
Abstract
Studies examining the etiology of problematic sexual behavior (PSB) among pre-teen children often rely on identifying correlational relationships without examining potential causal mechanisms. This study describes an exploratory analysis of a potential mediational model where child sexual abuse (CSA) and child physical abuse (CPA) predict the onset of PSB through their impact on the emergence of posttraumatic stress (PTS) symptoms and self-dysregulation. The caregivers of 189 children between the ages of 3 and 11 years presenting for mental health treatment in the United States completed a battery of measures designed to assess each of the variables in the model. Cross-sectional, regression-based mediational analyses showed that the overall model performed adequately (R = 0.33, R 2 = 0.11, F = 3.07, p = .004). CSA exerted a direct effect on PSB that was not mediated through either PTS or self-dysregulation. However, no direct effect for CPA was found. Rather, CPA exerted a significant effect on the display of self-dysregulation, which in turn was associated with PSB. These results are discussed in light of clinical implications and directions for further research.
Preteen children displaying problematic sexual behavior (PSB) are defined as “children ages 12 and younger who initiate behaviors involving sexual body parts (i.e., genitals, anus, buttocks, or breasts) that are developmentally inappropriate or potentially harmful to themselves or others.” (Chaffin et al., 2008, p. 200). The types of behaviors subsumed under this broad definition are diverse and include exhibitionistic and voyeuristic behaviors, self-focused behaviors, and those involving physical contact with another individual. Although epidemiological data are not available, estimates from large sample studies suggest that PSB may occur among 20%–25% of children (Allen, 2017; Friedrich et al., 2001; Friedrich et al., 1991). Estimates of the persistence of PSB over the course of 1–2 years range from 43% to 56.7% (Ensink et al., 2018; Lévesque et al., 2012), suggesting that these concerns are chronic in a large proportion of cases.
Initial attempts to understand the etiology of PSB focused on a presumed connection with the occurrence of childhood sexual abuse (CSA). For instance, Friedrich and colleagues (2001) compared a sample of children with CSA histories to normative and psychiatric comparison samples and found the highest prevalence of PSB among those experiencing CSA. Other early studies similarly found CSA predicted the occurrence of PSB (e.g., Gray et al., 1999; Hall et al., 2002). Postulations on the mechanisms connecting the two factors largely centered on the role of CSA-related posttraumatic stress symptoms (PTS; e.g., intrusive thoughts) that are inherently sexual in nature (e.g., Finkelhor & Browne, 1985; Rasmussen, 1999). Indeed, some evidence suggests that PSB is more prevalent among CSA survivors when they report higher levels of PTS (Allen et al., 2015; Friedrich et al., 2003; Wamser-Nanney & Campbell, 2020).
However, the CSA-related PTS model possesses significant limitations. For one, several studies suggest that the minority of children displaying PSB have a CSA history (Allen, 2017; Bonner et al., 1999; Silovsky et al., 2007). Even in those cases of PSB where CSA is present, PTS may not be a mediating mechanism. For instance, Silovsky and Niec (2002) found that, of 13 cases of preschool children displaying PSB and having a CSA history, only two met diagnostic criteria for PTSD. Using continuous measures, Allen (2017) observed only weak evidence linking PTS to the display of PSB among CSA survivors and Wamser-Nanney and Campbell (2022) found that PTS did not explain the connection between CSA and PSB. Data from Simon and Feiring (2008) suggested the opposite effect, that PTS, particularly posttraumatic avoidance of sexual topics, may predict lower rates of PSB among children with CSA histories.
