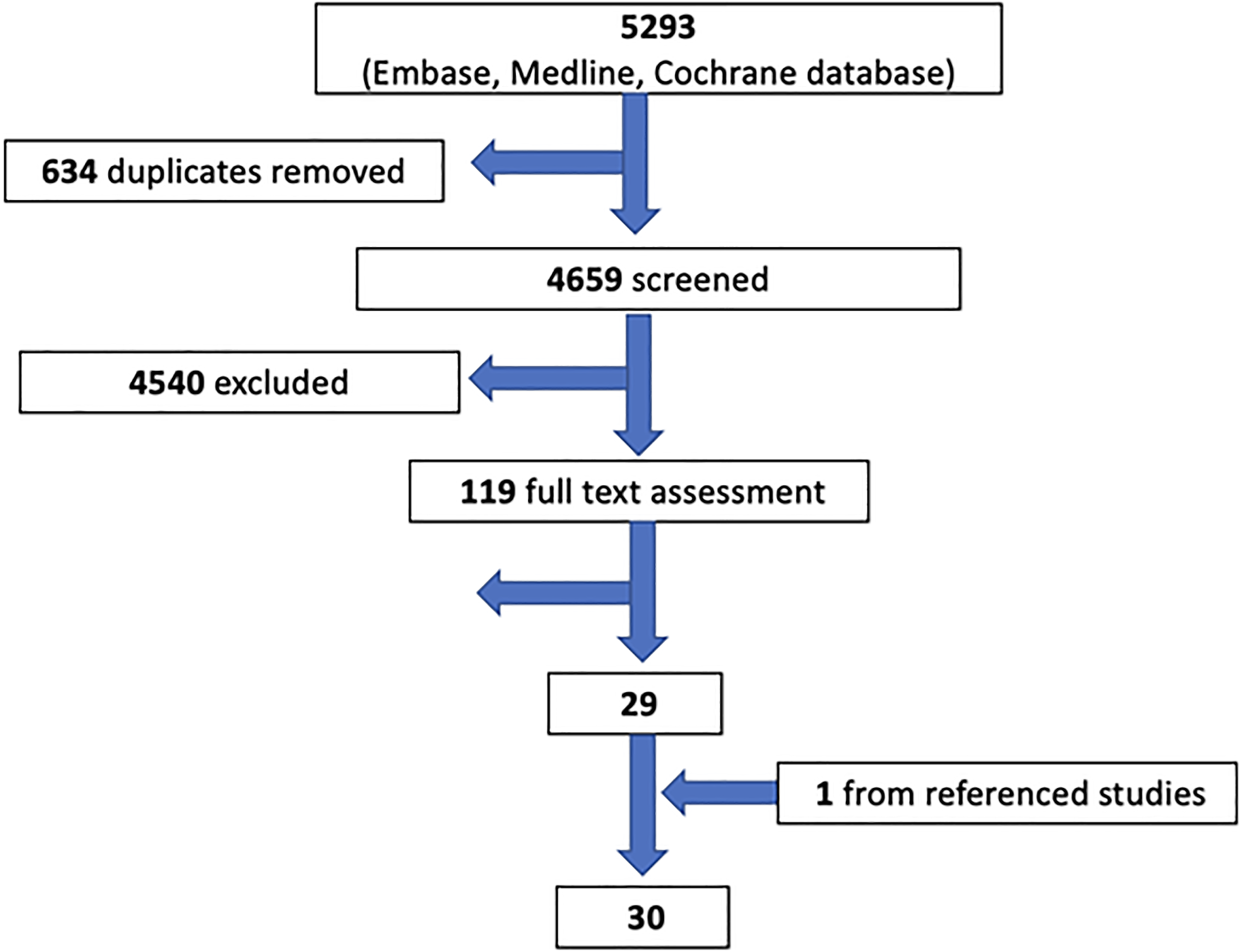
PRISMA chart.
