
Abstract
The Wilderness Medical Society convened a panel to review available evidence supporting practices for acute management of drowning in out-of-hospital and emergency care settings. Literature about definitions and terminology, epidemiology, rescue, resuscitation, acute clinical management, disposition, and drowning prevention was reviewed. The panel graded available evidence supporting practices according to the American College of Chest Physicians criteria and then made recommendations based on that evidence. Recommendations were based on the panel's collective clinical experience and judgment when published evidence was lacking. This is the second update to the original practice guidelines published in 2016 and updated in 2019.
Introduction
Approximately 236,000 deaths globally are attributed to drowning every year, although this number is believed to underestimate the true number. 1 Drowning particularly affects young persons and can have profound personal, emotional, and financial consequences for patients, families, and society. The goal of these practice guidelines is to reduce the burden of drowning through improvements in treatment and prevention. We present accepted drowning terminology as part of a review and evaluation of literature regarding acute care for drowning patients in both out-of-hospital and emergency medical care settings, with a particular focus on the wilderness context. The authors relied upon the experience and knowledge of a panel of wilderness and emergency medicine practitioners to make recommendations where little or uncertain evidence was available. This is the second update of these guidelines. The original guidelines were published in 2016, and they were first updated in 2019.2,3
Methods
The authors of this update reviewed each section of the original document to determine the relevance and need for updating. Articles published between 2018 and 2022 were identified through PubMed, MEDLINE, and Google Scholar using a keyword search appropriate to each topic. Randomized controlled trials, observational studies, case series, and review articles were reviewed and evidence assessed. Abstracts for which the full article could not be obtained were excluded. If no relevant studies were identified, recommendations were based on the panel's clinical experience and judgment. Recommendations were graded using the updated 2018 American College of Chest Physicians classification scheme, which is consistent with all other Wilderness Medical Society Clinical Practice Guidelines beginning in 2023 4 (see Supplemental File).
Terminology
The standard definition for drowning, according to the World Congress on Drowning in 2002, is “the process of experiencing respiratory impairment due to submersion or immersion in liquid.” 2 Inspired by the Utstein Style for reporting cardiac arrest data, the standard definition allows for only 3 outcomes after drowning: nonfatal drowning (with or without morbidity) and fatal drowning. This definition is based on the understanding that “respiratory impairment occurs as the person's airway goes below the surface of the liquid (submersion) or water splashes over the face (immersion).” 5 However, the inclusion of both submersion and immersion in this definition may cause confusion with the large body of work on survival and rescue related specifically to cold water immersion, which focuses more on hypothermia than on drowning. For the purposes of these guidelines, which could include cold water conditions, a further distinction is necessary. “Immersion” refers to a situation in which the airway is above water, whereas “submersion” refers to a situation in which the airway is underwater. Thus, immersion in cold water may lead to hypothermia (and only drowning if there is sufficient airway exposure through splashes), and submersion at any water temperature may lead to drowning. The following modifiers should not be used in association with drowning: near, wet, dry, active, passive, saltwater, freshwater, or secondary. Sufficient data related to human drowning pathophysiology show that none of these modifiers is valid because the final common pathway is hypoxemia and eventual cardiopulmonary arrest and because their definitions are vague and sometimes erroneously linked to any type of drowning at all.2,5–7 By understanding and using the standard definition for drowning and abstaining from using incorrect terminology, communication among medical practitioners, data collection entities, researchers, and policymakers has become more consistent. Accurate communication better reflects the true incidence, prevalence, and sequelae of drowning and should improve clinical dialogue and management as well as promote a correct understanding of drowning and its management in the public—critically important in this condition that must often initially be managed by bystanders.7–9
Epidemiology
The highest-risk age group for drowning worldwide is children 1 to 4 y old, primarily owing to unintentional falls into water; the next highest-risk group is adolescents and young adults in natural bodies of water. In the United States, there were, on average, 4012 drowning deaths per year from 2005 to 2014, plus an additional 658 boating-related deaths. 10 In 2021, 81% of which were from drowning. 11 Although the incidence of drowning has been gradually decreasing over time, drowning remains the leading cause of injury-related death for children aged 1 to 4 y. More than 90% of the world's drowning deaths occur in low- and middle-income countries where reporting systems are underdeveloped and significantly understate the true occurrence. 1 In the context of low- and middle-income countries, natural sources of water are often ubiquitous and lack barriers to entry. They are used for transportation, cleaning, food, and hydration. Based on the World Health Organization and Centers for Disease Control and Prevention systems for classifying drowning statistics, these numbers exclude deaths from homicide, suicide, and those occurring during transport, floods, storms, and other natural disasters. In 2010, there were 12,900 emergency department (ED) visits in the United States for drowning, with 20% of patients admitted to the hospital. Drowning deaths were 48% more likely to occur on weekends compared to weekdays. Fifty-three percent of all male and 26% of all female drowning deaths occurred in natural bodies of water. 10
The burden of drowning in high-income countries is underreported because most studies only address the issue of fatal drowning. In the United States, there were an average of 8061 estimated emergency department visits due to nonfatal drowning each year between 2011–2022. 12 Internationally, the burden of nonfatal drowning is more difficult to estimate because many patients may not present to an emergency medical system or hospital, where data collection typically occurs.10,13,14 In Bangladesh, a large population-based study showed fatal and nonfatal drowning rates of 15.8 per 100,000 and 318.4 per 100,000, respectively, compared to 1.17 per 100,000 and 10 per 100,000 in the United States.15,16 Risk factors for nonfatal drowning are similar to those for fatal drowning.15,17–21
Rescue of the Drowning Patient
Reaching the Patient