One alternative etiological hypothesis utilizes a developmental psychopathology framework (see Elkovitch et al., 2009). From this perspective, any number of events and circumstances may result in the aberrant development of one’s ability to tolerate and effectively modulate behaviors and emotions (i.e., self-regulation; Cicchetti & Toth, 1995). This difficulty with self-regulation is presumed to underlie various forms of psychopathology (Cicchetti & Rogosch, 1996), which may include PSB. Seen through this lens, CSA may impact the development of PSB through its effect on the emergence of self-dysregulation; however, other untoward developmental experiences may also create a similar effect. The most commonly identified antecedent of PSB outside of CSA is the experience of childhood physical abuse (CPA; e.g., Allen, 2017; Lévesque et al., 2010; Merrick et al., 2008; Silovsky & Niec, 2002)
There is evidence that CPA may play an influential role in the development of PSB. Friedrich et al. (2003) showed that children experiencing CSA were more likely to develop PSB if they also had a history of CPA and Pithers et al. (1998) found that CPA predicted a quicker onset of PSB following CSA. For those cases without a history of CSA, the experience of CPA is found to increase the risk for developing PSB two- to three-fold (Lévesque et al., 2010; Merrick et al., 2008). However, this finding is not uniform as some studies fail to find a connection between CPA and PSB (Smith et al., 2019).
Further evidence for the developmental psychopathology perspective comes from the multitude of studies showing a significant correlation between PSB and broader externalizing behavioral problems (e.g., Allen, 2017; Friedrich et al., 2003; Gray et al., 1999; Smith et al., 2019; Wamser-Nanney & Campbell, 2022). In addition, deficits in social competence also are well-established for children displaying PSB (e.g., Allen, 2017; Wamser-Nanney & Campbell, 2019), which may exacerbate anomalous developmental trajectories. These findings suggest that the concomitant display of broader externalizing/social problems and PSB are the result of a general etiological construct, presumably self-dysregulation.