Study Characteristics
We identified 7 randomized controlled trials, 2 systematic reviews, 5 observational studies, 10 case reports/series, 4 pilot studies, 1 qualitative study, and a single letter to the editor. A total of 583 regional anesthetic blocks conducted in the out-of-hospital setting have been documented in the literature. The most common was the fascia iliaca block (FICB), with 317 documented cases.
Provider
There is a wide range of prehospital clinicians carrying out regional anesthesia in an out-of-hospital setting, including physicians, paramedics, and nurses. Physicians were providers in 19 studies, nurses in 1 study, paramedics in 6 studies, and 1 article discussed the potential for regional anesthesia provision by astronauts. The remaining studies did not specify a provider. The type of physician delivering the blocks varied, with anesthesiologists, emergency physicians, and primary care physicians all documented as having performed regional anesthesia. No studies compared the outcomes for different providers. However, adverse outcomes and efficacy were consistent among different providers.
Techniques
For the application of regional anesthesia, a spectrum of techniques can be utilized. From the publications identified, 14 studies used a landmark-based approach, 5 studies used nerve stimulation, and 3 studies applied a combination of landmark and nerve stimulation. In 7 studies, the technique was not specified. While routinely used in the hospital, just one study indicated the use of ultrasound for the application of regional anesthesia in a prehospital setting.
Local Anesthetics
While there is a broad spectrum of different local anesthetics available, Lidocaine was the most used (16 studies). Levo-Bupivacaine was used in 3 studies and Ropivacaine in 2. Bupivacaine, Prilocaine, and Mepivacaine were each used in one publication. Four studies failed to declare what local anesthetic was used. Of those studies declaring which local anesthetic was used, no study used a local anesthetic from the Esters group.
Type of Blocks
Eight different regional blocks (Figure 2) have been described in the literature as being performed safely in the pre-hospital setting.
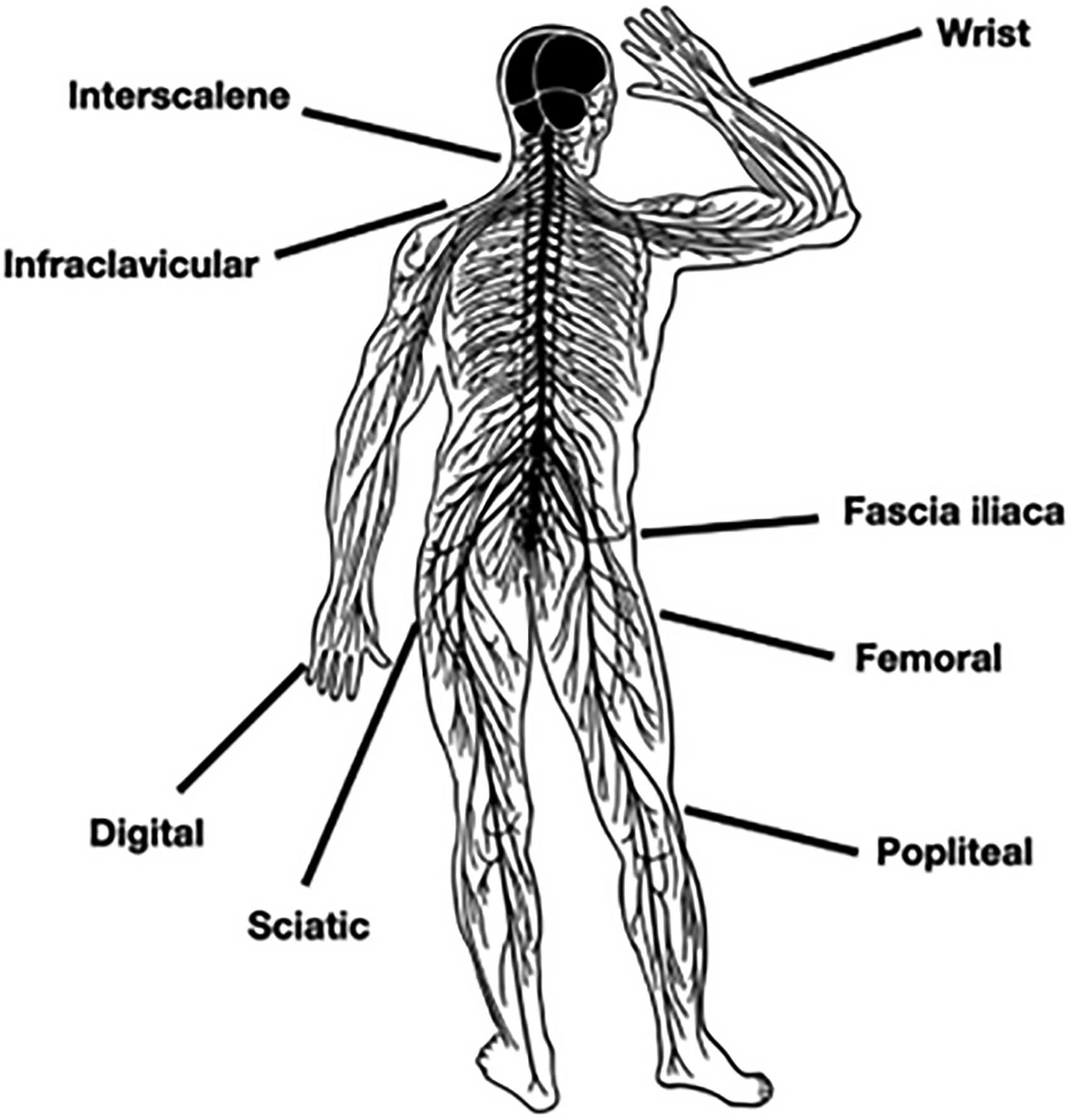
