
Abstract
Many efforts to prevent child sexual abuse (CSA) aim to teach children strategies for recognizing, resisting, and reporting victimization. There is limited evidence that victimization-focused efforts actually prevent CSA. Moreover, these efforts often overlook the fact that many children and adolescents engage in problem sexual behavior against younger children. Responsible Behavior with Younger Children (RBYC) is a novel universal school-based perpetration-focused intervention that aims to prevent the onset of inappropriate, harmful, or illegal sexual behavior by adolescents against younger children. 1 Responsible behavior with younger children was designed to provide adolescents and their parents with the knowledge and tools to help adolescents interact appropriately with younger children and avoid CSA behaviors. In this paper we describe intervention development, summarize lessons learned from implementing RBYC in four urban schools, and report results from our pilot randomized waitlist-controlled trial (RCT) with 160 6th and 7th grade students. Results indicate RBYC was associated with increased accuracy in youth knowledge about CSA and CSA-related laws, and with increased behavioral intention to avoid or prevent CSA with younger children and peer sexual harassment. Although the sample was small and the effects were relatively modest, the findings do suggest that RBYC holds promise for preventing the onset of problem sexual behavior.
One of the many troubling aspects about the sexual abuse of children under age 18 is the high proportion of cases committed by other children and adolescents under age 18. In representative surveys conducted in the U.S., more than 70% of female survivors of child sexual abuse (CSA) reported their abuse was committed by another child, most often a slightly older adolescent (Gewirtz-Meydan & Finkelhor, 2020). Juvenile justice records indicate that victims under age 12 were most likely to be offended against by adolescents ages 12–14 (vs. by children under age 12 or over age 14 (Finkelhor et al., 2009; Snyder, 2000).
While these data may seem surprising to some, early adolescence is the time when most people are first learning how to engage in sex with others and navigate sexual relationships. All youth are vulnerable to making mistakes and bad decisions when first engaging in complex behaviors governed by complex rules and norms, which is particularly characteristic of sexual behavior. Further complicating this issue is the lack of clarity in the information youth receive from adults about developmentally-normative sexual behavior and related concepts, including sexual consent and age of consent (Letourneau et al., 2017; Ruzicka et al., 2021). Although many schools offer sex education or victimization-focused prevention curricula, and many parents talk with their children and adolescents about sexual abuse (Mendelson & Letourneau, 2015; Whitaker et al., 2008; Wurtele, 2009), those activities rarely address youth perpetration of sexual harm against younger children or the more general issue of adolescents being vulnerable not only to sexual abuse victimization but also to sexual abuse perpetration.
Globally, approximately 12% of children experience CSA victimization (Stoltenborgh et al., 2011). The immediate impacts of CSA victimization can include fear, concern for safety, injury, sexually transmitted infections, and pregnancy (Basil et al., 2022). Child sexual abuse victimization also places survivors at increased risk of longer-term health problems. These include the development of mental health problems including post-traumatic stress disorder, mood and anxiety disorders, and substance use disorders (Noll, 2021); behavioral and physical health problems including suicidal and non-suicidal self-harm, eating disorders, obesity, and HIV (Hailes et al., 2019); and sexual health problems including pain and problems with sexual arousal or desire (Pulverman et al., 2018).
The impacts of CSA perpetration by an adolescent are also severe and can include adjudication, prison, and sex offender registration and notification (Fix et al., 2020). These legal consequences are ineffective and deleteriously impact child well-being. For example, youth prisons fail to prevent recidivism and “subject confined youth to intolerable levels of violence, abuse, and other forms of maltreatment” (Mendel, 2011, p. 5). Likewise, registration of adolescents fails to reduce recidivism and is associated with severe harms (Fix et al., 2020). For example, relative to adolescents with sex crime adjudications who were not subjected to sex offender registration, adolescents required to register were four times more likely to have attempted suicide in the past month, five times more likely to have been approached by an adult for sex in the past year and twice as likely to have been sexually assaulted in the past year (Letourneau et al., 2018).
Given manifold harms to children and adolescents who experience and who cause sexual harm, there is a clear and urgent need for effective prevention efforts targeting the onset of sexual offending behaviors. Yet there is a dearth of such preventive programming and limited evidence that prevention efforts to date have translated into a populational level reduction in sexual violence and harm against teens or younger children (Letourneau et al., 2017; Marcantonio et al., 2022; Wurtele, 2009). Some evidence-based interventions appear to effectively prevent sexual harassment and violence by adolescents against peers (Clinton-Sherrod et al., 2009; DeGue et al., 2014; Foshee et al., 1998, 2004; Taylor et al., 2013). However, these programs do not address the risk of adolescents engaging in harmful or illegal sexual behavior against younger children. In fact, aside from the program tested in this paper, we know of just one other prevention program that specifically targets the sexual abuse of younger children by adolescents, the Berlin Project for Primary Prevention of CSA by Juveniles. This model offers a clinic-based selective intervention for adolescents diagnosed with a sexual preference for younger children (Beier et al., 2016). Yet, few adolescents adjudicated for sex crimes have preferential sexual attraction to younger children or other readily identifiable risk factors such as persistent violence (Chaffin, 2008; Letourneau & Schaeffer, 2014; Letourneau et al., 2017). More common risk factors include lack of knowledge about appropriate sexual partners, about appropriate sexual behaviors and mores, and about CSA and prohibitions against it (Chaffin, 2008; Letourneau et al., 2009, 2013, 2017). Additional risk factors include immaturity, impulsivity, imitation (including survivors of CSA victimization), and irresponsible experimentation or misinterpretation of sexual cues (Chaffin, 2008). Moreover, sex crimes by adolescents against younger children are often “crimes of opportunity”, occurring without premeditation and in contexts of convenience such as babysitting (Finkelhor & Ormrod, 2001, p. 5). Thus, while selected interventions will be important for some at-risk groups, these programs will miss the majority of adolescents who are at risk due primarily to age, ignorance, and opportunity.