Although these two etiological models (i.e., CSA-related PTS, developmental psychopathology) are commonly discussed in the literature, rarely are they examined in tandem. Rather, studies commonly test one perspective or the other and give little consideration to how the two perspectives relate. For instance, CSA may disrupt the development of adaptive self-regulation capabilities as well as cause the onset of PTS. As such, CSA may predict PSB through its effect on self-dysregulation regardless of whether PTS is present. Considering a developmental model such as this allows for the inclusion of other indicated developmental experiences, particularly CPA. One may hypothesize that CPA yields significant self-dysregulation, which may result in PSB in the absence of CSA or CSA-related PTS.
This study provides an initial test of this proposed developmental approach. Figure 1 graphically depicts the full mediational model, where experiences of CPA and CSA are hypothesized to predict the development of both self-dysregulation and PTS, and these mediating mechanisms, in turn, predict the emergence of PSB. Of course, there are likely other ways that CSA and CPA may cause PSB and these are accounted for by the direct effect pathways linking these variables. It should be noted prior to describing the method of this analysis that the data are cross-sectional in nature. As such, although the variables are arranged in a theoretically defensible manner in the model, the data were not collected in a longitudinal design. It is best to consider this analysis as an exploratory model testing the potentiality that the variables may be related in the manner specified. Full Mediation Model for Problematic Sexual Behavior.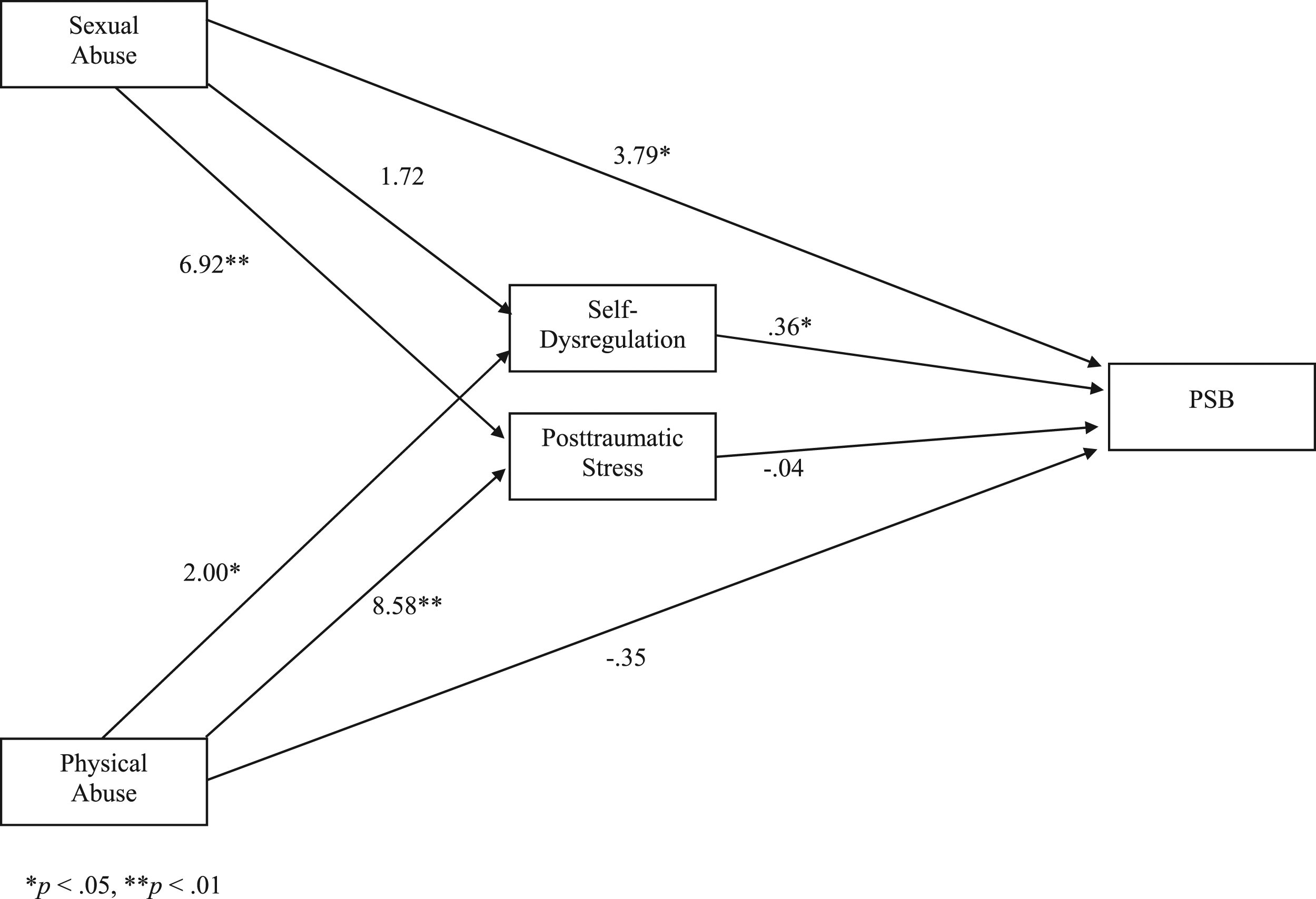
An additional issue deserves mention. It is not uncommon in studies of PSB for (a) the sample to consist exclusively of children with known PSB and for analyses to examine differences in severity or frequency, or (2) compare children with PSB to normative samples. Relatively few studies compare children with PSB to a suitable treatment-seeking sample not displaying PSB, which might explicate factors unique to the display of PSB. For example, one may expect to find higher rates of CPA, CSA, self-dysregulation, and PTS in children with PSB when compared to a normative sample, not because these factors relate necessarily to PSB, but because they relate to a mechanism common to various presenting concerns largely absent within the normative sample. This study employed a sample of children displaying PSB and/or with known maltreatment histories, which yields a sample comprised entirely of treatment-seeking cases.