A range of regional anesthetic blocks performed in the prehospital setting (picture by NA).
Upper Extremity
Five different types of upper extremity blocks have been successfully performed out of hospital. The interscalene block (8 cases) is the most well-documented, with only single reports of wrist blocks, digital nerve blocks, and infraclavicular blocks.
Lower Extremity
Four lower extremity regional blocks have been described in the prehospital literature, with the most prevalent being the fascia iliaca block for proximal femur fractures (317 cases). Other regional blocks described are the femoral nerve (210 cases), sciatic nerve (24 cases), and popliteal nerve block (1 case).
Summary of Outcomes
Adverse Events
While there were a small number of studies reporting mild adverse events, like transient headache or self-limiting tachycardia, there was no study reporting severe side effects like infection, nerve damage, or local anesthetic toxicity. 7
Success Rate
The definition of success and what constituted a significant reduction in pain scores was very heterogeneous. Most studies defined success as a reduction in a chosen pain score, such as a verbal numerical pain score (VNPS) or a visual analog scale (VAS), often recording pain scores at fixed time intervals post-procedure. Failure of treatment was a rarity, with most studies quoting success rates greater than 90%, with success being defined as a reduction in a pain-scoring system.
Efficacy versus Systemic Analgesics
Regional blocks were shown in multiple studies to be more effective than intravenous analgesia alone, defined by reductions in pain scores. Paramedics utilizing a FICB in addition to morphine had a greater reduction in VNPS of 50% versus a 20% reduction when utilizing morphine alone. 8 Peripheral nerve blocks have been demonstrated to be more efficacious than the use of systemic analgesia and sedation in facilitating joint relocation in the out-of-hospital setting. 9
Discussion
Regional Anesthesia Can Cover a Wide Range of Injuries