Furthermore, situating prevention interventions in school settings (vs. clinics) offers the broader public health benefit of near-universal reach that can be targeted to specific age groups and delivered at relatively low cost. There are numerous successful examples of universal school-based prevention curricula addressing adolescent perpetration of other harmful behaviors including bullying (Bradshaw, 2015; Farrington & Ttofi, 2009), dating violence (Taylor et al., 2013, 2015), and antisocial behavior (Hahn et al., 2007; Wilson & Lipsey, 2007). These and other successful school-based prevention programs indicate best practices on which to base the development of a novel universal curriculum targeting the onset of CSA perpetration by adolescents, as we describe next. To address gaps in the CSA prevention field, the purpose of the current paper is to describe the development and initial testing of a novel school-based prevention program called Responsible Behavior with Younger Children (RBYC) in 6th and 7th grade students and to examine its efficacy in reducing proximal indicators of CSA perpetration risk.
The Responsible Behavior with Younger Children Program
RBYC is a school-based universal prevention program designed to provide adolescents and their parents (or other guardians) with the knowledge and tools to help adolescents interact appropriately with younger children and avoid engaging younger children in sexual behaviors (Ruzicka et al., 2021). We designed RBYC for 6th and 7th grade students because these students are typically younger than 14 years, the peak age (among teens) of sexual offending against younger children (Finkelhor, 2009; Snyder, 2000), yet are old enough to be contemplating or engaging in early sexual behaviors (Moore et al., 2013).
Initial content for RBYC sessions was based on risk factors associated with adolescent problem sexual behavior (Chaffin, 2008; Letourneau et al., 2017) and our experience developing and validating interventions for adolescent behavior problems (Bradshaw, 2015; Herman et al., 2014; Jowers et al., 2007; Letourneau et al., 2013, 2016, 2017). Risk factors include lack of knowledge about key concepts such as what constitutes CSA, the conditions under which CSA occurs, legal issues that pertain to CSA, and sexual consent, as well as strategies to avoid, prevent, or address CSA. We also address peer sexual harassment within the context of RBYC, given thematic relevance to adolescents and school systems and given overlap in many of the key concepts and prevention strategies. We framed RBYC within the context of responsible behavior with younger children to distinguish this intervention from sexual education. In alignment with this strategy and to ease into discussion related to CSA, we first introduce content on developmental differences between teens and younger children and empathic responding to younger children.
To encourage uptake, we designed RBYC to function either as a stand-alone curriculum or to be integrated with existing curricula (e.g., focused on health education, sex education, violence prevention). We also designed RBYC to be delivered to mixed or single-gender groups. However, we note that there is some evidence that boys are more likely to acquire and retain key concepts of sexual violence prevention programming when delivered in mixed-gender (rather than boys-only) settings (Clinton-Sherrod et al., 2009).
Before testing the efficacy of RBYC, we completed a multi-step process to identify and revise problematic intervention elements (Tripp & Bichelmeyer, 1990). First, we convened separate focus groups of middle school students, parents, and educators to obtain feedback on intervention content relevance, acceptability, and comprehensiveness (Ruzicka et al., 2021). We then used a rapid prototyping process to further refine content. Specifically, study staff delivered discrete elements of the RBYC curricula at three partnering schools and observed student and educator engagement levels and reactions. Students provided immediate oral feedback on “what worked/what needs work” that was recorded by the research assistants. We revised session content based on observations and feedback and then delivered the revised elements to a new class using the same qualitative strategies. Once we prototyped and revised major intervention elements, we evaluated RBYC in a pilot randomized controlled trial (RCT).
Overview of the Current Study
The purpose of this study is to present results from the pilot RCT of RBYC conducted with 6th and 7th grade students in partnership with four urban middle schools. Consistent with the literature regarding risk factors for CSA perpetration and the targets of RBYC interventions, we hypothesized that the students who received RBYC would demonstrate more accurate knowledge about developmental differences between younger children versus adolescents, greater empathy for younger children, more accurate knowledge about CSA and related laws and concepts, and express greater behavioral intention to avoid harmful or illegal sexual behavior against younger children and against peers relative to students in the control condition.
Method
General Overview
We recruited four urban middle schools in Maryland, three of which had participated in the focus groups and/or rapid prototyping procedures used to develop RBYC in the 2 years prior to the RCT. The prior research efforts included only 7th grade students, the vast majority (≥95%) of whom would have advanced to 8th grade and been ineligible to participate in the current study (Plank et al., n.d.). Schools were recruited for participation in the pilot RCT for the 2018–19 school year based on existing relationships with the investigators, acceptance of research procedures, and interest in RBYC programming. Schools were located in four different urban neighborhoods serving primarily low-income students; all provided school-wide free meals. Student populations were majority Black/African American in three schools and majority Hispanic ethnicity in one school.
One school was larger than the others and contributed just over half of our recruited student sample. The project was approved by three researchers’ institutional review boards (IRB) and the school system’s IRB. To further ensure the integrity of this project and protections for student participants, we convened a parent advisory group comprised of one parent from each participating school as well as an expert advisory group comprised of two external child development experts to advise the investigators prior to and throughout the RCT.
Participants and Enrollment
Participant Demographic Characteristics at Baseline.