Method
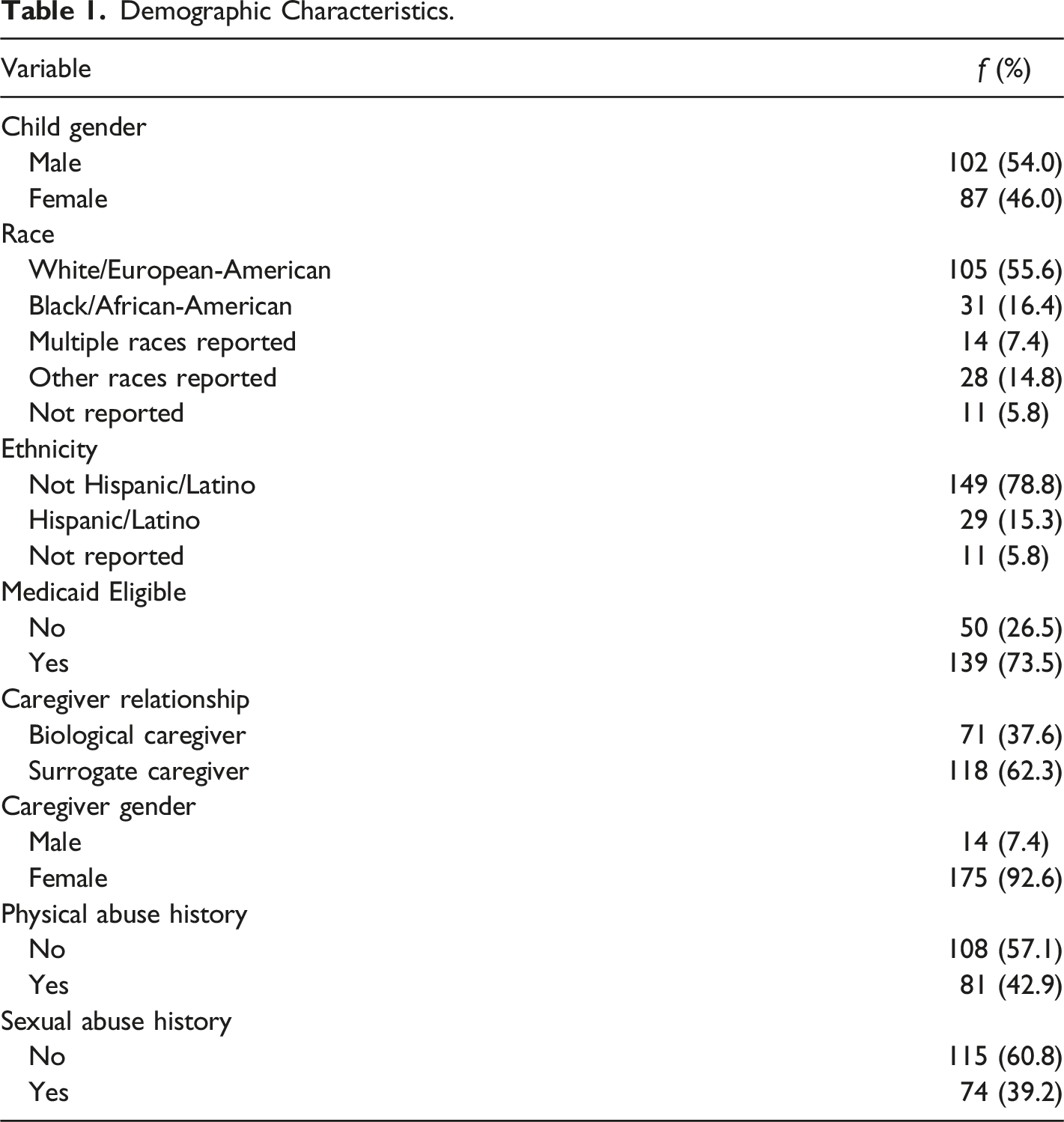
Participants
Demographic Characteristics.
Measures
Trauma History Screen (THS)
The THS is a 19-item screening measure for various forms of trauma and adversity (Lang & Franks, 2007). All caregivers were administered the THS in an interview format as part of the child’s initial evaluation and responded to each item in a yes/no format (coded: 0 = No, 1 = Yes). In cases of surrogate caregivers, the assessment interview was often supplemented with information provided by the child protective services (CPS) worker and incorporated into responses. The two items specifically assessing the child’s prior experience of sexual abuse and physical abuse were utilized for this study. Although a number of children presented for treatment with histories of other forms of maltreatment (e.g., physical neglect, exposure to inter-partner violence), these other forms of maltreatment are not consistently shown to predict the onset of PSB and, when they are indicated, the effect is often weak (Allen, 2017; Merrick et al., 2008). As such, these forms of maltreatment are not included in the specified models although children presenting with only these types of maltreatment are included in the total sample.
