
Abstract
Background:
This manuscript explores the silent yet urgent crisis of suicidal ideation and suicide within the nursing profession. Despite being one of the most trusted and essential health care roles, nurses face disproportionately high risks for psychological distress, moral injury, and suicide.
Aims:
The paper aims to synthesize existing evidence on prevalence, risk factors, and theoretical frameworks to guide prevention and intervention efforts, while emphasizing the critical need for trauma-informed, organizational, and policy-level responses.
Methods:
Using Joiner’s Interpersonal Theory of Suicide, the Job Demand–Control–Support (JDCS) model, and trauma-informed care (TIC) principles, the manuscript illustrates how feelings of burdensomeness, thwarted belonging, and exposure to trauma converge to elevate suicide risk.
Results:
Key contributing factors to nurse suicide include chronic occupational stress, compassion fatigue, workplace bullying, moral distress, and limited autonomy, all compounded by a pervasive stigma around mental health help-seeking. A poignant case study underscores how institutional silence and lack of systemic support following medical errors can lead to devastating outcomes. Barriers such as fear of licensure consequences and lack of confidential services further discourage early intervention.
Conclusions:
The suicide crisis among nurses necessitates a comprehensive, multi-level response. Nurse leaders must foster psychologically safe environments, promote peer support, and integrate mental health education into all levels of practice. System-level changes—such as confidential reporting systems, national suicide surveillance, licensure reform, and culturally competent outreach—are essential to prevent further loss. Future research must examine longitudinal risk trajectories, intervention efficacy, and artificial intelligence (AI)-driven early warning tools tailored to the nursing workforce.
Introduction and Epidemiology
Suicide was the eleventh overall leading cause of death in the United States according to the most recent data (Centers for Disease Control and Prevention [CDC], 2025a; National Institute of Mental Health [NIMH], 2025). In specified age groups, the ranked cause of death by suicide was third in ages from 15 to 24, second in ages from 25 to 35, fourth in ages from 35 to 44, sixth in ages 45–54, and ninth in ages 55–64. Trends in suicide rates have ebbed and flowed over time, but appear to be rising during the COVID-19 pandemic. Suicide rates peaked in 2022 and may have decreased slightly in 2023 with preliminary data (CDC, 2025a). In comparison, the suicide rate in the United States was nearly double the homicide rate in the same data set from the CDC (2025a). These rankings reflect the typical ages of employed adults. In all adults, the age-adjusted suicide rate per 100,000 population was 14.2 in 2022 (CDC, 2025a). However, health care workers, specifically registered nurses, health care support workers, and health technicians, had the most risk with rates between 15.6 and 21.4, while non-health care workers were 12.6 per 100,000 (Olfson et al., 2023).
Nurse suicide is well-documented. Davidson’s et al., (2020) study of nurse suicide revealed that both male and female nurses were more likely to complete suicide than an age and gender matched non-nurse group. Some data suggest that male rates may be similar to male non-nurse rates, but Davidson’s et al., (2024) study confirmed that female nurses are at higher risk than non-nurses. This may be related to increased incidence of mood disorders in nurses (Davidson et al., 2024; Olfson et al., 2023) and increased incidence of burnout (Melnyk et al., 2025; Nguyen et al., 2025). Patient care, safety, and outcomes depend on the fitness of health care providers, with nurses making up the largest employment group.
Despite years of data, calls for action from various nursing groups, health care organizations, and governmental agencies, and attempts to address the issue, it remains a crisis and a threat to future nurses. In recent years, many prevention programs have been implemented, but nurses are not as likely to attend or complete the programs for multifactorial reasons. Most recently, the American Academy of Nursing (AAN; 2025) indicated the need for policy dialogue to discuss the growing nurse suicide crisis and the lack of adequate research, evidence, and policies to support the continued aim for healthier work environments and increased well-being among the nursing workforce. Specifically, the AAN indicates a necessary partnership across psychiatric, mental health, and substance use experts, as well as the Acute and Critical Care experts on this dialogue. The purpose of this paper is to explore precipitating factors, theoretical frameworks, interventions, and propose solutions for the continuing problem using a case example.
Contributing Risk Factors
The nursing occupation is both physically and psychologically demanding. Workplace conditions often consist of high patient ratios, low staffing, high-stress situations, and difficult workplace relationships, which include bullying in some situations. This often leads to occupational burnout, as well as moral distress and compassion fatigue. Workplace bullying, which has been noted in up to 30.6% of nurses globally, has been associated with an increased risk of suicidal ideations and attempts (Lu et al., 2022).