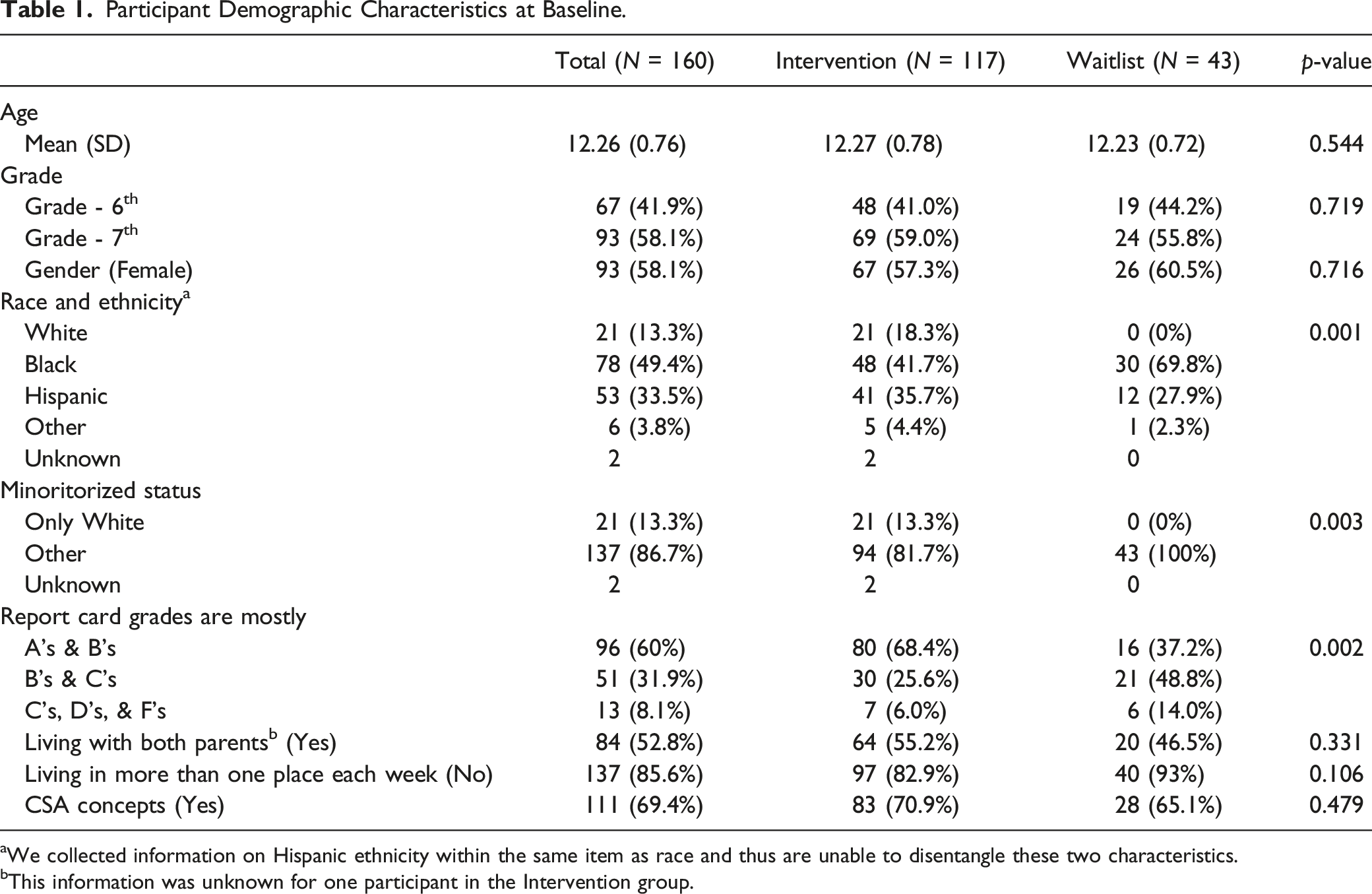
aWe collected information on Hispanic ethnicity within the same item as race and thus are unable to disentangle these two characteristics.
bThis information was unknown for one participant in the Intervention group.
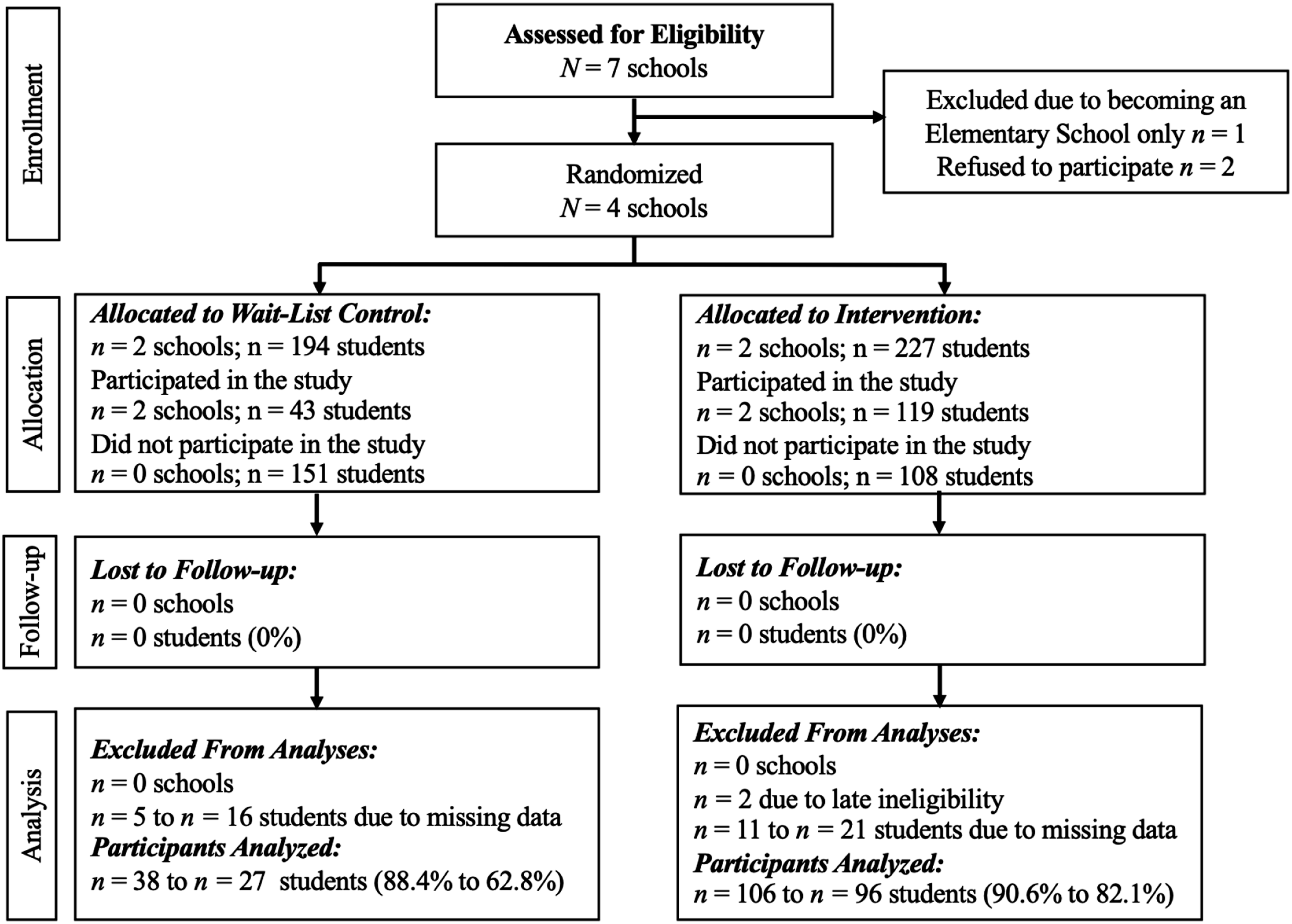
Consort diagram for the RBYC pilot trial.
Study Design and Randomization
In fall of 2018, participating schools were randomly assigned to either receive RBYC early in the spring semester of 2019 (RBYC Intervention group; 2 schools; n = 117 students) or later in the spring semester (Waitlist group; 2 schools; n = 43 students). We used a simple random number generator and placed groups with odd numbers in the waitlist condition and even numbers in the intervention condition.
All students completed a baseline assessment at the start of the spring semester (time 0). Students in the intervention condition then received RBYC and completed a post-intervention assessment (time 1) about 2 months later. Students in the wait-list condition completed a second baseline assessment at about that same time as the intervention students completed their post-intervention assessment (time 1), then received RBYC and completed a post-intervention assessment (time 2) at the end of the spring semester. In this paper we focus on the time 0 and time 1 data only.
RBYC Program and Program Implementation
The RBYC curriculum has eight core content sessions, each of which lasts approximately 45 minutes, in addition to orienting introductory and concluding sessions. Sessions addressed: 1) Developmental differences between children vs. teenagers; 2) Perspective-taking of and empathic responding to younger children; 3) Healthy versus unhealthy teenage-younger child relationships (Part A, which focuses on defining and describing sexual development, informed consent, and child sexual abuse); 4) Healthy versus unhealthy teenage-younger child relationships (Part B, which focuses on understanding behaviors that constitute child sexual abuse and harmful or inappropriate behaviors and building skills to identify and choose responsible behaviors to keep self and others safe); 5) Misconceptions vs. facts about child sexual abuse and legal ramifications; 6) Why adolescents may engage in harmful sexual behaviors or child sexual abuse and responsible behaviors for prevention; 7) Peer sexual harassment, what it is and how to avoid or address it, including how to identify and reach out to safe adults in various settings; and 8) Being a good bystander or upstander when you have concerns that another child or peer has been or may be harmed.