Trauma Symptom Checklist for Young Children (TSCYC)
The TSCYC is a widely-used 90-item caregiver-report measure of a child’s trauma-related symptomatology (Briere, 2005). It was developed for children between the ages of 3 and 12 years. Caregivers report how often each symptom occurred in the past month on a 4-point Likert-type scale ranging from 1 (not at all) to 4 (very often). For the current study, the TSCYC was administered at intake and the total score of the Posttraumatic Stress (PTS) subscale was used as an index of PTS. The TSCYC PTS subscale is repeatedly demonstrated to display acceptable internal consistency and to correlate strongly with other measures of childhood PTS (see Briere, 2005, for the results of multiple psychometric analyses). Internal consistency of the measure was excellent in the current sample (Cronbach’s α = .93).
Strengths and Difficulties Questionnaire (SDQ)
The SDQ (Goodman, 1997) is a widely used measure of youth emotional and behavioral concerns. It is a 25-item questionnaire where the caregiver is asked to identify whether each item is Not True (0), Somewhat True (1), or Certainly True (2) for the youth. The psychometric properties of the SDQ are well-established, including repeatedly demonstrated strong correlations between the SDQ and the Child Behavior Checklist (see Stone et al., 2010, for a meta-analytic review). Five subscales are derived from the SDQ items; the summation of three of these subscales (i.e., Conduct Problems, Emotional Problems, Hyperactivity) is generally considered a composite index of self-dysregulation (Deutz et al., 2018). This index was used for the current study and internal consistency within the present sample was strong (α = .84).
Child Sexual Behavior Inventory (CSBI)
The CSBI is the current “gold standard” measure for assessing PSB among preteen children (Friedrich, 1997). However, many of the items are considered objectionable in contemporary practice (e.g., “Dresses like the opposite sex.”) or ask about behaviors that are not captured by contemporary definitions of PSB. For these reasons, a modified form of the CSBI was employed that eliminated questions designed to assess transgender behaviors, non-sexual boundary violations (e.g., “Stands too close to people”), and subjective caregiver opinions of normality (e.g., “Knows more about sex than other children their age”). The final measure included 28 items assessing exhibitionistic, voyeuristic, self-focused, and intrusive/interpersonal forms of sexual behavior. Modification of the CSBI is common in developmental research (e.g., Allen, 2017; Lussier et al., 2018) largely because of the issues discussed here. In addition, the norms for the CSBI were collected over 30 years ago and are generally considered out-of-date. This precludes identifying clinical cutoffs or utilizing T-score conversations. For this reason, raw scores were used for the current study. Higher scores inherently reflect the display of a greater number of discrete behaviors and/or a greater frequency of exhibiting the endorsed behaviors. As such, while lower scores may reflect non-clinical forms of sexual behavior, higher scores suggest an increasing likelihood that a child is displaying PSB. The internal consistency of the measure was strong in the current sample (α = .89).
Data Analysis
Initial analyses examined the normality of the distributions of continuous data and applied necessary transformations to allow for valid parametric analyses. Next, several demographic factors were examined for their potential relationship to model variables using t-tests, ANOVAs, Pearson product-moment correlations, and X 2 tests, depending on the structure of the data. Demographic variables identified as significantly related to at least one model variable were subsequently entered as covariates during estimation of the mediational model. Lastly, the full hypothesized mediational model was tested using the PROCESS macro (v. 4.0) for SPSS v. 28, which utilizes ordinary least squares regression (Hayes, 2022). The statistical significance of each direct pathway was determined using t-tests and the overall model was evaluated as any other multiple regression model. It should be noted that the model evaluated was prespecified based on theoretical grounds and prior research, and was not constructed after preliminary analyses suggested the nature of relationships within the data.