Rescuer safety is paramount during rescue operations; in the aquatic environment, specific skills, training, and physical capabilities are required. The physical characteristics of aquatic environments vary widely, ranging from pools to lakes, rivers, oceans, swift river water, and ice scenarios, among others, each requiring different sets of equipment and training for technical rescue. Few studies objectively measure the effectiveness of in-water rescue techniques. Much of the literature on this topic is based on the experiences and policies of the writers or organizational authorities. There is a high prevalence of fatal and nonfatal drowning of untrained persons attempting to perform in-water rescues, with 1 study reporting 114 rescuer deaths during a 3-y period in Turkey alone.22–24 Hazardous water conditions that led to the initial person drowning often persist and place the well-intentioned rescuer at risk of becoming an additional drowning patient. 25 Rescue by untrained persons should be attempted without entering hazardous conditions by reaching out to the drowning patient with a paddle or branch; throwing a rope, buoy, cooler, or any floating object; or rowing a boat, canoe, or paddleboard to the patient. Trained rescue personnel should operate according to their level of training, expertise, equipment, and comfort level. Entering the water to perform a rescue should be attempted only by persons with specific training to operate in that dangerous environment. Few studies have been conducted on the effectiveness of different water safety devices (eg, rescue tubes, rescue cans, throw bags, life rings), but what has been demonstrated is that proper and effective use of these devices requires basic knowledge of their function combined with regular practice. 26
Patients in Submerged Vehicles
Death from entrapment and drowning in submerged vehicles is often not classified as a drowning death, confounding attempts to accurately track the epidemiology of this type of drowning. 27 Studies suggest that 10% of drowning deaths may be due to entrapment in submerged vehicles, especially during disasters, and that in the case of inland flooding, as many as 10% of motor vehicle crashes result in a drowning death.28–31 There is a small body of medical and rescue literature on the topic of vehicle submersions.29,32–37 A formal review of educational and public service information identified “three probable significant contributors to [the] high fatality rate [of drowning in submerged vehicles]: 1) ‘authorities’ provide an inadequate description of vehicle sinking characteristics; 2) contradictory and inadequate advice is often provided; and 3) a poor public perception of how to escape.” 32 Several sources recommend questionable escape practices without supporting evidence. These practices include allowing the passenger compartment to fill with water so that it will be easier to open doors, waiting until the vehicle sinks to the bottom of a body of water to maintain orientation, relying on kicking out the windshield or opening doors after the vehicle has fully sunk, and relying on breathing trapped air in the passenger compartment. In a formal survey, more than half of the general public identified an option that involves staying in a vehicle while it sinks to the bottom as being the safest option when trapped in a submerging vehicle; this advice often appears in the popular media. 36 Research data derived from 35 vehicle submersions conducted in diverse locations and seasons suggest this advice is erroneous. The best time to escape from a submerging vehicle is immediately during the initial floating phase, ideally during the initial 30 s to 2 min after water entry when most vehicles remain partially above the surface. 36 An algorithm, using the acronym SWOC, has been developed to advise those entrapped in water how to sequence escape actions. The SWOC algorithm recommends the following sequencing of actions before mobile phone use: Seatbelts off, Window open (upstream window), Out immediately, Children first. 37 The available research points out that electric windows should work if engaged quickly; if necessary, windows should be broken before water rises high enough to push against them; children should be helped from the oldest to youngest and before adults.38,39 The rationale for evacuating from oldest to youngest is that older children are more likely to be able to follow instructions to exit the vehicle and hold on or quickly be helped out of the vehicle, allowing the adult to focus on the other children. If starting with the youngest first, it is likely that the adult would not be able to help the other children if they had to assist other children while holding an infant. If the vehicle is in moving water, recommendations are to open the upstream window for egress, which will only be possible if the water level is below the level of the window. The rationale behind this is that if one attempts to exit through the downstream window, it increases the likelihood of being swept away by a strong current. Therefore, exiting via the upstream window would increase the chance that the victim could climb on top of the roof to await rescue. In 2008, Priority Dispatch, a US-based proprietary out-of-hospital emergency medical dispatcher system added an addendum to its standardized protocols that instructed emergency medical dispatchers not to persist in getting a location for a caller in a submerging vehicle. Instead, it recommends that a caller exit the vehicle immediately if it is submerging—before using precious time to determine location—and using the SWOC protocol.38,40 In 2010, the International Academies of Emergency Dispatch (IAED) began work on revising their sinking vehicle protocol; in 2013, they approved a new protocol shifting dispatcher priorities from establishing location to first instructing victims on how to self-rescue and escape the vehicle before it sinks.38,39 An additional protocol was developed in 2013 to address the subset of patients drowning in floodwaters. Differences here include the survival benefit in floodwaters to a vehicle not floating (vs survival benefit to vehicles floating in deeper water), the possibility of using a door, and specific recommendations to get on the roof after exiting rather than into the water.38,39
In-Water Resuscitation
The primary physiologic insult in a drowning patient is cerebral hypoxia; its rapid reversal is the primary objective of drowning resuscitation. For the purpose of these guidelines, in-water resuscitation (IWR) is defined as an attempt to provide ventilation to a drowning patient who is still in the water. This does not apply to chest compressions. It is impossible to perform adequate chest compressions while the victim and rescuer are in the water, and so they should not be attempted. 41 Successful use of IWR was first described in 1976, with a mannequin-based feasibility study reported in 1980; however, the first clinical study to show a positive patient outcome was not published until 2004.42–44