We incorporated behavioral skill practice (e.g., role plays) and physical activities in each session, in light of evidence that these strategies improve engagement, learning, retention, and use of new skills (Bradshaw, 2015). We also developed four family activities for students to lead with their parents/guardians periodically throughout the curriculum, because engaging parents in prevention programming has been found to improve student knowledge and skills (Herman et al., 2014; Jowers et al., 2007). Family activities were designed to promote parental awareness of situational factors that increase risk for CSA, encourage parent-child communication about CSA, and establish clear family rules against sex with younger children.
When possible, the RBYC curriculum was integrated into the participating school’s health or sex education curriculum; however, these curricula varied widely. Two schools did not deliver a formal health or sex education curriculum the year of our study (e.g., due to teacher turn-over). When schools did have a curricula and content appeared to overlap with RBYC core concepts (e.g., regarding sexual consent), the schools agreed replace those lessons with the RBYC content. All schools implemented passive consent for their health curricula, in which students received the curricula unless the student or a parent or other legal guardian provided an opt out form. All parents received information describing RBYC and an opt out form specific to RBYC. Consistent with standard school practice, the 15 students who opted out of participation in RBYC were provided alternative content in a different classroom with other students in their grade (the specific alternative content varied both within and between schools).
RBYC sessions were delivered by two implementation coaches who were hired, trained, and supervised by the study investigators to ensure high fidelity implementation of the program. The interventionists (one Black man, one Filipina woman) and their direct supervisors (one Black woman, one White woman) had significant experience implementing evaluation studies of middle-school curricula in that school district. The interventionists each received approximately 40 hours of training on RBYC including practice implementing sessions. Additional training and supervision focused on recognizing and addressing student distress, addressing student disclosures of abuse or other concerns, and providing students, parents, and educators with requested resources.