PROCESS evaluates indirect effects using a percentile bootstrap method that generates 95% confidence intervals derived from 5000 bootstrap samples. Using this method, if the calculated confidence interval includes 0, the indirect/mediational pathway is not statistically significant. According to a simulation study conducted by Fritz and Mackinnon (2007), a sample size of 162 is required to detect statistically significant mediational effects using percentile bootstrap methods when the effect sizes of the involved pathways are halfway between the coefficients customarily considered small and medium in strength. However, only 78 cases are required when the effect sizes are medium in strength. Given these estimates, the current sample size of 189 appears more than sufficient to detect statistical significance given medium effect sizes, and it is likely that power is sufficient to detect effects of a lesser magnitude as well. The author takes responsibility for the integrity of the data, the accuracy of the data analyses, and has made every effort to avoid inflating statistically significant results.
Results
Preliminary Analyses
Normality checks showed that one of the continuous variables, PSB, exhibited extreme positive skew (Kolmogorov-Smirnov = 0.27, p < .001; Shapiro-Wilk = 0.66, p < .001) given the high proportion of cases who received the lowest possible score of 0 (n = 78, 41.3%). As a result, the variable was inverse transformed with the addition of a constant (+1). All reported parametric analyses utilized this transformed variable in calculations. However, given that coefficients related to transformed variables are difficult to interpret, all coefficients reported were calculated with raw, untransformed data for the PSB variable.
Using indicated parametric and non-parametric methods, the following statistically significant relationships were found between demographic and model variables: physical abuse experience was more prevalent among children qualifying for Medicaid (X 2 = 6.13, p = .013); biological caregivers reported higher levels of PTS (t = 3.78, p < .001) than surrogate caregivers; an older age was weakly associated with lower scores for PSB (r = 0.20, p = .007). As such, Medicaid eligibility, caregiver relationship, and age were included as covariates in model estimates.
It should also be noted that of the 189 cases included in this analysis, only 31 endorsed a history of both CSA and CPA, yielding extremely limited power to detect an interactive effect. However, significant concerns are noted in contemporary child maltreatment research regarding the contamination of studies when one fails to control for the impact of other forms of maltreatment (e.g., CPA) that may co-occur with the primary subject of the study (e.g., CSA; see Shenk et al., 2022). The use of multiple regression analyses in the current study results in the statistical controlling of the impact of one type of abuse while deriving coefficients for the effect of the other type of abuse, thus addressing this concern. In other words, although the interactive effect of the two forms of abuse could not be effectively evaluated, the impact of CSA is controlled when estimating the effects for CPA, and vice versa.