Available outcome data for IWR are based on a single retrospective analysis of lifeguard rescues in Brazil and show significant improvement in survival and neurologic outcome in persons receiving IWR. These rescues were performed by trained, professional lifeguards in the ocean environment. Lifeguards would frequently tow the patient beyond breaking waves and perform mouth-to-mouth ventilations while awaiting helicopter pickup. 44 Subsequent studies, primarily using mannequins, evaluated the ease of performing this task in controlled aquatic environments and found that IWR increases overall rescue time, subjective rescue difficulty, number of submersions, and water aspiration.45,46 A single study comparing lifeguards to lay rescuers when using IWR found that lifeguards showed improved rescue times and decreased estimated pulmonary aspiration. 47 A scoping review was conducted that showed limited evidence, but a formal recommendation is forthcoming from the International Liaison Committee on Resuscitation. IWR may be considered in situations where a trained rescuer determines that the rescuer's safety, equipment available, and distance to shore warrant its use, with the understanding that rescuers should maintain their own safety and stop at any time. 48
Similarly, there are no studies directly measuring patient outcomes when CPR is performed in boats, but there are numerous studies that show it is feasible.48–53 We recommend that CPR with or without chest compressions can be performed in a moving boat if sufficiently safe for the rescuers. Rescuer safety and prevention of communicable diseases are of utmost importance, so consideration should be given to the use of barrier devices during IWR. Food and Drug Administration–approved, IWR-specific devices are available that use a self-purging mechanical one-way valve instead of the paper valve on standard CPR masks.54,55
Initial Resuscitation
Cardiopulmonary Resuscitation and Prioritization of Airway
Because of the central role of hypoxemia in the pathophysiology of drowning, initial resuscitation should focus on establishing and maintaining a patent airway and providing oxygen at the highest concentration available, which may include positive pressure ventilations. Recent updates to cardiopulmonary resuscitation (CPR) algorithms, specifically for the lay rescuer, include recommendations for compression-only CPR and prioritization of compressions before airway maneuvers.56,57 Compression-only CPR is likely to be of little to no benefit in drowning resuscitation, and its use should be limited to bystanders not trained to provide full (rescue breath and compression) CPR. Bystander CPR for infants and children includes compressions and ventilations, regardless of which is started first. Professional rescuer CPR should emphasize prioritization of airway and breathing with positive pressure ventilation before initiation of chest compressions. If the airway is overlooked in initial resuscitation, ongoing hypoxemia leads to decreased survival and worse neurologic outcomes. Incorrect administration of rescue breaths can delay care and cause gastric insufflation and pulmonary aspiration. For persons who are not trained, able, and/or willing to give rescue breaths, compression-only CPR is still the recommended method of resuscitation. All persons who might respond to a drowning person (eg, parents, trip leaders, lifeguards) should take CPR classes that include training on the proper use of chest compressions and rescue breathing.
Oxygenation
Few large-scale studies have evaluated the use of different airway adjuncts for resuscitating drowning patients. Although ideal rescue breathing includes supplemental oxygen and a positive pressure delivery device, any amount of oxygen delivery (eg, mouth-to-mouth, bag-valve-mask [BVM] with ambient air) is better than none if supplemental oxygen is not available. Mannequin studies of supraglottic airways have shown that lifeguards can successfully insert them, but there is concern that this does not replicate real-world usage.58,59 Additional concern is that because of pulmonary edema from drowning, certain supraglottic airway devices may perform poorly for oxygenation based on leak pressures.60,61 If the supraglottic airway fails to achieve adequate chest rise, a BVM or other method to oxygenate and ventilate the patient should be used. BVM usage is a complex task that is difficult to perform correctly, even with regular training. Those with a duty to act should use a BVM only if it is part of a competency-based training program with regular retraining and maintenance of equipment. Otherwise, mouth-to-mouth or mouth-to-mask should be considered. 62
Automated External Defibrillator
Although cerebral hypoxia is the primary cause of morbidity in the drowning patient, hypoxic myocardial injury is also likely to occur with prolonged hypoxemia. Typically, drowning patients initially experience sinus tachycardia, followed by bradycardia, pulseless electrical activity, and then asystole, owing to the hypoxic nature of the event. 63 In drowning patients, ventricular fibrillation (VF) is rare, occurring in less than 10% of patients; thus, reversal of hypoxemia with ventilations and compressions should not be delayed in an attempt to apply an automated external defibrillator (AED).63–69 Once resuscitation is established, early application of an AED might be beneficial, given the possibility of VF as the cause or result of drowning. In the drowning patient, if global myocardial hypoxia persists, attempts at defibrillation may be unsuccessful without concomitant oxygenation and ventilation. Experimental animal models have shown that as long as AED pads are placed firmly on a patient's chest and a rescuer is not in direct contact with that patient, the use of an AED in a wet environment does not pose an increased risk to the patient or rescuers.70–72 AEDs have been tested and noted to correctly detect simulated arrhythmias and deliver shocks on moving boats. 73
Abdominal Thrusts
Drowning involves water obstructing the airway and causing cerebral hypoxia; in some cases, small amounts of water are aspirated into the lungs. This can cause atelectasis, direct cellular injury, and pulmonary edema. Even after unconsciousness, reflex swallowing of water from the hypopharynx into the stomach may occur. Dr Henry Heimlich advocated use of abdominal thrusts in initial treatment of the drowning patient, claiming that aspirated water must first be cleared from the airway to allow proper ventilations.74–76 In the 30 y since his original report, concern has been raised about this recommendation, resulting in an Institute of Medicine report and a systematic literature review by the American Red Cross.77,78 All of these investigations failed to identify quality data to support use of the Heimlich maneuver before providing ventilations. Its use during initial resuscitation delays delivery of ventilations and prolongs hypoxemia. 77 In drowning resuscitation, the upper airway is frequently occluded by water or vomit, which should be cleared by standard suction techniques, not abdominal thrusts. If the drowning was precipitated by choking on food or a solid object, or if the airway is occluded by a solid object that is preventing ventilation, then the standard guidance for clearing foreign body airway obstruction applies, which may include abdominal thrusts/back blows if they are conscious or chest compressions if unconscious.