To ensure high fidelity implementation of RBYC, the interventionists completed a written self-reported log following each RBYC session; these logs recorded detailed notes on the administration of the program’s core components, as well as session attendance, any implementation challenges (e.g., elements that could not be covered, deviations from the curriculum manual), and perceived student engagement, rapport, and group dynamics. Supervisors met weekly with interventionists to review fidelity information, answer questions, and address concerns. Supervisors also conducted 12 live observations of classroom sessions (6 per interventionist) to assess implementation quality, participant engagement, and the administration of the core components of the lessons; the supervisors provided feedback to the interventionists based on each observation and ongoing review of the fidelity data collected by the interventionists.
We intended to deliver RBYC at the rate of one, 45-minute session per week; however, each school required a modification to this format. In one school, two sessions occurred per week a few times to accommodate snow days, annual state testing, and spring break. At three schools, RBYC sessions were delivered in more frequent and shorter segments (two to three times per week) due to shorter class periods and more rapidly alternating instruction cycles. Such minor adaptations to delivery are common in real-world settings (Gottfredson et al., 2015).
Data Collection Protocol
Baseline and post-intervention assessments were conducted in groups by class, typically as part of a class session. Make-up sessions were provided as needed for absent students. Care was taken to distance student seating so they could not oversee one another’s responses. To further enhance confidentiality, all participants were instructed to create a 7-digit self-generated anonymous identification number to use on each assessment form (see Vacek et al., 2017). This number was used to link pre- and post-intervention assessments for individual participants. As mandated by the lead author’s IRB, participants were re-assented prior to each assessment. At all assessments, students were reminded that they could skip any questions or end the assessment at any time without penalty.
Assessments were completed on electronic tablets provided by the research team. Students were given the option to listen to a recording of questions via headphones or to read questions. Following each assessment, participants were provided with a hard-copy form listing mental health resources in the school (e.g., school counselor’s name and contact information), community (e.g., local mental health providers), and nationally (e.g., helplines). Specific resources pertained to CSA victimization, concerns about one’s own or someone else’s sexual thoughts or behaviors, and concerns about suicide. Participants were also told they could reach out to any member of our research team for assistance and were informed in writing and verbally about limits to confidentiality and about mandated reporting requirements. Participants received a $5 gift card after completing each assessment. During data collection, a three-person team from the study was available to address questions and technical issues.
Measures
To evaluate core constructs addressed within RBYC, we sought measures to assess change in knowledge about developmental differences between children and adolescents, empathic responding toward younger children, knowledge of CSA and issues related to legal consequences and important constructs such as sexual consent. We also sought to assess the impact of RBYC on the perpetration of sexual abuse against younger children and of sexual harassment and abuse against peers. We were not permitted by the IRB to inquire about specific CSA or peer perpetration behaviors and it is unlikely that the sample size from this study was sufficient to power analyses of these low base rate behaviors. To get a signal of behavioral change, we instead assessed participants’ intentions to avoid, interrupt, and address CSA and, separately, to avoid, interrupt, and address peer sexual harassment. In addition, we sought to characterize participants’ prior exposure to CSA prevention messaging and social norms regarding sexual behavior against younger children and with peers.
Unfortunately, there is a dearth of pre-existing measures relevant to assessing CSA prevention outcomes (Wurtele, 2009). Therefore, we created or adapted most of the items and scales used to measure our outcomes of interest. Some of these new or adapted items and scales performed reasonably well and results are reported below. Several measures, however, did not perform well. For example, to assess social norms about sexual behavior with peers we utilized the Student Health Questionnaire (Marín et al., 2000) and we adapted those items to assess social norms about sexual behavior with younger children. At Baseline, Cronbach’s alphas for both measures were 0.63 and 0.39, respectively. Likewise, to assess change in empathy toward younger children, we adapted two scales from the Interpersonal Reactivity Index, including Perspective Taking and Empathic Concern (Davis, 1980). At Baseline, Cronbach’s alpha for both scales were 0.45 and 0.67, respectively. Given these low alphas we dropped these measures from further consideration. All items used in this project are available from the authors and in an online supplemental appendix. Each of our assessments began with a review of definitions of two recurring terms: “younger children” and “peers”. Younger children were defined as, “someone who is at least 3 years younger than you. This includes babies, toddlers, preschoolers, kindergarteners and kids in 1st, 2nd and 3rd grade. These children are about 0–9 years old”. Peers were defined as “boys and girls about the same age as you who are no more than 3 years older or younger than you. They may be people in your class, school, neighborhood, or community. You may or may not think of them as your friends”.
Demographic characteristics and prior exposure to CSA information
We obtained self-reported demographic information from all participants at Baseline (see Table 1). The gender item included several options of which only ‘male’ and ‘female’ were selected by participants. Race and Hispanic ethnicity were obtained in a single forced-choice item and therefore we are unable to disentangle Hispanic ethnicity from race; this item was dichotomized to indicate minoritized status - white only versus Other - for analyses. We also asked participants whether their parent or another caregiver had ever talked with them about CSA. Response options to both items were yes, no, and not sure.
Developmental differences – Baseline and Post-intervention assessments
RBYC aims to educate adolescents about developmental differences between adolescents and younger children. We were unable to identify an existing relevant measure and therefore created seven items to assess knowledge about developmental differences between adolescents and younger children. For example, “Children might feel frustrated when they can’t do the same things as teenagers.” Response options were true or false and scored as 0 (inaccurate) or 1 (accurate). A total score was computed by summing the seven items (range = 0–7), with higher scores indicating more accurate understanding of developmental differences between teenagers and younger children.