The Mediational Model
Bivariate Correlations.
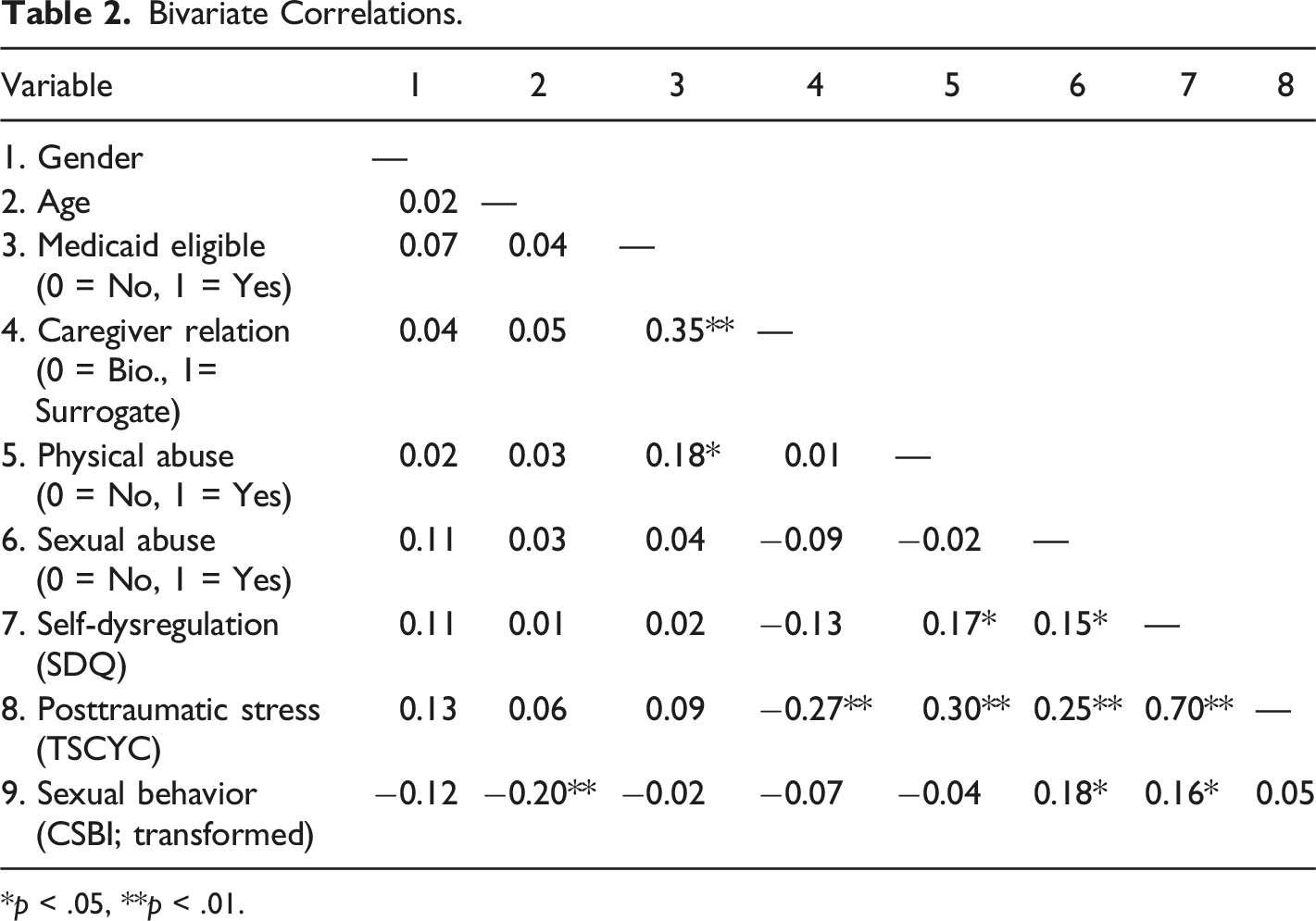
*p < .05, **p < .01.
The full mediational model significantly predicted PSB and with a medium size effect (R = 0.33, R 2 = 0.11, F = 3.07, p = .004). Results examining the direct and indirect effects for CSA and CPA on PSB provided interesting results. The estimate for CSA exerting a direct effect on PSB was significant (ß = 3.79, t = 2.54, p = .012); however, there was no evidence of an indirect effect for CSA through self-dysregulation (ß = 0.027, 95% CI = −0.002–0.072). Meanwhile, results pertaining to CPA provided a contrasting picture. The direct effect of CPA on PSB was not significant (ß = −0.35, t = −0.29, p = .77), although CPA was observed to exert an indirect effect on PSB through its influence on self-dysregulation (ß = 0.032, 95% CI = 0.001–0.077).
Discussion
In many cases, the etiology of PSB is likely a complex interplay between multiple factors. This study tested the combined contribution of two different hypotheses regarding the emergence of PSB: posttraumatic stress symptoms secondary to CSA and the development of self-dysregulation. In addition, this study incorporated two experiences most frequently associated with PSB, CSA and CPA.
Results of the mediational model suggested that CSA did exert a significant direct effect on the display of PSB, but was not mediated through PTS or self-dysregulation. This finding is not unique to the literature as Wamser-Nanney and Campbell (2019) similarly found that CSA continued to predict PSB after controlling for PTS. Such findings require the incorporation of other etiological perspectives to explain such a relationship. The most likely explanation utilizes a social learning perspective, which suggests that the sexual nature of the abuse provided a modeling experience which influenced the development of PSB. Consider Cale and Lussier’s (2017) sample of preschool children exposed to inter-partner violence (IPV). Children exposed to sexual coercion occurring within the IPV were more than twice as likely to development PSB as those children whose IPV exposure did not involve sexual coercion. More directly as it pertains to CSA, Friedrich et al. (2003) initially found that CSA predicted PSB, but this relationship no longer held after controlling for the child’s exposure to various forms of expressed sexuality within home. In other words, after accounting for a form of non-CSA social modeling of sexual behavior, CSA was no longer connected to PSB. These studies suggest that CSA may increase the likelihood of PSB largely as a result of the social modeling provided to the child.