Cervical Spine Precautions
Recent discussions and research in the field of out-of-hospital medicine have brought to question the utility, safety, and clinical benefit of what once was called routine spine immobilization. The most current published review of this topic specific to austere environments is the Wilderness Medical Society Clinical Practice Guidelines for Spinal Cord Protection: 2019 Update. 79 We recommend reviewing the updated guidelines for current evidence on the utility of this procedure.
Retrospective studies of drowning patients found the incidence of cervical spine injuries was low (0.5% to 5%) and that most injuries were related to diving from a height. In patients without obvious signs of trauma or a known fall or diving event, the risk of spine injury is low.80,81 Another recent study further suggests that patients with no history to suggest axial spine loading are at exceptionally low risk of cervical spine injury. 82 In patients without this specific traumatic mechanism, treatment maneuvers focused on restricting spine motion may distract rescuers from the critical role of oxygenation and ventilation.
Hypothermia
Water is thermally neutral at approximately 33°C (91°F). Because most patients drown in water at a lower temperature than this, concomitant hypothermia is not uncommon. 28 The main physiologic problem with drowning is brain hypoxia. Current practice suggests that the brain can withstand longer periods of hypoxia if the body is cooler than the normal physiologic range. On one hand, leaving a patient moderately cool, or warming them to a moderately cool degree, could be beneficial or at least innocuous. On the other hand, moderate-to-severe hypothermia should be corrected, with the understanding that warming may be operationally difficult in some drowning situations. Beyond initiation of basic warming measures, the details of hypothermia treatment, including augmented advanced life support measures, are beyond the scope of these guidelines. Readers are encouraged to review the most current version of the Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia. 83
Postresuscitation Management
Oxygenation/Ventilation
Mechanical Ventilation
No literature is available comparing out-of-hospital or in-hospital mechanical ventilation (MV) strategies for the drowning patient. Current practice recommends a lung protective ventilation (LPV) strategy similar to that used for patients with acute respiratory distress syndrome (ARDS), on the premise that the lung injury pattern after drowning is similar.5,84,85 This includes MV starting with a tidal volume (VT) of 6 to 8 mL/kg−1, augmentation of VT and respiratory rate to maintain plateau pressure < 30 mm Hg, and augmentation of positive-end expiratory pressure and fraction of inspired oxygen (FIO2) to maintain partial pressure of arterial oxygen (PaO2) at 55 to 80 mm Hg (SpO2 89–95%). 86 As many patients who require MV also suffer from hypoxic cerebral injuries, it is difficult to determine the value of MV alone for survival. 87
Noninvasive Positive Pressure Ventilation
Noninvasive positive pressure ventilation (NIPPV) has been used successfully in the out-of-hospital setting. There are case reports describing its successful use in drowning.88–91 Similar to MV, the addition of airway pressure to prevent atelectasis and support respiratory muscle use while preventing hypoxemia can be achieved with NIPPV. However, NIPPV can only be used in spontaneously breathing patients and should be used with caution in the drowning patient with altered mental status because there may be an increased risk of vomiting and aspiration. Drowning patients who have mild to moderate hypoxemia and are being treated in out-of-hospital and emergency medical systems using NIPPV might benefit from this therapy. One small retrospective study showed similar neurologic outcomes and correction of hypoxemia and acidosis between patients treated with early endotracheal intubation versus NIPPV after drowning; in addition, patients receiving NIPPV had a lower incidence of infection and decreased hospital and intensive care unit length of stay. 92 This study also showed similar levels of oxygenation and correction of hypoxemia with MV and NIPPV; the limiting factor in use of NIPPV remains the patient's mental status and ability to cooperate with the intervention. 92
Diagnostics
Radiologic Testing
Several retrospective ED studies of drowning patients found that the initial chest radiograph did not correlate with arterial blood gas levels, outcome, or disposition.93–95 A study of admitted drowning patients showed that those who went on to develop acute lung injury or ARDS had abnormal chest radiograph findings within the first few hours but not necessarily on arrival to the ED. 84 Head computed tomography (CT) has been studied in an attempt to quantify anoxic brain injury in drowning patients. Retrospective studies have found that patients with abnormal initial CT all went on to develop severe brain injury or die, whereas initially normal head CT had no prognostic value. 96
Laboratory Testing
Canine studies performed in the 1960s showed clinically significant hemodilution and red blood cell lysis associated with salt, chlorine, and freshwater drowning.97–99 These studies were based on instilling up to 44 mL/kg−1 of fluid into the trachea of anesthetized dogs, far greater than the 1 to 3 mL/kg−1 typically aspirated by human drowning patients. Electrolyte abnormalities and hemodilution only occurred in dogs that had 11 mL/kg−1 or more instilled. No studies have identified clinically significant electrolyte or hematologic abnormalities in drowning patients that help guide initial therapy or provide prognostic information. In patients with altered mental status or decreased level of consciousness, laboratory evaluation for alternative causes that might have led to the drowning event, such as hypoglycemia or intoxication, can be helpful. Arterial blood gas analysis in symptomatic patients can be used to help guide respiratory resuscitation.
