
Abstract
Keywords
Depression disproportionately affects women, especially during the childbearing years (Villarroel & Terlizzi, 2020). Up to one in five women experience depressive symptoms during pregnancy (Yin et al., 2020). Antenatal depressive symptoms are likely to continue unabated postnatally (Suri et al., 2017) and follow a protracted, recurrent course throughout the parenting years (Freeman et al., 2018). Thus, depressed mood during pregnancy has far-reaching implications for women’s well-being throughout parenthood.
Depressed mood is also associated with hypothalamic–pituitary–adrenal axis dysregulation of the stress hormone cortisol (Pariante & Lightman, 2008). During pregnancy, cortisol plays a crucial role in regulating the cascade of physiological events that determine the timing of labor (Challis et al., 2001). Cortisol typically follows a dynamic daily pattern in which levels are high in the morning and gradually decline toward evening (Lovallo, 2005). A surge in cortisol shortly after waking, known as the cortisol awakening response, facilitates consciousness and energy mobilization for the day ahead (Clow et al., 2010). Although absolute cortisol levels rise threefold over pregnancy, the diurnal pattern of a morning awakening response followed by cortisol decline toward evening remains mostly unchanged (Duthie & Reynolds, 2013). Generally, more dynamic cortisol variation across the day (i.e., robust cortisol awakening response in the morning and low cortisol levels in the evening) is associated with better physical and mental health outcomes, whereas flatter diurnal cortisol patterns (no cortisol awakening response and high levels in the evening) are associated with worse physical and mental health outcomes (Adam et al., 2017). Antenatal depressive symptoms are associated with flattened, less dynamic cortisol rhythms, a weak or absent cortisol response to awakening, and higher evening cortisol levels (Epstein et al., 2020; O’Connor et al., 2014; Osborne et al., 2018).
Importantly, maternal cortisol levels that remain elevated in the afternoon/evening partially mediate adverse birth outcomes such as shorter length of gestation and preterm birth (Gillespie et al., 2017; Osborne et al., 2018). Evidence also suggests that a flattened pattern of diurnal cortisol during pregnancy (i.e., small cortisol awakening response and inadequate afternoon cortisol decline) are associated with altered stress reactivity in neonates after birth (Nazzari et al., 2020). These stress-related exposures may have long-lasting neurodevelopmental effects on the fetus, increasing the risk for behavioral and mental health disorders later in childhood (Van den Bergh et al., 2020) such as anxiety, depression, and attention-deficit hyperactivity disorder (Davis & Sandman, 2012; Graham et al., 2019; Zhu et al., 2015).
Women’s use of coping strategies to manage stress have been associated with differences in cortisol regulation. In adolescent girls, the use of active coping and social support are associated with a better diurnal cortisol rhythm and lower overall cortisol secretion (Guan et al., 2016; Sladek, Doane, & Stroud, 2017). Furthermore, various forms of social support buffer the cortisol response to acute social stress in controlled experiments (Sladek, Doane, Jewell, et al., 2017). Use of distraction as a coping strategy is associated with better cortisol recovery after an acute social stressor (Janson & Rohleder, 2017). On the other hand, higher use of disengaged/avoidant coping has been associated with flatter (less dynamic) cortisol rhythms and greater perceived stress, depression, and negative affect (Peters et al., 2020; Tull et al., 2005).
It is unknown whether coping strategies attenuate the physiological effects of depressed mood on cortisol dysregulation in pregnant women or how social context might shape the use of these strategies. Therefore, the purpose of this mixed-methods study was to examine patterns of coping strategies in pregnant women, whether any strategies moderate depression-related cortisol dysregulation, and how social context influences women’s coping strategies.
The selection of study concepts was informed by theories of stress and coping (Carver et al., 1989; Lazarus, 1999), whereby strategies for coping with stress are an essential component of emotional life (Lazarus, 1999). In this study, coping is conceptualized as a relatively stable trait (Carver et al., 1989), which is conditioned by social contexts and systems of power (Pinderhughes, 2017; Spencer, 2017). Social context here refers broadly to the structural, historical, and socioeconomic conditions within which people live and work. Specifically, some people’s experiences of being chronically subjected to oppression, discrimination, and social exclusion over the life course can shape strategies for responding to challenge (Pinderhughes, 2017). Thus, while we primarily focus on integrating individual-level biopsychosocial factors in this article, it is imperative to consider how such individual-level factors are situated within and conditioned by social contexts that offer differential access to opportunity, resources, and support over the life course.
Method
Design
This study used a convergent mixed-methods design (Creswell, 2014). The quantitative arm examined the moderating effect of coping on diurnal cortisol related to depressed mood. The qualitative arm helped contextualize the quantitative results. The two arms were collected concurrently and integrated during analysis. The two arms were integrated by using the quantitative results of the moderation analysis as a sensitizing framework for the qualitative analysis.