Globally, nurses are more prone to die by suicide through self-poisoning, as compared to the general population, which more commonly utilizes firearms in the United States, and hanging or strangulation in the United Kingdom (Groves et al., 2023; Kreuze et al., 2025b). The presence of medications such as opioids, benzodiazepines, barbiturates, and antidepressants is found more commonly among health care clinicians (nurses, physicians, etc.) who die by suicide versus the general population (Davis et al., 2021). This might suggest that the risk of self-poisoning may be increased among health care workers as a result of access to such medications.
Comorbid psychiatric conditions appear to be a contributing risk factor in nurses who have died by suicide. In a study by Groves et al. (2023), 90.5% of nurses who die by suicide are found to have a psychiatric condition, 38.1% are found to have a personality disorder, and 38.1% have both a psychiatric condition and a personality disorder. Post-traumatic stress disorder (PTSD) has also been found to be a significant risk factor for death by suicide among nurses (Doherty, 2025). Notably, among nurses who have died by suicide in multiple countries, the most common psychiatric condition appears to be depression (Ariapooran et al., 2022; Groves et al., 2023).
Burnout has long been a factor in poor mental health among nurses, predating the COVID-19 pandemic by decades. It is believed that the rate of burnout among the nursing profession is as high as 45% to 55% (Rushton & Boston-Leary, 2022). Burnout significantly contributes to higher rates of anxiety, depression, substance use disorders, and suicide. The COVID-19 pandemic is believed to have further worsened the rates of anxiety, posttraumatic stress disorder, depression, insomnia, burnout, and suicide among nurses, with over 50% of nurses under the age of 25 reporting symptoms of depression (Ariapooran et al., 2022; Bergman & Rushton, 2023).
Barriers to Seeking Help
Nurses are an integral part of the U.S. health care system and are the largest group of health care workers. Unfortunately, they are often left feeling alone in their emotional turmoil. Fear of professional consequences, concerns with licensing and credentialing, and lack of institutional support prevent nurses from seeking mental health care services. Stigma surrounding seeking out mental health care services also prevents nurses from asking for help, even after they have determined that they need help (Bergman & Rushton, 2023).
The nursing profession has cultivated a culture that portrays that nursing is not for the weak or tender-hearted. In nursing, only the strongest survive, and it is often viewed as a sign of weakness for a nurse to seek out mental health assistance (Bergman & Rushton, 2023). An expectation of perfectionism within the profession further drives this stigma, as well as the high burnout rates (Rushton & Boston-Leary, 2022). As much as the profession has pioneered destigmatizing mental health within the general population, much work still needs to be done to destigmatize mental health within the nursing community. Nurses are often unsupportive of each other, and harsh work environments, which include gossip and bullying, further prevent nurses from seeking out mental health care resources (Edmonson & Zelonka, 2019).
Theoretical Frames
Interpersonal Theory of Suicide
Suicidal desire arises when individuals simultaneously feel thwarted belongingness (a sense of social disconnection) and perceived burdensomeness (a belief that one is a burden to others) (Sadri Damirchi et al., 2019). When nurses feel isolated or alienated from peers and believe they are harming others (for example, feeling incompetent or guilty about patient care), these constructs can fuel suicidal thoughts. A seminal study applying this model to nurses found that higher levels of thwarted belongingness and burdensomeness together accounted for nearly half of the variance in nurses’ suicidal ideation (Sadri Damirchi et al., 2019).
In practical terms, a nurse who works long shifts with little peer support may feel lonely (thwarted belongingness) and exhausted from heavy responsibilities (perceived burdensomeness), greatly increasing suicide risk. Empirical evidence supports this; specifically, during the COVID-19 pandemic, German nurses who reported greater perceived burdensomeness (feeling like a burden to family or society) were significantly more likely to endorse recent suicidal ideation (Höller & Forkmann, 2022). Moreover, these interpersonal feelings often co-occur with despair. As Sadri Damirchi et al. (2019) summarize, feeling like a burden induces self-hatred and, when combined with loneliness, the combination of these two structures leads to the formation of suicidal ideation in nurses.
Joiner’s third construct, acquired capability for suicide, is also relevant. Notably, repeated exposure to patient death and suffering can habituate nurses to pain and fear of death, potentially enabling lethal self-harm in those with suicidal desire.