Other Treatments
Antibiotics
Although microorganisms present in aspirated water may eventually cause pneumonia, no study to date has shown benefit from empiric administration of antibiotics in drowning patients. This is in part because microorganisms found in drowning-associated pneumonia are atypical bacteria or fungi and often are resistant to standard empiric treatments.100–102 Aspiration of even small volumes of water can produce abnormalities on chest radiograph that can mimic pneumonia. The psychological trauma of the drowning event and hypoxemia can cause leukocytosis from stress demargination as well as fever from inflammation and irritation caused by water in the airways, making it difficult to differentiate inflammatory from infectious pneumonitis. 103 The decision to administer antibiotics should be made after initial resuscitation and ideally be based on expectorated sputum or endotracheal aspirate bacterial culture, blood cultures, or urinary antigen tests.100–102 Because these tests are not available in the wilderness setting, treatment should be initiated for symptoms consistent with pulmonary infection (eg, fever, increased sputum, abnormal lung auscultation) that continue after initial resuscitation and treatment phases.
Corticosteroids
Corticosteroids were historically used in drowning patients to facilitate pulmonary recovery and surfactant production. However, there is not sufficient evidence to support empiric corticosteroid administration for drowning patients. 104
Targeted Temperature Management
Mild therapeutic hypothermia (TH) has been shown to decrease cerebral oxygen utilization and improve neurologically intact survival in patients with witnessed VF cardiac arrest. 85 There has been more recent evidence that suggests there may be no difference in neurologically intact survival in out-of-hospital cardiac arrest between normothermia and mild TH, and this is an area of active investigation. 105 Current American Heart Association/International Liaison Committee on Resuscitation guidelines recommend targeted temperature management (TTM) for adults after cardiac arrest, at a temperature between 32 and 34°C (90 to 93°F) for at least 24 h. 106 Many institutions have extrapolated these data to include non-VF causes of cardiac arrest.
The 2002 World Congress on Drowning provided a consensus statement recommending TH of 32 to 34°C for patients achieving return of spontaneous circulation (ROSC) after cardiac arrest due to drowning. 107 Our literature search yielded multiple case reports and retrospective reviews supporting neurologically intact survival in hypothermic patients, but several older studies showed no benefit.108–120 There is no prospective study comparing TTM to normothermia after ROSC in drowning patients. There might be benefit to discontinuing rewarming interventions after a hypothermic drowning patient has reached TTM temperature range, but this has been insufficiently studied to support an evidence-based recommendation.
Disposition in the Wilderness
Ceasing Water-based Rescue and Resuscitation Efforts
The care of drowning patients in the wilderness can range from a small group of untrained bystanders/volunteers to a highly trained search-and-rescue team with extensive resources. In the wilderness setting, available resources, risk to rescuers, and team/volunteer safety must be considered when deciding how long to search for a submerged patient. Although each drowning episode has unique patient and environmental factors, the most important predictor of outcome is the duration of submersion.69,121,122 Available evidence shows that prognosis is poor with submersion times greater than 30 min, regardless of water temperature. 123 There are case reports of survival with good neurologic outcomes despite prolonged submersion—predominantly young children (around 6 y old) in water < 6°C (43°F) and with the use of advanced treatment modalities, such as extracorporeal membrane oxygenation.124–129 There are also case studies of patients in cardiac arrest, also young, having full neurological recovery after CPR for more than 90 min. 130 These cases are considered exceptional. For the purpose of these guidelines, recommendations are based on available evidence relevant to a typical drowning patient and on the probability of neurologically intact survival in specific conditions. A literature review of 43 cases serves as the evidence for water-based rescue. 131 The report concludes that there is minimal chance of neurologically intact survival with a submersion time of more than 30 min in water warmer than 6°C (43◦F) or more than 90 min in water that is colder than 6°C (43°F). It is important to note that “submersion time” was defined as beginning upon arrival of emergency services personnel; total submersion time is often unknown.
If a drowning patient is removed from the water and resuscitation takes place, it might be necessary to decide when to cease resuscitation efforts if no signs of life return. Based primarily on retrospective studies, submersion times of >10 min appear to correlate with increased mortality or survival with severe neurologic dysfunction.69,122,132 In addition, more than 25 min of resuscitation or prolonged time to advanced medical care also correlates with negative outcomes but without the statistical significance of submersion time. In a Dutch retrospective review of 160 hypothermic drowning patients under the age of 16 y, 98 children received CPR for more than 30 min, with only 11 surviving to discharge, all of whom were neurologically devastated.123,132–134
Based on resources, we suggest cessation of rescue and transition to body recovery operations when there is a known submersion time of greater than 30 min in water warmer than 6°C (43°F), or longer than 90 min in water < 6◦C (43°F). Cessation of resuscitation is recommended after 30 min of continuous cardiopulmonary resuscitation. If at any point during search-and-rescue efforts the safety of the rescue team becomes unacceptably threatened, we recommend rescue efforts be ceased. If resources are available and recovery team activities are appropriately safe, we suggest body recovery efforts continue beyond the search-and-rescue period with the understanding that resuscitation attempts will likely be futile.
Strong recommendation, low-quality evidence.