Setting and Participants
Women were recruited in 2016 from an urban women’s health clinic and were eligible to participate if they were pregnant with a single fetus, between the ages of 19 and 45 years, and English speaking. Women were excluded if they received a referral for care in a medically high-risk pregnancy clinic, had major pregnancy complications/existing medical issues, or regularly worked a night shift. A subset of participants (n = 20) were selected using maximum variation sampling to participate in qualitative interviews.
Initially, 75 women provided written informed consent to participate. Two participants voluntarily dropped out, and one was lost to follow-up. Two participants were excluded due to not meeting inclusion/exclusion criteria. Five participants did not return sufficient salivary biospecimens. Demographic characteristics of the final sample (N = 65) are shown in Table 1. The study was approved by the institutional review board affiliated with the recruitment site (#718-15-EP).
Demographics.
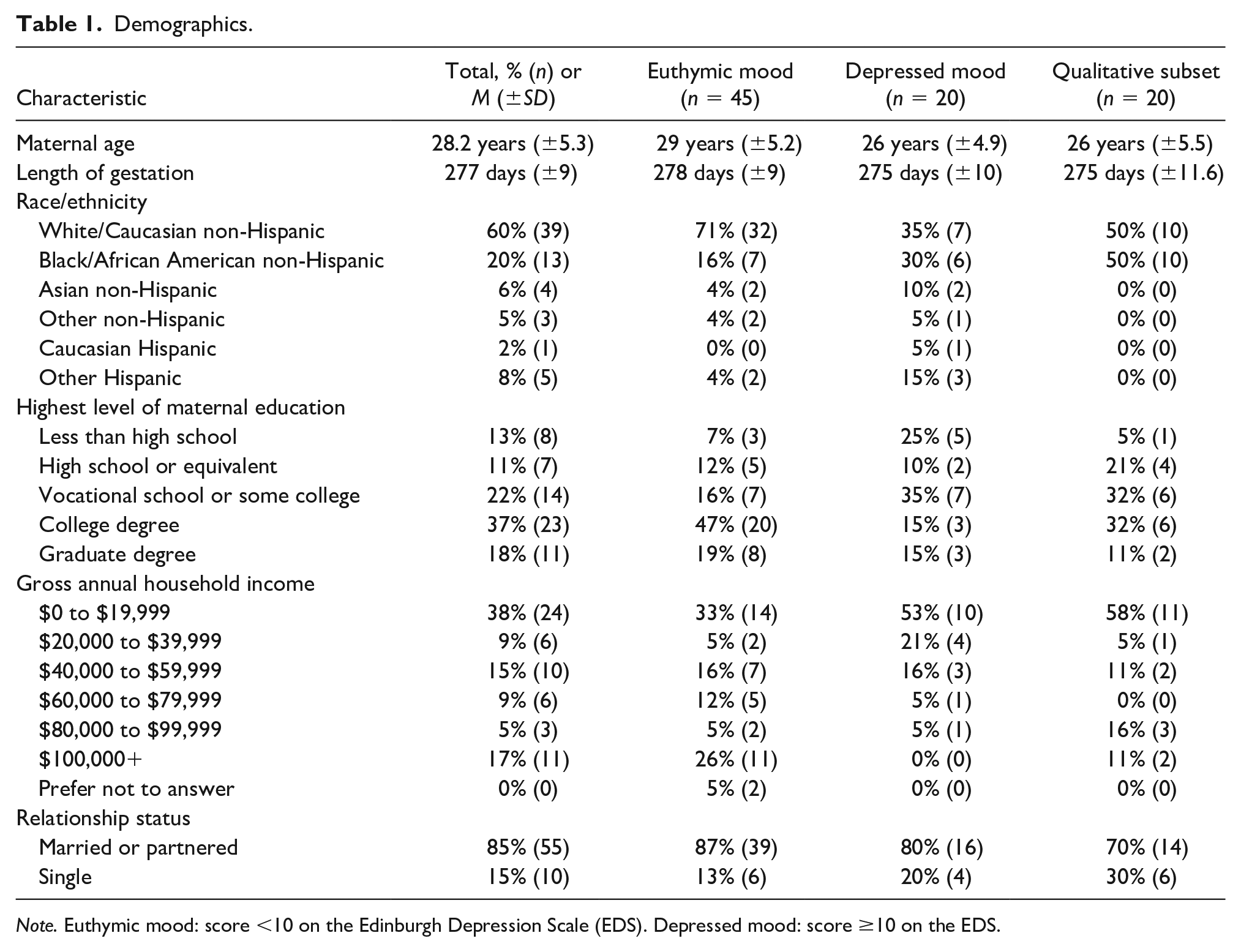
Note. Euthymic mood: score <10 on the Edinburgh Depression Scale (EDS). Depressed mood: score ≥10 on the EDS.