The clinician working in the austere environment may encounter a range of injuries depending upon the environment and types of activities taking place. Approximately 90% of injuries encountered in wilderness and mountain activities affect the extremities, including soft tissue injuries and bony fractures. 10 While fractures are not the most common extremity injuries encountered in wilderness expeditions, they have the highest likelihood of requiring evacuation. 11 Regional anesthesia is well suited to managing fractures, with numerous types of regional block having previously been performed outside a hospital setting. Pain from femoral bone fractures (occurring from high-energy trauma such as a fall from height) can be managed with the use of fascia iliaca compartment blocks and femoral nerve blocks. Both have been previously conducted in prehospital environments.8,12 Joint dislocations can account for significant pain following trauma in wilderness settings, and nerve blocks have been shown to safely facilitate finger dislocation reduction and to provide effective analgesia for glenohumeral joint dislocations.9,13,14
Both leisure and work can result in humans operating in extremes of cold temperatures. Cold environments risk the potential of cold injuries, including frostbite. Frostbite injuries are most likely to affect the extremities and are, therefore, a good target for regional anesthesia. 15 Bilateral wrist blocks have been utilized by medics operating in remote regions to achieve complete analgesic control to facilitate the painful rewarming process, which is vital to increase the chances of tissue viability. 16
Soft tissue injuries are the most common type of extremity injuries for which regional blocks are also beneficial. 11 Quadriceps tendon ruptures can occur from a fall and have been effectively controlled with the use of an iliofascial block in the prehospital environment. 17
Impalement injuries have also been managed with regional blocks, in one case using an iliofascial block performed on the mountainside for a patient with a large, deep quadriceps wound resulting from a fir branch. 18
Additionally, local anesthetic agents may be useful for various procedures aside from regional anesthesia, including wound suturing and dental work. The ability to cover a wide range of extremity injuries with regional anesthesia makes it a useful addition to a practitioner's kit when working in resource-limited environments.