Decision to Evacuate
If a victim survives a drowning event in the wilderness, objective physical examination findings may assist in the decision to evacuate the victim to advanced medical care. A single large retrospective study of nearly 42,000 ocean lifeguard rescues serves as the primary evidence for on-scene decision-making. 135 This study found that victims who experienced a drowning event but had no symptoms other than mild cough and who did not have abnormal lung sounds had 0% mortality(Grade 0, 1; Table 1). As symptoms worsened and victims developed abnormal lung sounds (Grades 2, 3), mortality increased. Hypotension (systolic blood pressure < 90 mm Hg or mean arterial pressure < 60 mm Hg) accounted for the next-largest increase in mortality (Grade 4). In a retrospective study of children who experienced nonfatal drowning, any clinical deterioration occurred within the first 4 h in victims presenting with mild symptoms and Glasgow Coma Scale score 13 or above. 93 These findings are similar to those from another retrospective study of pediatric victims in which new symptom development after arrival to the hospital occurred within 4.5 h in all but 1 victim; the 1 outlier developed symptoms in 7 h and had a good outcome. 93 Additional recent emergency department studies are discussed in the Disposition in Emergency Department section of these guidelines. These studies had similar results—clinical decompensation, if present, occurred in the first few hours of observation. 136
Out-of-hospital management and classification of drowning patients.
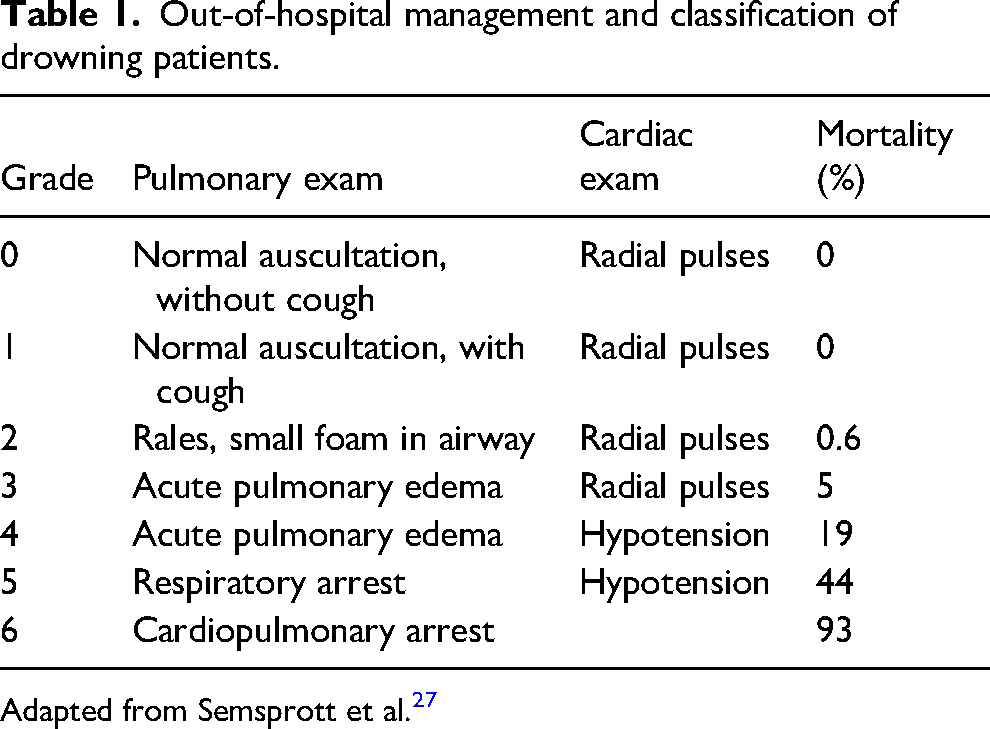
Adapted from Semsprott et al. 27
We recommend immediate evacuation to advanced medical care if risks of evacuation do not outweigh potential benefits for any victim with abnormal lung sounds, severe cough, frothy sputum, foamy material in the airway, depressed mentation, or hypotension. We suggest considering release from the scene any victim who is asymptomatic (other than a mild cough) and displays normal lung auscultation. Ideally, another individual should be with them for the next 4 to 6 h to monitor for symptom development or the victim should be advised to seek medical assistance if symptoms develop. We suggest observation of victims with mild symptoms and normal mentation for 4 to 6 h in the event that evacuation is difficult or may compromise the overall expedition. Any evidence of decompensation warrants prompt evacuation if the risks of evacuation do not outweigh the potential benefit. If evacuation of a mildly symptomatic victim has begun and the victim becomes asymptomatic for 4 to 6 h, we suggest cancelling further evacuation and continuing previous activity.
Strong recommendation, low-quality evidence.
Disposition in the Emergency Department
Although many studies have addressed prognostic factors for neurologic survival at hospital discharge, only a few have addressed the question of which patients can be safely discharged from the ED. The first, a prospective study of primarily pediatric patients, included follow-up phone interviews with 33 patients who were either released on the scene or discharged from the ED within 1 to 6 h of arrival and found that none of these patients experienced delayed effects. 137 A retrospective review of 48 pediatric drowning patients who presented to a single ED with Glasgow Coma Scale score 13 or above studied whether factors predicting safe ED discharge could be identified. 93 Initial chest radiograph did not correlate with severity of disease, and all patients who deteriorated did so within 4 h of ED arrival. The authors concluded that patients could be safely discharged home if normalized and if there was no deterioration in respiratory function after 4 to 6 h of observation in the ED. A retrospective review of hospitalized pediatric patients found that in all patients who were initially asymptomatic but who went on to develop symptoms during their stay, these symptoms developed within 4.5 h in all but 1 patient and did so within 7 h in the final patient. 138 In the 6 y preceding this current guideline update, 4 more pertinent retrospective studies investigating safe discharge of pediatrics patients were published.95,139–141 The findings of these articles are in line with the aforementioned studies in that patients who initially presented as normal or with minimal symptoms, with normal mentation, and with no need for airway support generally could be safely discharged. Patients in this group who had a clinical decline did so within the first few hours and had subsequent safe discharge. One of the studies derived and validated a clinical score to assist in determining which patients may be safely discharged after 8 h of ED observation. The study found that the presence of 4 or more of the following factors predicted safe discharge: normal mentation, normal respiratory rate, absence of dyspnea, absence of need for airway support, and absence of hypotension. 140
Prevention
Prevention has the potential to save far more lives than rescue or treatment of drowning persons. A comprehensive prevention program includes participant screening for medical diseases that increase the risk of drowning, demonstrated ability to swim, use of safety devices, and use of safe practices when in and around water.