Job Demand–Control–Support Model
The Job Demand–Control–Support (JDCS) model characterizes work stress in terms of job demands, decision authority (control), and social support. High demands (e.g., workload, time pressure) coupled with low control (little autonomy) and low support (poor coworker/manager support) create “high-strain” jobs that predict negative outcomes such as burnout and depression (Christiansen et al., 2024). Nursing is prototypical of this risk as nurses often face relentless demands (short-staffed wards, long or erratic shifts) while having limited control over schedules or care decisions, and sometimes experience low social support (e.g., managerial neglect or bullying) (Alnajdawi et al., 2024). For example, an emergency nurse working 12-hour shifts with multiple critical patients, little input into staffing decisions, and inadequate colleague support epitomizes a high-strain environment. Research confirms the impact of such strain on suicidality; specifically, in a recent cross-sectional study of physicians and nurses, measures of job strain (high demands with low control/support) correlated positively with suicidal ideation (Alnajdawi et al., 2024). In that Jordanian study, suicidal ideation was higher among health care staff reporting high psychological demands and low job satisfaction, consistent with the JDCS model’s prediction that excessive workload and low autonomy can erode well-being.
In nursing-specific terms, factors like understaffing and lack of decision-making autonomy—core JDCS stressors—have been linked to burnout and increased suicide risk in nurses (Christiansen et al., 2024). Thus, the JDCS framework helps explain how organizational conditions amplify nurses’ suicide risk: chronically high demands and lack of control/support can engender helplessness, depression, and ultimately suicidal thoughts.
Trauma-Informed Care Principles
Trauma-informed care (TIC) is an organizational approach that recognizes the widespread impact of trauma, acknowledges how traumatic experiences influence individuals’ beliefs and behaviors, and seeks to resist re-traumatization by promoting safety, trust, and empowerment (Dawson-Rose et al., 2023). In a trauma-informed system, staff are trained to identify trauma symptoms and to create policies and practices that provide psychological safety and support (Dawson-Rose et al., 2023). Nurses occupy roles with frequent exposure to trauma where they witness patient suffering, death, violence, and sometimes make split-second decisions with life-or-death consequences. These experiences can cause vicarious trauma and moral injury (psychological distress from actions that conflict with one’s values).
Trauma-informed principles applied to nurses emphasize the need for organizational support—for example, routine debriefings, peer support, and accessible mental health resources—to address cumulative trauma and prevent burnout. Specifically, Dawson-Rose et al. (2023) note that nurses experience vicarious trauma and secondary traumatic stress on the job, and that a trauma-informed approach at the hospital level could better provide for nursing staff suffering from burnout and exhaustion. In practice, a trauma-informed nursing unit might ensure transparent communication, allow choices in scheduling when possible, and normalize help-seeking after critical events. Failure to do so can exacerbate risk (Fleishman et al., 2019). Recent evidence shows that health care workers’ moral injury is strongly linked to suicidal ideation. In one longitudinal study of Chinese health professionals, high moral injury scores (reflecting exposure to ethical-violating situations and trauma) increased the odds of suicidal ideation by nearly fivefold (He et al., 2023). This suggests that when nurses’ traumatic stresses are unaddressed, their accumulated emotional burdens can translate into suicide risk. By contrast, a trauma-informed workplace that acknowledges nurses’ own trauma and promotes healing—aligning with the Substance Abuse and Mental Health Services Administration’s six principles of safety, trustworthiness, peer support, collaboration, empowerment, and cultural sensitivity (Dawson-Rose et al., 2023)—may mitigate factors like chronic stress and isolation that contribute to suicidal thoughts.
Integrative Perspective
These three theoretical lenses converge on the notion that nurses’ suicide risk is multifactorial. Interpersonal theory highlights internal states (feeling isolated or burdensome), JDCS highlights external work conditions (excessive demands, low control/support), and TIC highlights the impact of unprocessed trauma. For example, a nurse who feels like a burden to their family (interpersonal) may be more vulnerable if the hospital unit offers no workplace support or autonomy (JDCS), and if they have endured repeated traumatic patient care without organizational acknowledgment (lack of TIC). Conversely, interventions that integrate these perspectives—such as improving staffing levels (reducing demands), enhancing nursing autonomy and peer support, and providing trauma-focused debriefing—address both the work stressors and the emotional experiences linked to suicide risk (Alnajdawi et al., 2024). In sum, applying the interpersonal theory, the JDCS model, and trauma-informed principles together provides a comprehensive framework for understanding and preventing suicidal ideation in nurses. Each model underscores different but complementary pathways through which the profession’s burdens can translate into self-harm risk.