Non-Resource-Heavy
Working in an austere environment poses challenges with regard to the weight and amount of equipment one can carry, particularly if not on a vehicle-bound expedition. Therefore, the ideal analgesic in such environments should require minimal equipment. There are several methods of delivering regional anesthesia, with varying amounts of equipment required. Blocks are often classified as landmarks and ultrasound-guided techniques. They can also be categorized by whether they utilize a nerve stimulator or not. The most resource-sparse methods and, therefore, most suited to austere environments are the landmarked, non-nerve-stimulator approaches. However, with the growing potential use of ultrasound within wilderness medicine, an ultrasound probe may be a standard part of an advanced practitioner’s kit already. 19 The increase in portability of ultrasound machines additionally means this will become less of a barrier to ultrasound-guided blocks.
A variety of local anesthetics can be used to provide analgesia, all with different onset times and half-lives. Lidocaine, bupivacaine, and ropivacaine have all been used within the out-of-hospital setting.16,20 Local anesthetics have also been shown to still be effective at lower temperatures, with slight delays in onset times but no significant difference in duration of action. 21 While there are inconclusive data about the analgesic effect provided by warmed local anesthetics, there is limited information about the impact on the action time. 22 To ensure best clinical performance, local anesthetics should be stored and applied around room temperature, avoiding extreme temperature changes.
Basic requirements for a regional anesthesia block are small, lightweight, and would be easy to carry on long expeditions (Figure 3).
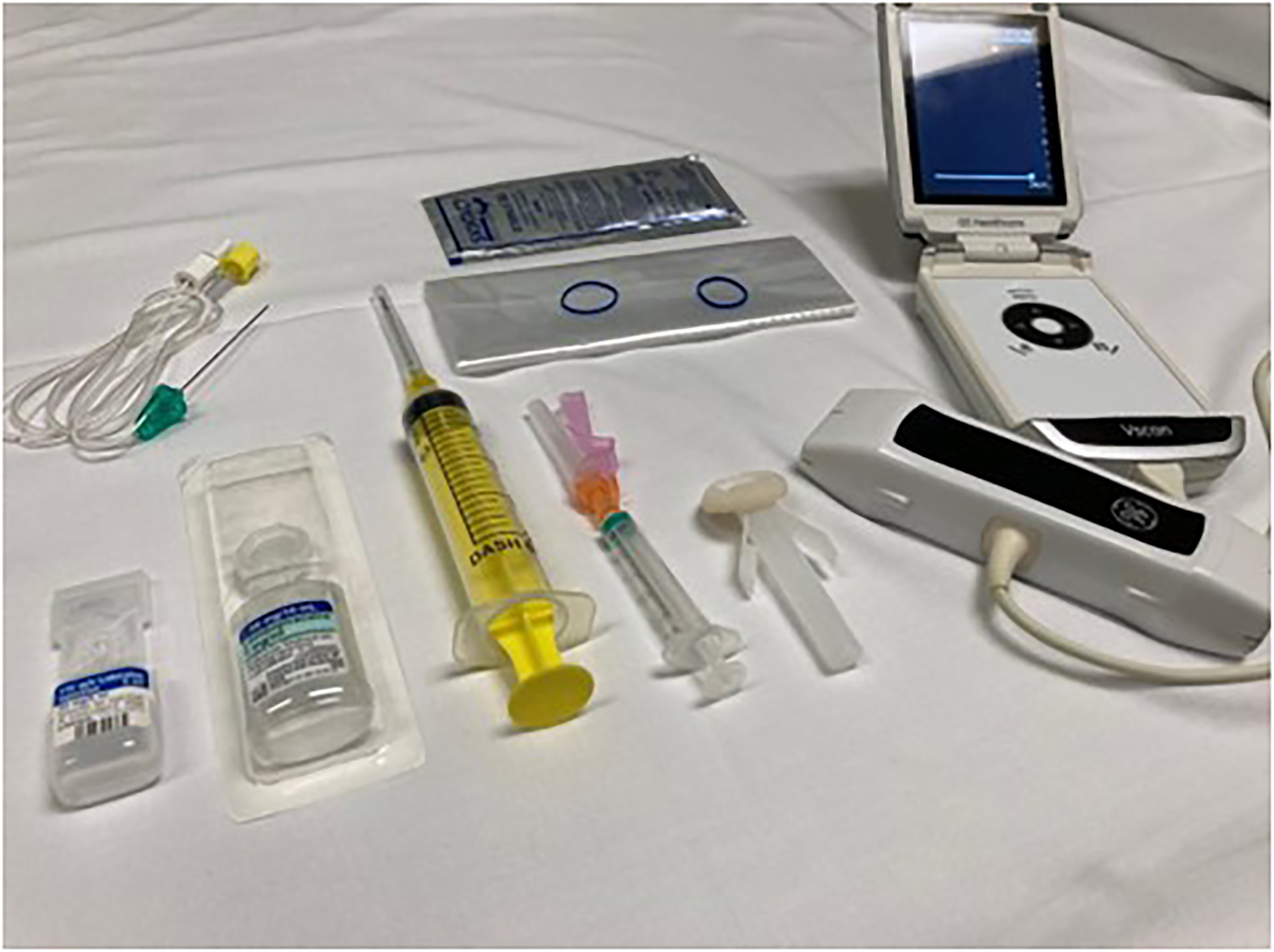
Basic equipment required to deliver a regional anesthetic block. Included are a local anesthetic agent (both short and long-acting), needle, syringe, and skin cleaner (optional ultrasound, probe cover, and nerve stimulator needle). Not pictured is a sharps bin and gloves. Items removed from sterile packaging and not on sterile field for demonstrative purposes (picture by NA).