Measures
Edinburgh Depression Scale
The Edinburgh Depression Scale (EDS) is a 10-item scale that measures depressive symptoms over the past 7 days (Cox et al., 1987). Higher scores (range 0-30) represent greater severity of depressive symptoms. Internal consistency reliability (α = .84) was adequate in this sample. Predictive criterion validity (Composite International Diagnostic Interview–Depression) has been established (Bergink et al., 2011; Cox et al., 1987). Scores from the EDS were analyzed dichotomously as either below or above the cutoff (≥10). This cutoff has adequate sensitivity (70% to 86%) and specificity (84% to 96%) for detecting antenatal depression among diverse samples of pregnant women (Bergink et al., 2011; Tandon et al., 2012).
Brief COPE
The Brief COPE is a 28-item scale with 14 factors evaluating the frequency of coping strategies on a 4-point scale. A second-order, three-factor model demonstrating good fit in a sample of pregnant women was used in the analysis (Peters et al., 2020). The three factors had good internal consistency in this study: active coping (α = .88), disengaged coping (α = .75), and social support coping (α = .84). Active coping (12 items) is defined as efforts to mitigate a stressor (e.g., “I’ve been taking action to try to make the situation better”) and includes strategies of positive reframing, planning, humor, acceptance, and religion. Disengaged coping (10 items) is characterized by avoiding, escaping, or ignoring feelings of distress (e.g., “I’ve been giving up the attempt to cope”) and includes strategies of behavioral disengagement, denial, self-blame, venting, and self-distraction. Social support coping (4 items) includes strategies of emotional support (e.g., “I’ve been getting comfort and understanding from someone”) and instrumental support (e.g., “I’ve been trying to get advice or help from other people about what to do”).
Salivary Cortisol Collection
The collection and processing of salivary cortisol samples (n = 914) for this study have been described elsewhere (Epstein et al., 2020). Briefly, participants collected five saliva samples per day over 3 days and were instructed to skip any sampling times that were forgotten or missed. Collection times included immediately upon awakening (MTime 1 = 7:42 a.m.), 30 minutes after awakening (MTime 2 = 8:13 a.m.), before lunch (MTime 3 = 12:45 p.m.), before dinner (MTime 4 = 6:52 p.m.), and before bedtime (MTime 5 = 10:37 p.m.). Samples were processed in duplicate by enzyme immunoassay. Raw cortisol values were natural log-transformed due to nonnormality and were examined for extreme outliers. The cortisol awakening response and area under the curve (AUC) were calculated from the natural log-transformed values.
Qualitative Data
Semistructured interviews were conducted with a subset of participants (n = 20; see demographic characteristics in Table 1). Qualitative interview questions addressed women’s current and past stressors and inquired about strategies women have used to cope with stress and depressed mood. The qualitative sample included nine depressed women and 11 nondepressed women. Interviews were audio recorded (18-75 minutes) and professionally transcribed.
Data Analysis
Quantitative Analysis
Stepwise linear regression was used to identify the confounding variables of age, smoking, and antidepressant use. Other variables that were evaluated as confounders include education, income, gestational timing of cortisol collection, average time at awakening, sleep duration, and fetal sex. Spearman’s rank-order correlations were used to examine the biopsychosocial correlates of coping. Multiple linear regression was used to examine the main effects and interactive effects of coping on diurnal cortisol parameters. Post hoc analyses were conducted using independent t tests to examine unadjusted mean differences in cortisol levels between groups with a significant modifier effect. Although the samples size in the secondary analyses is small, the unadjusted mean differences can inform areas future areas of research. SPSS Statistics version 26 was used for all statistical analyses, with significance set at p < .05.
Qualitative Analysis
Transcripts were analyzed in ATLAS.ti using thematic analysis (Miles et al., 2014). The qualitative analysis was conducted subsequent to the quantitative analysis to contextualize the quantitative findings. A multiple-case sampling approach was used to stratify the transcripts based on participants’ depression and social support scores. Because social support coping was a significant modifier of the relationship between depressed mood and cortisol, “social support” was used as a sensitizing concept to focus the qualitative analysis. To more fully understand participants’ coping, focus was placed on identifying contextual factors that may have limited or hindered women’s use of social support. The first cycle of coding consisted of coding units of data with the a priori code of “social support.” Next, line-by-line focused coding used descriptive and in vivo codes to identify emergent patterns and themes within the data. The themes describe the intersection of social context with the variable of depressive symptoms to influence support seeking.