Case Study: A Silent Loss—The Death of a Pediatric Nurse Following a Medication Error
Megan, a 29-year-old pediatric intensive care nurse, had been working at a major urban children’s hospital for just under five years. Known by her peers as compassionate, detail-oriented, and deeply committed to her patients, Megan often volunteered for complex cases that required both technical skill and emotional presence. Families frequently requested her by name due to her gentle bedside manner and calm communication during crises.
One afternoon, during a high-acuity shift marked by simultaneous admissions, equipment shortages, and a 30% shortfall in staffing, Megan was assigned to a critically ill 4-year-old child in septic shock. During a rapid sequence of orders and multiple competing demands, she inadvertently administered potassium chloride, intended for slow infusion, via IV push. The error was discovered too late. The child experienced sudden cardiac arrest and, despite resuscitation efforts, could not be revived.
A subsequent root cause analysis identified multiple system-level contributors: ambiguous medication labeling, a malfunctioning override system in the automated dispensing unit that failed to flag high-alert medications, absence of a mandated secondary verification process, and organizational normalization of unsafe workload ratios. While these findings underscored system failures, they did little to address the immediate human and ethical fallout.
In the hours following the event, Megan’s professional and human rights, specifically, her rights to due process, psychological safety, dignity, and nonpunitive treatment, were not fully upheld. Although her supervisor initially offered verbal reassurance, Megan was escorted off the unit, placed on immediate administrative leave, and instructed not to discuss the incident with colleagues. These actions, though framed as procedural, left her isolated and implicitly criminalized. No just-culture framework was applied, and she was not offered representation, peer accompaniment, or a formal explanation of her rights regarding investigation, confidentiality, or support services.
Megan began showing clear signs of acute psychological distress: profound guilt, insomnia, panic symptoms, social withdrawal, and intrusive self-blame. While she received a brochure for the Employee Assistance Program (EAP), she declined to use it, expressing fear that seeking mental health care could threaten her licensure or be used against her in institutional review. This fear reflected long-standing cultural stigma within the profession and inadequate institutional communication about protections for help-seeking nurses.
Critically, no second-victim response protocol, crisis intervention team, or trauma-informed support structure was initiated, despite Megan’s clear status as a clinician involved in an adverse event. She did not receive a structured debriefing, a wellness check, or even a follow-up call from leadership in the days that followed. The absence of these safeguards represented a significant lapse in institutional responsibility to uphold her right to psychological support, equitable treatment, and protection from harm.
On her scheduled day off, one week after the incident, Megan drove to the hospital parking garage, returning to the place where her life had become defined by unremitting guilt, and died by suicide using carbon monoxide poisoning. In her note, she wrote: I loved my patients, and I failed one of them. I can’t live with that. The tragedy sent shockwaves through the staff and the broader hospital community. Many nurses experienced prolonged grief, vicarious trauma, and fear that they too could become casualties of a system that punished error rather than preventing it. Although leadership provided brief unit-based debriefings, no long-term psychological support, policy revision, or formal second-victim program was introduced.
Megan’s death was not formally reported to national nurse suicide surveillance systems, remaining another uncounted loss in a profession facing silent suffering.
This case reveals a painful intersection of system failure, human vulnerability, and the erosion of professional rights. Megan’s experience demonstrates how acute psychological trauma following medical error can escalate rapidly, particularly when institutions lack just-culture principles, transparent investigative processes, mental health protections, and trauma-informed leadership responses. The absence of safeguards not only contributed to her suicide but also reflects a broader need to integrate human rights protections into organizational policies governing adverse events, clinician wellness, and suicide prevention.
Implications for Nursing Practice and Leadership
Nurse leaders hold a pivotal role in suicide prevention by shaping the work environment, identifying at-risk staff, and advocating for mental health visibility and support. Early recognition of suicidal ideation requires leaders to be trained in trauma-informed communication, psychological first aid, and how to interpret behavioral warning signs such as withdrawal, decreased job performance, or expressions of hopelessness (West et al., 2020). Nurses may not openly disclose distress due to stigma or fear of licensure consequences; therefore, leaders must foster trust and confidentiality in all mental health-related interactions (Davidson et al., 2021).