Participant Screening
Retrospective studies have linked coronary artery disease, prolonged QT syndrome, autism, and seizure disorders with higher-than-normal rates of drowning and drowning deaths.64,142–148 Preparticipation screening should focus on uncovering any medical or physical condition that may potentially impair decision-making, physical ability, and thus swimming ability in the event of drowning. These include a history of spontaneous syncope, exertional syncope, and a family history of sudden cardiac death. There remains no reliable screening tool for the evaluation of cardiac conduction disorders, but screening electrocardiogram and family history of sudden cardiac death can help clinicians differentiate which patients might benefit from further evaluation or genetic testing if indicated.
Swimming Ability
Common sense dictates that an individual who is a competent swimmer and has the neurocognitive ability to make appropriate decisions about water safety has a decreased likelihood of drowning. However, the best ages to learn technique and specific swimming skills that reduce a person's chance of drowning are not well established. Most literature evaluates infant and pediatric populations for the effects of swimming and infant survival lessons on drowning and mortality.136,149 There is concern that by providing swim lessons to young children, parents may develop a false sense of security in their child's swimming ability, which might lead to increased drowning incidents.150–152
The American Academy of Pediatrics has always maintained that children should learn to swim at some point in their lives. Currently, they recommend that most children over the age of 1 y will benefit from swim lessons, but those under 1 y are unlikely to benefit as they are developmentally unable to learn the complex movements required.136,153 Children typically develop the motor skills to swim by ages 2–4 y and most are developmentally able to swim at age 4.5 y. Most children can master the front crawl by 5–6 y old. 149
There is considerable debate regarding the definition of “swimming” or “survival-swimming” and what constitutes the most protective approach to swim instruction. Although the ability to swim farther distances can be perceived as increased swim ability, for the purpose of swimming as a tool for drowning prevention, the distance of 25 m (82 ft) has been adopted by international lifesaving agencies and a large population-based study in Bangladesh.154,155 Despite the lack of definitive evidence showing clear benefit to formal swim lessons, panel members agree that familiarity with and, more importantly, confidence in an aquatic environment would be beneficial in the event of accidental immersion or submersion. In addition, unique aquatic environments, such as whitewater, should be approached only after focused instruction on swimming techniques specific to that environment.
Personal Flotation Devices
Personal flotation devices include lifejackets, manually or automated inflation systems, and neoprene wetsuits, among others. Currently, lifejackets are the only devices with injury prevention data available and will, therefore, be used as the prototypical model for this category. In 2019, according to the US Coast Guard, there were 613 boating-related deaths—79% due to drowning. 10 In 86% of the cases due to drowning, no life jacket was worn. Three other retrospective studies have found an association between life-jacket use and decreased mortality in boating accidents.156–158 One of these studies compared drowning deaths before and after increased life-jacket regulations, revealing improved survival rates after regulations went into effect. These data suggest that activities in and around water, especially while boating, should include life-jacket use. 156
Alcohol Use
Alcohol is a known contributing factor to drowning deaths. Data obtained primarily from telephone studies likely underrepresents the true burden of alcohol in drowning causation. In 2017, alcohol was a leading factor in boating-related deaths. 10 A 2004 review found that 30% to 70% of drowning fatalities have a measurable blood alcohol level, with 10% to 30% of deaths being directly attributed to alcohol use. 159
Lifeguards
There are no specific peer-reviewed studies on the utility of lifeguards on expeditions or wilderness trips. 160 A 2001 Centers for Disease Control and Prevention working group report recommends the presence of lifeguards for drowning prevention in open-water settings. In 2021, the United States Lifesaving Association reported nearly 7 million preventative actions and over 50,000 water rescues covering a population of almost 260 million beachgoers. There were 30 reported drowning deaths at guarded beaches compared with 80 deaths at beaches without lifeguards. 161 Among nationally recognized lifeguard-certifying agencies (Ellis & Associates, American Red Cross, Starfish Aquatics Institute, and National Aquatic Safety Company), there are no specific guidelines or recommendations for the number of lifeguards per number of participants in an event or at an aquatic facility.
Special Situations
Cold Water Survival
No single recommendation can address all possible scenarios in a water setting. An unintentional fall into a swift-moving river, deep offshore ocean, inland waterways, backyard swimming pool, or through ice into static or moving water are all treated according to the skill level, preparation, and equipment available to patient and rescuer. Immediate attention must always be given to self-rescue and extricating oneself from a hazardous environment.