Regional Anesthesia Can Be Delivered by a Range of Providers
There are numerous providers of wilderness and expedition medicine, including doctors, nurses, paramedics, and nonhealthcare professionals with first aid qualifications. 23 This spectrum of providers must be taken into account when evaluating potential new methods of analgesia for the austere environment. Historically, regional anesthesia has been delivered to hospitals by anesthesiologists; however, regional anesthesia has now been adopted into nursing and paramedic practice with success. Emergency medical service nurses in Europe have safely delivered fascia iliaca blocks. 24 Their training involved a theoretical element followed by procedural practice on cadavers with a final assessment before being signed off. These nurses went on to perform 100 blocks with no complications and effective pain reduction in 96% of cases. A group of paramedics in New South Wales, Australia, have been trained to safely perform fascia iliaca blocks utilizing a self-directed learning package. 8 They received a one-day training with an anesthesiologist, which included simulations. Some may have concerns regarding the scope of practice for providers carrying out regional anesthesia who are not accustomed to utilizing it regularly in their day job; however, there is supporting evidence that with formal training, fascia iliaca blocks can be safely delivered in the out-of-hospital setting. Emergency physicians have also safely and effectively delivered a range of regional blocks in the prehospital setting, including interscalene, infraclavicular, sciatic, and femoral nerve blocks. 25 Subsequently, there is sufficient evidence that this form of analgesia has the potential to be used within the field of wilderness and expedition medicine by nonanesthesiologist physicians. Regional anesthesia may offer benefits over systemic analgesia in treacherous environments. There are numerous resources available for clinicians to deepen their understanding of regional anesthetic blocks.26–28
One of the challenges of delivering analgesia in an austere environment is that patients may be required to assist with their own evacuation, continuing to be part of their expedition team to ensure their own and others' ongoing safety. For this reason, there are significant downsides to the use of more traditional systemic analgesics. Opioids are a mainstay of pain management but have numerous side effects, including reduced consciousness, respiratory depression, hypotension, and vomiting. 29 These side effects could significantly impede a patient's ability to safely assist with extrication from a wilderness environment, as well as the possibility of leading to hypoxemia and worsened clinical outcomes. This risk does not apply to regional analgesic blocks. Simple analgesia such as paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDs) can allow a degree of pain relief for mild to moderate injuries; however, in an extreme environment in which a casualty may be already dehydrated and facing a prolonged evacuation, NSAIDs may further exacerbate any acute kidney injury. 30 Regional anesthesia could possibly be limb-saving if pharmacological analgesia is ineffective, for example, in a fracture-dislocation with occlusion of blood supply. Here, effective pain control might contribute to a more effective reduction and restoration of blood flow.
Regional Anesthesia Can Be Conducted Safely in a Prehospital Environment