A critical distinction for leaders lies in recognizing the difference between acute psychological crises and chronic, cumulative distress, each requiring different organizational responses. Acute crises often follow practice errors, near misses, or traumatic clinical events. These situations may provoke intense shame, fear of punitive action, or profound moral emotions, leaving the nurse in immediate need of structured support. Rapid interventions, such as immediate debriefings, psychological first aid, crisis counseling, and programs like the Resilience in Stressful Events (RISE) model (Connors et al., 2024), are essential to mitigate acute harm and prevent the onset of second-victim syndrome. These interventions are time-sensitive and designed to stabilize the clinician’s emotional functioning in the hours or days following an event.
In contrast, many nurses experience slow-building, longitudinal psychological strain related to persistent workplace stressors such as bullying, compassion fatigue, moral injury, chronic staffing shortages, thwarted belongingness, and institutional stigma around mental health help-seeking. These issues erode wellness over time, often invisibly, and increase risk for suicidality through cumulative emotional depletion and hopelessness (Galanis et al., 2024; Powell et al., 2024). Addressing chronic distress requires sustained leadership investment through workload redesign, supportive supervision, normalized mental health dialogue, longitudinal peer support, and intentional culture change.
Creating a psychologically safe workplace, one in which nurses feel supported, respected, and unafraid to voice concerns, is critical. Psychological safety has been strongly linked to decreased burnout and improved team cohesion (Edmondson & Lei, 2014). Nurse managers can foster such safety by encouraging open dialogue, validating emotional struggles, and leading debriefings after traumatic clinical events. Structured peer support programs, such as Code Lavender or trained peer responder models, have been shown to reduce symptoms of distress and promote resilience following critical incidents (National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine; Committee on the Future of Nursing 2020–2030, 2021). In addition to these approaches, the Resilience in Stressful Events (RISE) program, as previously mentioned, provides. For immediate, confidential emotional support to health care workers following adverse events and has demonstrated effectiveness in promoting coping, restoring professional functioning, and reducing the long-term psychological sequelae associated with workplace trauma (Connors et al., 2024). Including programs like RISE alongside Code Lavender reflects the growing recognition that tiered, trauma-informed peer support infrastructures are essential components of organizational well-being and clinician retention.
Confidential mental health services are another cornerstone of suicide prevention. Institutions should ensure that Employee Assistance Programs (EAPs) are robust, anonymous, and easily accessible. More importantly, they must be paired with culturally competent outreach, especially given that many nurses report mistrust in these services due to past breaches or perceived judgment (Melnyk et al., 2025).
In addition, integrating mental health training into nursing education—both at the undergraduate and professional development levels—is essential. Curricula should include modules on stress response, burnout, moral distress, and suicide risk awareness, framed within trauma-informed and peer-supportive approaches. Ongoing clinical education should also prepare leaders to assess unit wellness and intervene when patterns of distress or turnover arise.
Implications for Policy and System-Level Change
System-level reform is needed to address suicide risk among nurses comprehensively. Hospitals must first implement internal reporting mechanisms that allow for anonymous flagging of mental health crises, behavioral changes, or near misses that may indicate distress. These systems should be supported by trained mental health liaisons or designated wellness officers who ensure follow-up and support without punitive action.
Beyond individual facilities, the absence of national surveillance and mandatory reporting systems remains a significant gap. Unlike other high-risk professions, nurse suicide is not systematically tracked in the United States, which limits prevention efforts and funding allocation. National-level tracking, modeled on the CDC’s National Violent Death Reporting System (NVDRS), could generate clearer epidemiological data to inform targeted interventions (CDC, 2025b).
State-level legislation also plays a role. Boards of Nursing should revise outdated requirements around mental health disclosure for licensure and renewal. Studies show that fear of professional repercussions deters nurses from seeking help (Davidson et al., 2020). Reforming these policies to align with ADA protections and allow for conditional or monitored practice—rather than punitive suspension—could dramatically improve help-seeking behavior.
Funding mechanisms must prioritize nurse-specific interventions, such as resilience programs, mindfulness-based cognitive therapy, and unit-level staffing improvements. Federal and philanthropic investment in these areas can offset institutional budget constraints, especially in rural and under-resourced systems. Efforts such as the American Association of Colleges of Nursing’s Healthy Nurse, Healthy Nation™ initiative provide national infrastructure for such change and can be leveraged to mobilize cross-sector partnerships (American Nurses Association, 2024; Healthy Nurse, Healthy Nation, n.d.).