Knowledge about CSA and related concepts - Baseline and Post-intervention assessments
RBYC aims to improve students’ knowledge about CSA and related laws and concepts. While we identified several measures that assessed similar constructs (Halperin et al., 1996; Hunter et al., 1991; Tutty, 1995), none met our needs, often because item wording was specific to forensic populations or quite dated. Using existing measures as a guide, we developed 41 true/false items coded as 0 (inaccurate) or 1 (accurate) to assess five core areas of knowledge. Items comprising a given subscale were summed for a subscale score, with higher scores indicating more accurate knowledge. The five areas included: 1. CSA Facts. Students’ knowledge about CSA was assessed with 15 items. For example, “Having sex with a child may hurt the child later in life.” 2. CSA Laws. Students’ knowledge about laws and legal consequences regarding CSA was assessed with seven items. For example, “In Maryland, a teen can’t get in trouble for sharing nude pictures of someone under the age of 18.” 3. CSA Prevention. Knowledge about strategies to prevent or avoid CSA was assessed with seven items. For example, “It is OK to say ‘no’ and move away if someone touches you in a way you don’t like.” 4. Knowledge about Sexual Harassment. Knowledge about peer sexual harassment was assessed with eight items. For example, “As long as you are just joking around, what you say or do to someone cannot be considered sexual harassment.” 5. Sexual Consent. Students’ knowledge about sexual consent was assessed with four items. For example, “If two people are dating, they need to consent to sex each time they have sex.”
Peer sexual harassment behaviors – Baseline and Post-intervention assessments
Prevention of peer sexual harassment perpetration has previously been demonstrated by existing interventions such as Shifting Boundaries, a peer-focused sexual harassment and sexual violence prevention program for middle school students (Taylor et al., 2015). We included content about peer sexual harassment and violence in one session of RBYC because CSA and peer-focused sexual abuse are thematically related and because we anticipated that school administrators and educators would expect to see such coverage. We were permitted by the IRB of record only to inquire about relatively minor forms of peer sexual harassment behaviors. To do so, we used five items from a measure created by Taylor et al. (2011). For example, “Have you ever done any of the following with a peer: Made sexual comments, jokes, gestures, or looks to them?” Response options were no (0) or yes (1) and were summed to provide a final score that ranged from 0–5 with higher scores indicating engaging in more harassing behaviors.
Behavioral intention to avoid or prevent harm – Baseline and Post-intervention assessments
To assess intention to avoid peer sexual harassment, we used five items developed by Taylor and colleagues (Taylor et al., 2011). For example, “I can help prevent sexual harassment against peers at my school”. Items were measured on a four-point scale ranging from completely disagree (1) to completely agree (4) and summed for scores ranging from 5 to 20. To assess intention to avoid or prevent CSA, we crafted seven similar items. For example, “I know how to teach my friends about how to stop child sexual abuse”. Again, response options ranged from completely disagree (1) to completely agree (4) and were summed for scores ranging from 7 to 28. For both scales, higher scores indicated stronger intention to prevent or avoid harm. At time 0, Cronbach’s alpha was 0.86 for both scales.
Analytic Strategy
First, we examined equivalence of groups on demographic characteristics and prior exposure to CSA prevention concepts via chi-squared test for categorical variables (or Fisher’s exact test when cell counts were small) and independent sample t-tests for continuous variables (see Table 1). Results indicated significant between-groups differences on two variables (minoritized status and grades). Next, we examined whether RBYC exerted effects on outcomes between time 0 (baseline) and time 1 (post-RBYC) via generalized linear mixed models (GLMM), adjusting for the two significant differences in demographic characteristics. This regression approach is appropriate for modeling data that are measured over time and are not normally distributed (Bono et al., 2021; Lo & Andrews, 2015). In GLMM, a significant interaction of group (Intervention vs. Waitlist) and time (0 and 1) variable indicates an intervention effect. Thus, we created a categorical variable with a total of four categories: two categories indicating the Intervention group at time 0 and time 1, and two categories indicating the Waitlist group at time 0 and time 1. This categorical variable was entered in all the models as the primary predictor. The reference group was the Intervention group at time 0. The expected intervention effect would be observed between the Intervention group from time 0 to time 1; however, no change was expected for the Waitlist group in comparison to the reference Intervention group at either time point. All outcome measures had discrete values, were left censored at zero, and were skewed (i.e., did not meet the normality assumptions as per Shapiro-Wil, Kolmogorov-Smirnov, and Cramer-von Mises tests). A GLMM with AR(1) variance-covariance structure, log link function, Poisson distribution, and random effects due to repeated measures at two time points of the subjects was tested for eight of the nine outcomes. The Peer Sexual Harassment Behavior outcome was zero inflated right skewed (i.e., had many zero response values). Thus, we used a Zero Inflated Poisson GLMM with random effects to measure the intervention effect in this outcome (Bono et al., 2021; Fitzmaurice et al., 2012). All data preparations and statistical analysis were conducted in SAS software version 9.4.
Missing data ranged from 12% to 21% across time 0 and time 1. Particularly, missingness was higher in the waitlist group (30% vs. 18% at time 0, and 26% vs. 12% at time 1). To investigate the robustness of results due to missing data, we conducted sensitivity analysis for each outcome with all available data, including participants with data missing from one assessment timepoint. Results were consistent with results from analyses that included only those participants with data at both assessments. Except where noted, we present only those results from analyses that excluded participants with data missing from either time point. Unadjusted models (models without minoritized status and grades covariates) were also tested to see the direct intervention effect of the RBYC program.