Despite best efforts, working in an extreme environment can rarely offer the same sterility and cleanliness offered by in-hospital practice. One complication of regional anesthesia is postprocedural infection. When basic infection control precautions are taken for single-injection nerve blocks in hospitals, the occurrence of postprocedure infections is extremely low. 31 Follow-up on patients who underwent prehospital regional anesthesia has shown very low infection rates, suggesting noninferiority to hospital practice.32,33 It remains unclear if the low infection rates in a prehospital environment are transferable to a true austere environment. Local anesthetic toxicity, while rare, is challenging to manage in a remote situation. Clinicians should be aware of the symptoms and signs of overdose, ranging from mild (perioral paresthesia, tinnitus, metallic taste) to severe (fits, coma, hypotension, dysrhythmias, and cardiac arrest). The risks and benefits to the patient should always be assessed before commencing a regional anesthesia block, and any block should be carried out by a trained practitioner with awareness of the safe dosage of the local anesthetic agent to be used (Table 1).
Different types of regional blocks conducted in the prehospital setting.
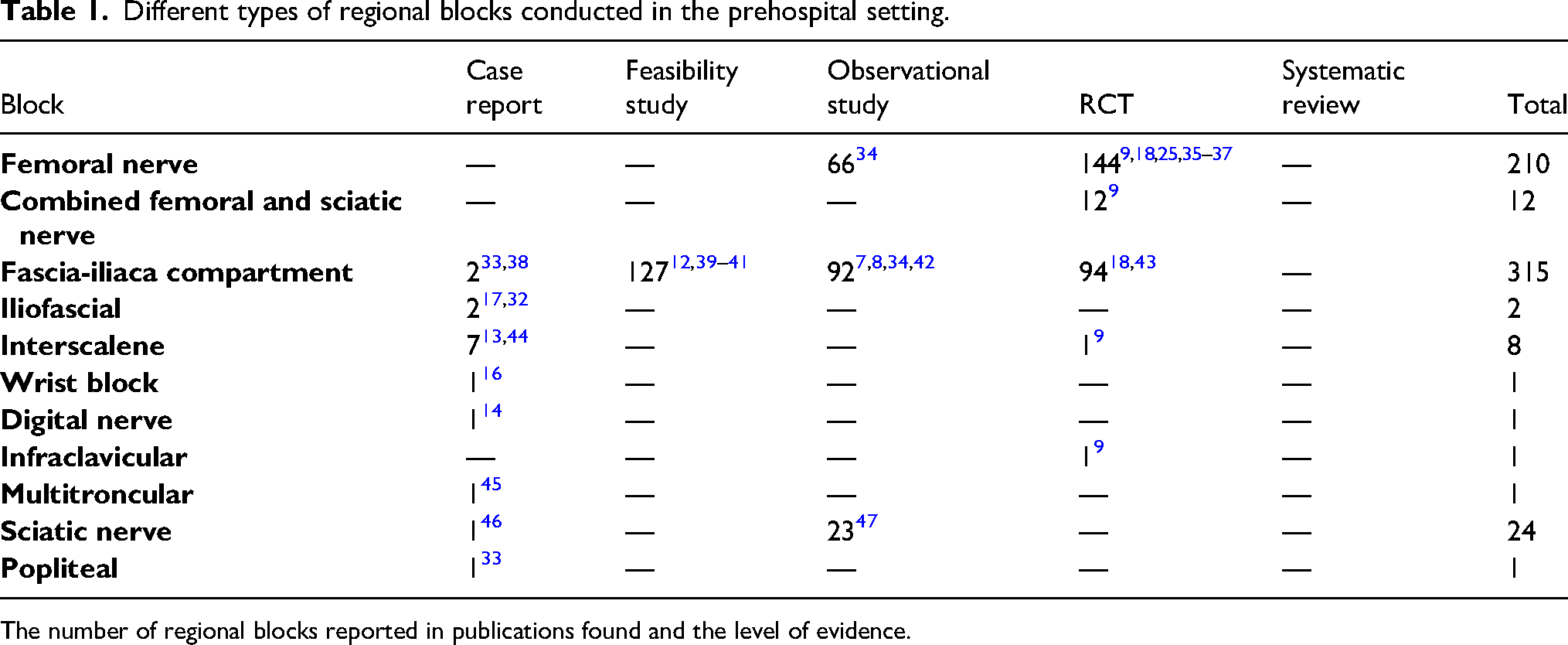
The number of regional blocks reported in publications found and the level of evidence.
Emerging Use of Ultrasound in the Austere Environment - Role in Regional Anesthesia?
Due to advanced technology, ultrasound (US) has become more and more available in prehospital settings over recent years. Small devices like the Butterfly IQ might reasonably find their way into the backpack of expedition medics. While prehospital point-of-care ultrasound (POCUS) is normally used to identify life-threatening conditions (eg, cardiac tamponade, abdominal bleeding), it can also help support the application of a peripheral nerve block.
Limitations
There was significant heterogeneity in methodologies utilized among the studies included and the definitions used to quantify a successful regional block. Comparisons made between systemic analgesics and regional anesthetic blocks were not always applicable to standard practice, with intravenous NSAIDs being utilized rather than intravenous opioids. Therefore, results may not be applicable to individual systems.
Most of the evidence base derives from case reports and series, with limited randomized controlled trials. Despite all studies reporting on regional blocks conducted outside of a hospital setting, it was not well documented exactly what type of prehospital environments these were. Of those that had clearly documented locations, not all were conducted in an austere environment, with many taking place in urban environments.
Conclusions
This review suggests regional anesthesia to be a safe and effective option for pain management of trauma in a prehospital environment. It has been shown to be effective in a range of prehospital settings with a level of nonsterility and can be delivered by a wide range of healthcare providers with varying levels of clinical training. There is limited data in austere settings, but our findings suggest regional anesthesia may also be efficacious in a wilderness environment. Due to a lack of evidence on the use of regional anesthesia, specifically in extreme environments, there is a need for further research to determine the safety and efficacy in these settings.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Appendix
Search strategy.