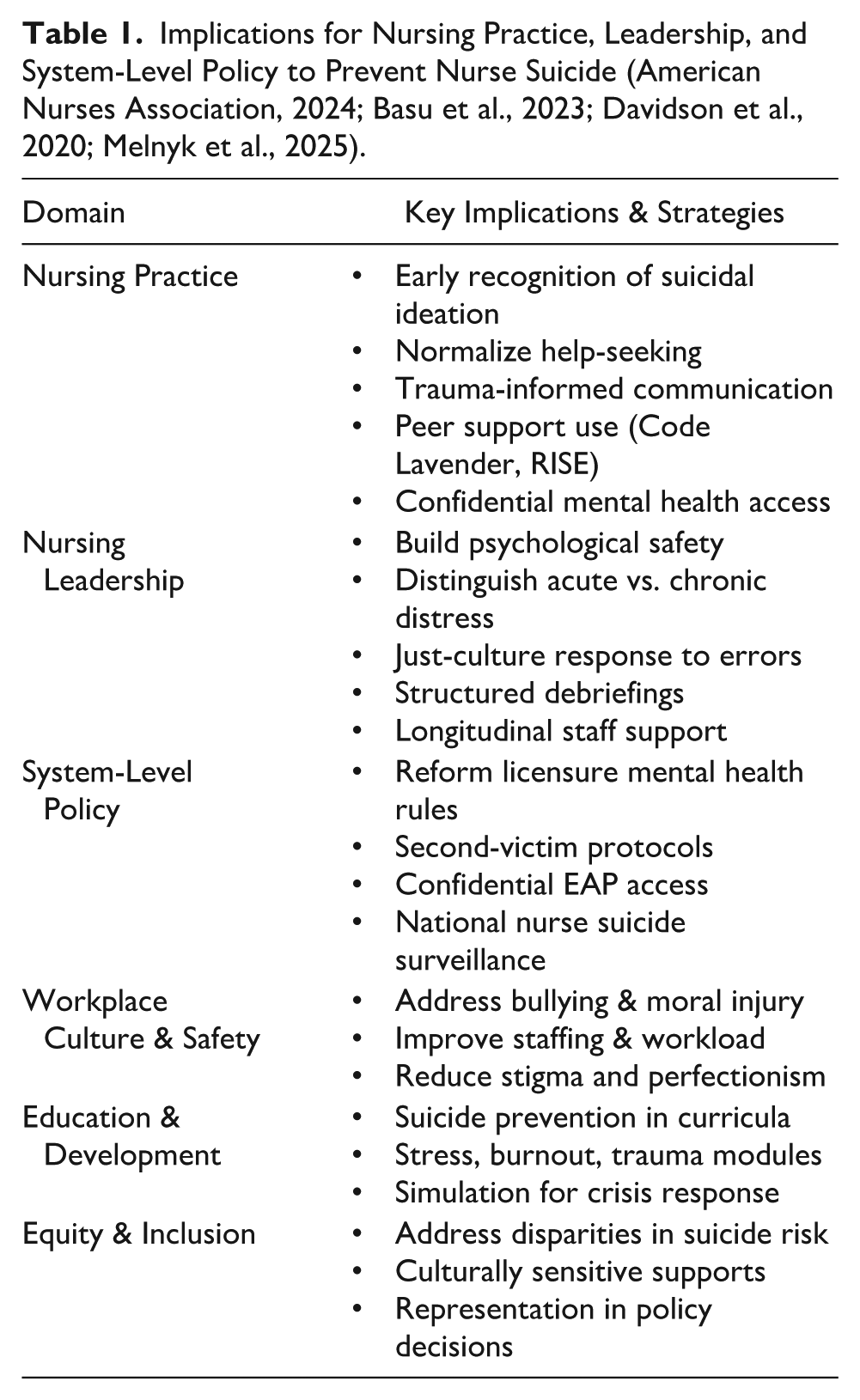
Finally, institutional and regulatory policy must address intersectionality and equity within nurse suicide prevention. Data and programs must account for variation across gender, race, sexual orientation, and job roles. For example, studies have shown disproportionately high stress and suicide risk among male nurses and nurses of color—groups often left out of mainstream interventions (Melnyk et al., 2025) (Table 1).