CPA, on the other hand, was not directly related to the display of PSB. Rather, there was evidence that the experience of CPA played a role in the development of self-dysregulation, which in turn was associated with the display of PSB. Indeed, the formative experience of CPA on dysregulated emotions and behaviors is well-established (Kim & Cicchetti, 2010; Kim et al., 2023) and it is likely this factor accounts for the often-cited association between PSB and others forms of externalizing psychopathology (e.g., Allen, 2017; Smith et al., 2019; Wamser-Nanney & Campbell, 2022). In this view, the emergence of PSB is more related to aberrant development as opposed to a specific stressor or event.
The regression-based methodology of the current study provides an important strength for the study: the collective influence of other model variables was statistically controlled when determining whether a specific variable was associated with the outcome. In other words, the direct effect of sexual abuse on PSB remained after controlling for CPA, self-dysregulation, PTS, and the demographic covariates. Similarly, the indirect effect of CPA on PSB through self-dysregulation was significant after controlling for CSA and the rest of the entered variables. This suggests that each of the two identified pathways (i.e., CSA, developmental psychopathology) may operate independently and constitute two distinct avenues through which PSB may arise.
These results have clear clinical implications. Given the finding that PTS did not mediate the impact of CSA on PSB, there is little suggestion that a trauma-focused intervention specifically targeting post-CSA PTS may improve PSB. Although PSB is frequently included as a secondary outcome in clinical trials of interventions targeting CSA-related PTS (e.g., Allen & Hoskowitz, 2017; Cohen et al., 2004), no trials test the effectiveness of a trauma-focused intervention for children displaying clinically elevated levels of PSB. Rather, a developmental psychopathology perspective argues for the importance of an intervention that can improve self-regulation as a means of reducing PSB. Much like the research on treatment for other forms of externalizing problems (see Kaminski & Claussen, 2017), behavioral parent-training models appear worthy of study. There is evidence that such programs not only improve self-regulation (e.g., Lieneman et al., 2020), but may also reduce harsh physical discipline practices that may promote and maintain poor regulatory ability (Chaffin et al., 2004). As it relates specifically to PSB, there is preliminary evidence that such behavioral parent-training interventions may be effective (Allen et al., 2016; St. Amand et al., 2008). In addition, those interventions designed specifically to treat PSB teach caregivers behavioral child management skills (Allen et al., 2018; Silovsky et al., 2007).
It should be reiterated that the data for the current study were cross-sectional in nature, which prevents demonstrating that the variables examined relate in the developmental nature presented. Longitudinal studies of the onset and trajectory of PSB are necessary to push the field forward and may confirm the model specified here or identify necessary modifications. It must also be remembered that PSB is a broad concept that subsumes a diversity of phenomenologies (e.g., self-focused, intrusive/interpersonal). Future studies may examine specific subtypes of PSB to determine how etiological factors might differentiate between them. In addition, while the current study examined mediational pathways, it did not examine potential moderation of effects. Determining whether demographic factors moderate the relationship between a mediator and the outcome of PSB or whether two mediators may combine to enhance vulnerability for the development of PSB (e.g., the combination of PTS and self-dysregulation) are suitable next steps. In addition, the inclusion of techniques designed to assess the contribution of social learning mechanisms may help in determining how CSA fosters the development of PSB. By identifying the underlying etiological mechanisms of PSB, it may be possible to more effectively design and test appropriate interventions.
Footnotes
Authors’ Note
The author takes responsibility for the integrity of the data, the accuracy of the data analyses, and has made every effort to avoid inflating statistically significant results.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Allen is supported by grants R01HD097707 and P50HD089922 from the Eunice Kennedy Shriver National Institute for Child Health and Human Development (NICHD). The views expressed in this paper are solely those of the author and do not necessarily reflect the views of NICHD or the National Institutes of Health (NIH).