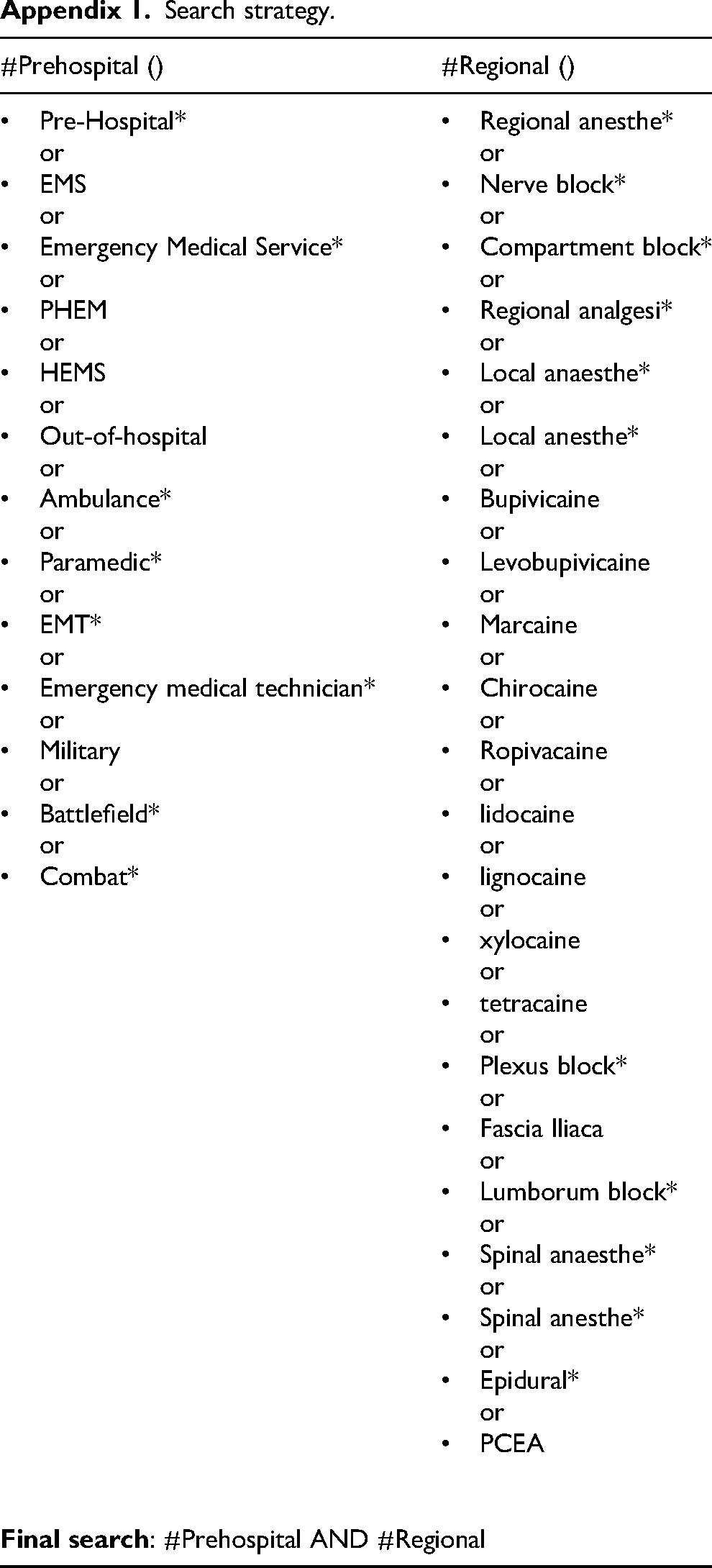
| #Prehospital () | #Regional () |
|---|---|
|
Pre-Hospital* or EMS or Emergency Medical Service* or PHEM or HEMS or Out-of-hospital or Ambulance* or Paramedic* or EMT* or Emergency medical technician* or Military or Battlefield* or Combat* |
Regional anesthe* or Nerve block* or Compartment block* or Regional analgesi* or Local anaesthe* or Local anesthe* or Bupivicaine or Levobupivicaine or Marcaine or Chirocaine or Ropivacaine or lidocaine or lignocaine or xylocaine or tetracaine or Plexus block* or Fascia Iliaca or Lumborum block* or Spinal anaesthe* or Spinal anesthe* or Epidural* or PCEA |