Results
Characteristics at Baseline
In Table 1 we summarize demographic information and present results of chi-squares and t-tests. Groups differed on the race and ethnicity variable and on the typical grades they reported receiving on their report card. Relative to students in the Waitlist group, students in the Intervention group were more likely to identify as White (0% vs. 18%, respectively) and to indicate earning mostly As and Bs on their report card (37% vs. 68%, respectively). We adjusted for these factors in our analyses. Most participants (69%) reported that a parent or caregiver had ever talked with them about CSA and groups were equivalent on this item.
Change in Outcomes Over Time
Results of Between-Groups Analyses Analyzed via Adjusted Generalized Linear Mixed Models with Log Link and Poisson Distribution.
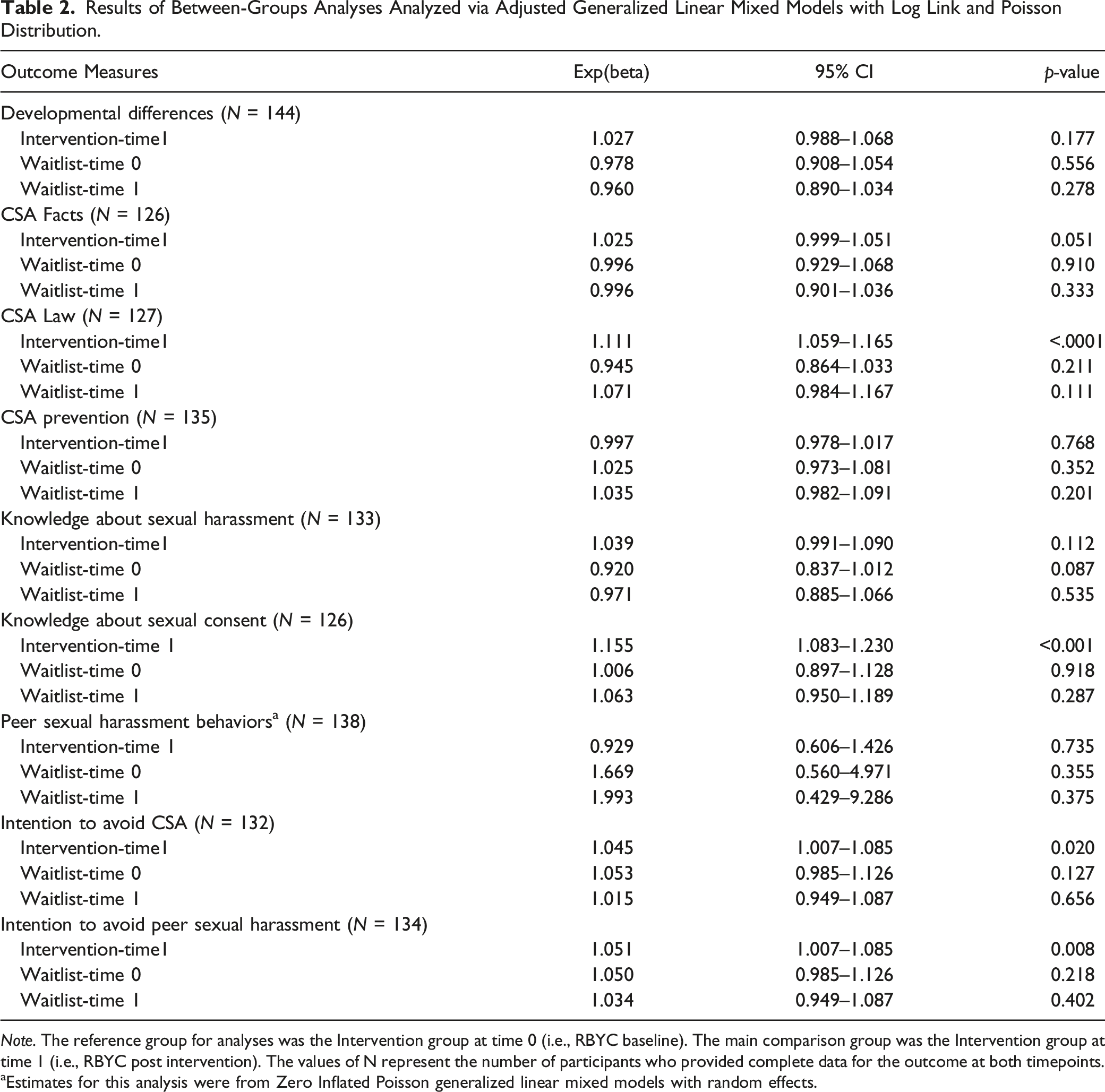
Note. The reference group for analyses was the Intervention group at time 0 (i.e., RBYC baseline). The main comparison group was the Intervention group at time 1 (i.e., RBYC post intervention). The values of N represent the number of participants who provided complete data for the outcome at both timepoints.
aEstimates for this analysis were from Zero Inflated Poisson generalized linear mixed models with random effects.
Developmental differences
This outcome was not significantly associated with the RBYC program.
Knowledge about CSA and related concepts
Groups differed significantly on two of the five subscales that assessed students’ knowledge of CSA and related laws and concepts. The RBYC program was associated with a significant increase (improved accuracy) on CSA Law (p < .0001) and Sexual Consent (p < .0001). In addition, the increase on CSA Facts approached significance (p < .051). Given that this was an initial pilot test with a small sample, the adjusted models may be a bit conservative. Sensitivity analysis indicated the RBYC program was associated with a significant increase in CSA Facts (unadjusted full sample: p < .048, adjusted all available cases: p < .03). There were no significant differences on the CSA Preventive Strategy or the Knowledge about Sexual Harassment subscales.
Peer sexual harassment behaviors
This outcome was not significantly associated with the RBYC program, likely owing to the preponderance of zero responses for the full sample at both Baseline and Post-RBYC (71% and 75%, respectively).