There are 4 phases of cold water immersion (airways above water), each of which can contribute to aspiration and drowning.28,162 The first phase, the “cold shock response,” causes gasping and hyperventilation lasting 30–90 s. If the head is submersed (airway under water) during this phase, uncontrolled breathing can lead to immediate aspiration and drowning. The second phase, “cold incapacitation,” results as cooling of muscle and nerve fibers causes weakness and incoordination. Weakness may be evident after only a few minutes of submersion and progresses to incapacitation after 10 or more min; this may manifest as swim failure or inability to carry out other survival tasks. “Hypothermia” can take 30 or more minutes to occur in an adult who is not wearing specific thermal protective garments. A victim can only survive this long if flotation is available. In this case, drowning may occur if waves cover the airways. Finally, drowning may occur due to “rescue collapse” (otherwise known as circum-rescue collapse), which can occur just before, during, or shortly after rescue. It is thought that a main cause of this collapse (symptoms range from collapse to syncope to death) is that rescue can result in mental relaxation and a sudden reduction in epinephrine levels, leading to increased peripheral blood flow resulting in decreased blood pressure, decreased core temperature, and transport of metabolic byproducts from the periphery to the irritable heart.
After immersion in cold water, a person has a limited amount of time before fatigue and incapacitation render self-rescue impossible. Likelihood of survival is increased by having appropriate gear (eg, a PFD or lifejacket) and training and by dressing for water temperature, not just air temperature, in the event of immersion.
Extensive controlled trials of cold water survival are lacking, and the available literature is not generalizable to all scenarios. For example, sea state, weather, physical fitness, clothing, the presence of a lifejacket, and mental preparedness all contribute to survivability in cold water. Whitewater is different from still water or the ocean in polar regions. A single large literature review serves as the source for recommendations about cold water survival under ideal conditions and must be interpreted according to the level of training, preparation, and situation presented to the patient. 163
After immersion, the most important decisions a person must make are: 1) assessment of the presence of any potential immediate threats to life and 2) whether to swim to safety or await rescue. Should a person choose to await rescue, preventing loss of body heat becomes paramount. By positioning the body to protect major areas of heat loss, a patient may lengthen immersion survival time. A position that has been proven in a laboratory setting to decrease heat loss is the heat escape lessening position. The goal of this position is to decrease heat loss from areas such as the armpits; groin; and, to a lesser extent, neck. This position is achieved by pressing the arms against the sides of the chest and squeezing the legs together. If possible, additional protection may be obtained by flexing the hips and knees and shrugging the shoulders. In some cases, it may be possible to pull the knees to the chest with the hands. Some individuals will be unstable in this position; in this case, the arms can simply be folded across the chest. In the event of group immersion, huddle formation has been recommended to lessen heat loss, assist injured or weak persons, and improve group morale. Although this position has been shown to decrease cooling in participating individuals in a controlled environment, the effort needed to assist debilitated individuals in an actual emergency may result in increased heat loss (Figures 1 and 2). 164

Heat escape lessening position (used with permission from http://www.boat-ed.com).

Huddle formation (used with permission from http://www.boat-ed.com).
Swimming or treading water should be limited to minimize heat loss. Life jackets should be worn to aid insulation and flotation. If possible, the ideal location to await rescue is out of the water, even if only partially, to reduce heat loss and delay onset of hypothermia. Prolonged cold water exposure eventually results in motor disabilities, which can appear within 10 m of immersion, making advanced maneuvers difficult. For this reason, it may be beneficial to affix one's body or clothing to a floating object using rope or freeze clothing to the ice surface if exit is not possible. Prolonged immersion will also eventually lead to cognitive disabilities, rendering decision-making difficult.
Should a person decide to swim to safety, some important physiologic changes may occur. The initial cold shock, which lasts seconds to a few minutes, may prompt gasping and hyperventilation and can have a disorienting effect, making self-rescue attempts difficult. Upon immersion in cold water, if no immediate life threats are present, a person should focus on remaining calm and controlling breathing by taking slow, deep breaths. Once a person is able to obtain his or her bearings, he or she may have far less than 10 m of effective swimming and up to 1 h of consciousness before succumbing to hypothermia. All of these statements assume the person is wearing an appropriate life jacket. Further detailed discussion of the science behind cold water immersion is available in chapter 8 of Auerbach's Wilderness Medicine (7th edition). 28
Conclusions
Drowning is a process with outcomes ranging from no morbidity to severe morbidity to death. Persons who drown and survive with or without morbidity should be described as having had a nonfatal drowning. Those who do not survive should be described as having had a fatal drowning. The most important aspect of treatment is to reverse cerebral hypoxia by providing oxygen to the brain. Drowning prevention strategies can be effective and should be thoroughly deployed.
Supplemental Material
sj-pdf-1-wem-10.1177_10806032241227460 - Supplemental material for Wilderness Medical Society Clinical Practice Guidelines for the Treatment and Prevention of Drowning: 2024 Update
Supplemental material, sj-pdf-1-wem-10.1177_10806032241227460 for Wilderness Medical Society Clinical Practice Guidelines for the Treatment and Prevention of Drowning: 2024 Update by Christopher A. Davis, Andrew C. Schmidt, Justin R. Sempsrott, Seth C. Hawkins, Ali S. Arastu, Gordon G. Giesbrecht and Tracy A. Cushing in Wilderness & Environmental Medicine
Footnotes
Author Contribution(s)
All authors contributed to drafting, revision, and approval of final manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors report the following disclosures. AS, JS, and SH are directors of Lifeguards Without Borders. SH is Medical Director for Landmark Learning, Starfish Aquatics, and North Carolina State Parks as well as owner of Hawk Ventures. TC is section editor for WMS Practice Guidelines. AA, GG, and CD have no disclosures to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.