Implications for Nursing Practice, Leadership, and System-Level Policy to Prevent Nurse Suicide (American Nurses Association, 2024; Basu et al., 2023; Davidson et al., 2020; Melnyk et al., 2025).
Recommendations for Future Research
Future research must address critical knowledge gaps surrounding suicidal ideation and suicide among nurses across their career trajectories. Longitudinal studies are particularly needed to map how suicide risk evolves across the nursing continuum—from pre-licensure students to bedside clinicians, administrative leaders, and academic faculty. Emerging data suggest that burnout and suicidal ideation manifest differently at various career stages, with bedside nurses often reporting emotional exhaustion and moral distress, while faculty and leaders cite isolation and institutional pressure (Davidson et al., 2021; Melnyk et al., 2025). Understanding these nuances through prospective, cohort-based studies will help target prevention efforts more precisely.
There is also an urgent need to evaluate suicide prevention interventions tailored specifically to the nursing profession. While some programs, such as mindfulness training, resilience workshops, or Code Lavender initiatives, show promise, few have been rigorously tested in nursing populations using randomized controlled trials (West et al., 2020). Intervention research should examine not only outcomes like reduction in suicidal ideation or increased help-seeking but also feasibility and long-term sustainability within clinical and academic settings.
Additionally, culturally sensitive approaches must be prioritized. Suicide risk among nurses is not uniform; recent findings indicate that racial, ethnic, gender, and LGBTQ+ minority nurses experience unique stressors—including discrimination, identity-related stigma, and exclusion—that may compound risk (Melnyk et al., 2025). Future studies should explore how cultural background, social determinants of health, and intersectionality influence suicide risk and resilience. Designing inclusive, equity-focused suicide prevention strategies is essential to ensure all nurses benefit from supportive environments and tailored interventions.
Finally, advancements in artificial intelligence (AI) and machine learning offer promising tools for early risk detection. Predictive analytics, when used ethically and with nurse consent, could identify individuals at elevated risk based on electronic health record usage patterns, absenteeism, and behavioral indicators (Rihan, 2025). Future research should assess the accuracy, clinical integration, and privacy safeguards of such technologies in nursing contexts. These tools could eventually support proactive outreach and reduce missed opportunities for intervention. Together, these lines of inquiry will help build a more robust evidence base to understand, prevent, and ultimately reduce suicide in the nursing profession.
Conclusion
The evidence presented underscores that suicide among nurses is not only a personal tragedy but also a systemic crisis with wide-reaching implications for the profession and health care delivery at large. Nurses face unique occupational hazards, including moral injury, compassion fatigue, workplace bullying, and exposure to trauma, which are compounded by stigma and fear of professional repercussions when seeking help. Case examples, such as Megan’s tragic loss, highlight how silence and lack of systemic safeguards perpetuate preventable outcomes. Recognizing these complex dynamics affirms the urgency for a paradigm shift in how the profession, institutions, and policymakers respond to suicide risk in nursing.
Addressing this crisis requires a multi-level strategy that integrates interpersonal, organizational, and policy-driven solutions. Trauma-informed care principles, coupled with frameworks such as the Interpersonal Theory of Suicide and the Job Demand–Control–Support model, provide actionable roadmaps for intervention. Nurse leaders must prioritize psychologically safe workplaces, foster peer support networks, and ensure confidential and culturally competent access to mental health resources. Equally vital are system-level reforms, including national suicide surveillance, licensure policy reform, and dedicated funding for prevention programs. Such efforts must not only respond to individual crises but also preemptively dismantle the organizational and cultural barriers that sustain nurse vulnerability.
Future directions must emphasize research, innovation, and equity in suicide prevention. Longitudinal studies can illuminate how suicide risk evolves across the career trajectory, while rigorous evaluations of nurse-specific interventions will strengthen evidence-based practice. Emerging technologies, including AI-driven early detection tools, hold promise for proactive prevention, provided they are implemented ethically and with safeguards for nurse privacy. Ultimately, the nursing profession must reclaim its own commitment to well-being by dismantling stigma, amplifying systemic accountability, and creating sustainable cultures of care for its workforce. Only through such comprehensive and compassionate action can we begin to reverse the silent crisis of suicide in nursing and honor the lives of those lost.
Resources for Nurses Experiencing Suicidal Thoughts or Emotional Crisis
Examples:
Footnotes
Author Contributions
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This is not a research study and did not include human subjects or any protected data. Case studies are fictitious albeit representative of actual situations.