Behavioral intention to avoid or prevent harm
RBYC was significantly associated with increased intention to avoid or prevent problem sexual behavior against younger children (p < .020). Likewise, RBYC was also significantly associated with increased intention to avoid or prevent peer sexual harassment (p < .008).
Discussion
This study reports on the development and initial evaluation of a school-based program designed to prevent the onset of CSA by young adolescents against younger children. Previously published results from student, parent, and educator focus groups (pre-intervention) and interviews with individual educators (post-intervention) supported interest in and utility and feasibility of RBYC (Ruzicka et al., 2021). Results from this initial pilot RCT were also promising. As hypothesized, RBYC was associated with improved understanding of CSA facts, related laws, and the critical concept of sexual consent. Importantly, RBYC was also associated with increased intention to prevent or avoid CSA against younger children and increased intention to prevent or avoid peer sexual harassment. Lack of knowledge and impulsivity are two risk factors identified for CSA among adolescents (Chaffin, 2008; Letourneau et al., 2017). Improved knowledge about what constitutes sexual abuse, related laws, and concepts such as consent should counter lack of knowledge, while increased behavioral intentions to prevent or avoid perpetrating harm may counter impulsivity. Effectively addressing these and other proximal risk factors may be one method for preventing sexual abuse by adolescents against younger children and peers.
We did not find evidence of improved knowledge of developmental differences between adolescents versus younger children or of CSA prevention strategies. While it is possible that RBYC simply did not effectively address these two areas, it is also true that we created questions to measure knowledge about developmental differences and CSA prevention strategies and our questions may have been insensitive to change. Moreover, the majority of our student participants reported having previously received messaging about CSA prevention from parents or other caregivers, which might have contributed to these null results. We also did not find evidence of improved knowledge of sexual harassment or of reductions in peer sexual harassment behaviors. We used well-validated questions from Taylor and colleagues' work (Taylor et al., 2011) to assess for change in knowledge about peer sexual harassment, so poor measurement is not to blame. Rather, we think it likely that RBYC, which addresses peer sexual harassment in just one session, may not be robust enough to effect change in knowledge of peer sexual harassment. We also did not find differences in peer sexual harassment behaviors, likely due to the fact that few students reported engaging in such behaviors at either assessment time point. As noted above, we did find differences in behavioral intention to avoid or prevent peer sexual harassment, so including even limited content on this topic, within the context of a broader focus on CSA against younger children, does appear to have some merit.
This study was characterized by several strengths and limitations. Random assignment at the school level was used, which reduced the risk of intervention contamination. However, we did not have sufficient resources to recruit enough schools to analyze results at the school level of nesting or to follow students across a longer period of time. We utilized a waitlist randomized design, which improved engagement with partner schools - all of whom desired the intervention - but which also constrained our ability to conduct a longer-term follow-up of intervention effects. We were delighted that four schools in the target community were willing to partner with us on this project; however, that also meant that the study was conducted solely in urban schools in a single district, which impacts generalizability of findings. The most substantial limitation was our reliance on newly-generated or adapted items and scales to assess outcomes, some of which were characterized by disappointingly low scale reliability. There is a pressing need for psychometrically sound measures of CSA prevention outcomes (Tutty, 2000). Additional limitations include that this study relied solely upon student self-report (we did not have the resources to assess teacher- or parent-reported outcomes), that assessors and data analysts were not blinded, and that intervention delivery varied between schools (e.g., due to duration or availability of class periods), which may impact replicability of findings.
CSA prevalence rates are unacceptably high and stubbornly stable despite increased awareness and proliferation of victimization-focused prevention efforts (Marcantonio et al., 2022). Adolescents commit a substantial proportion of sexual offenses against younger children as well as against peers. Some adolescents with specific risk characteristics, such as sexual attraction to young children, might benefit from more intensive interventions such as the Berlin Project (Beier et al., 2016). However, our results, in combination with results from evaluations of two other school-based programs, Shifting Boundaries (Taylor et al., 2015) and Safe Dates (Foshee et al., 1998; 2004) support the promise of universal school-based perpetration-focused prevention strategies. RBYC is now fully developed and well-positioned for larger evaluation trials that could address the need for replicability as well as several limitations of this pilot study, including randomization at the school level, implementation in more geographically diverse settings, and evaluation across longer follow-up and of student, teacher, and parent-reported outcomes. We previously reported on support for RBYC from students, parents, educators, and administrators (Ruzicka et al., 2021) which counters the frequent criticism that school-based health promotion efforts expect too much of educators (Miller-Day et al., 2013). Nevertheless, future research should seek to identify the minimal amount of content necessary to effect change. In particular, we believe that combining elements from peer-focused and younger-child focused sexual abuse perpetration prevention interventions is one obvious strategy that should be tested, and might help improve the impact of RBYC on peer sexual harassment. Perhaps the clearest lesson from the current trial is the critical need for validated outcome measures. Despite all that remains to be done, we believe the results from this initial pilot trial suggest that RBYC is a promising prevention intervention that warrants such further investigation.
Supplemental Material
Supplemental Material - Responsible Behavior With Younger Children: Results From a Pilot Randomized Evaluation of a School-Based Child Sexual Abuse Perpetration Prevention Program
Supplemental Material for Responsible Behavior With Younger Children: Results From a Pilot Randomized Evaluation of a School-Based Child Sexual Abuse Perpetration Prevention Program by Elizabeth J. Letourneau, Cindy M. Schaeffer, Catherine P. Bradshaw, Amanda E. Ruzicka, Luciana C. Assini-Meytin, Reshmi Nair, and John R. Thorne in Child Maltreatment
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Child Health and Human Development under grant HD083704-01A1 (Elizabeth J. Letourneau, Principal Investigator).
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.