Results
Quantitative Findings
Depressive symptoms were positively correlated with greater use active coping (ρ = .36, p < .01) and disengaged coping (ρ = .57, p < .001), but not social support coping (ρ = .14, p = .26), indicating higher overall individual coping efforts among depressed women (Table 2). Black women reported greater use of active coping, t(51) = 2.27, p = .03, relative to White and Hispanic women. All three coping strategies were positively and moderately correlated. No coping strategies were directly correlated with any cortisol parameters. There were no discernable differences between disengaged and active coping in terms of the size or direction of relationship with any study variables (see Table 2). The overall diurnal cortisol trajectory was flatter among Black women due to the combined effect of lower morning cortisol levels and higher bedtime cortisol levels, t(63) = −2.91, p = .005. This effect remained even after controlling for depressive symptoms (adjusted R2 = .09, β = .33, t = 2.70, p = .01).
Zero-Order Spearman Correlation Between Primary Study Variables.
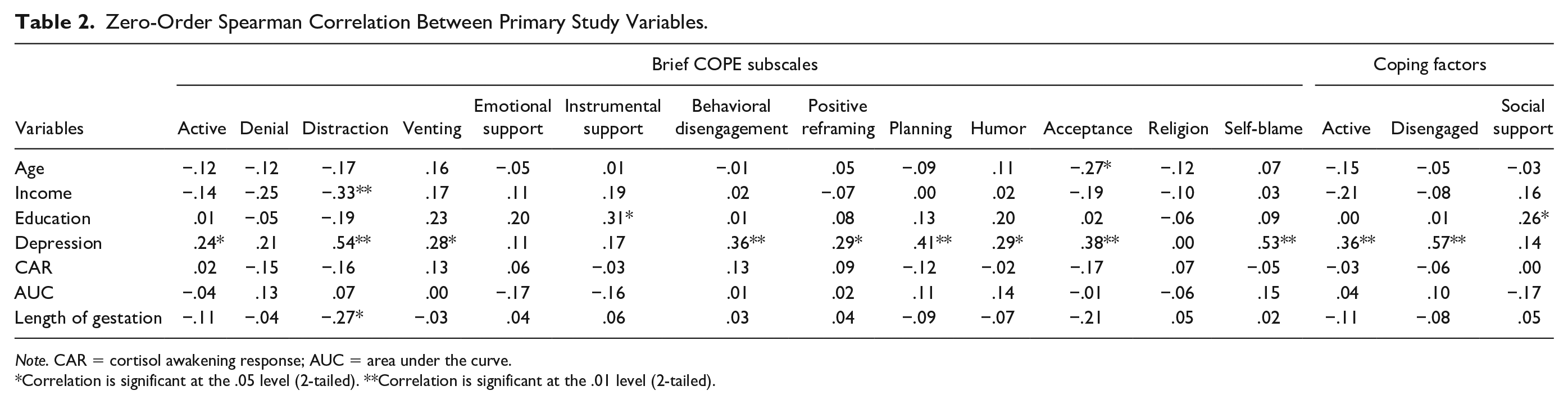
Note. CAR = cortisol awakening response; AUC = area under the curve.
Correlation is significant at the .05 level (2-tailed). **Correlation is significant at the .01 level (2-tailed).
Moderation Effects
Social support coping, but not active or disengaged coping, significantly moderated the relationship between depressed mood and cortisol. Social support coping was associated with lower bedtime cortisol levels among depressed women (adjusted R2 = .268, β = −.941, t = −2.032, p = .047). Greater use of social support coping was also marginally associated with a more robust cortisol awakening response in the morning among depressed women (adjusted R2 = .099, β = 1.016, t = 1.978, p = .053). This result was primarily due to lower awakening cortisol levels among depressed women who reported greater social support. When testing moderation effects on total average cortisol secretion (AUC) across the day, there were no significant interactions. Thus, the moderation effects on cortisol were specific to the time of day.
Post hoc Analysis
To better characterize the moderating effect of social support coping, mean differences in cortisol parameters were examined between depressed women reporting high social support (depressed–supported; n = 9) and low social support coping (depressed–self-reliant; n = 11). The depressed–self-reliant group (compared with depressed–supported) had a flatter, less dynamic diurnal rhythm characterized by a marginally higher awakening cortisol, t(18) = 1.93, p = .07, flatter cortisol awakening response, t(18) = −2.41, p = .03, higher bedtime cortisol, t(18) = 2.71, p = .02, and higher total daily cortisol secretion (AUC), t(18) = 2.23, p = .048 (Figure 1). Notably there were no differences in mean depressive symptom severity, t(18) = 1.40, p = .18, or age, t(18) = −.29, p = .78, between depressed–supported and depressed–self-reliant groups, which suggested that these variables had limited confounding effect on the observed differences. However, there was a difference between groups in terms of race/ethnicity. The majority of depressed Black women (83%, n = 5) were self-reliant rather than supported. Among White and Hispanic participants, higher depression scores were associated with more use of social support (ρ = .42, p < .01; Figure 2). In contrast, among Black participants, higher depression scores were associated with less use of social support (i.e., more self-reliance; ρ = −.56, p = .049; Figure 2).
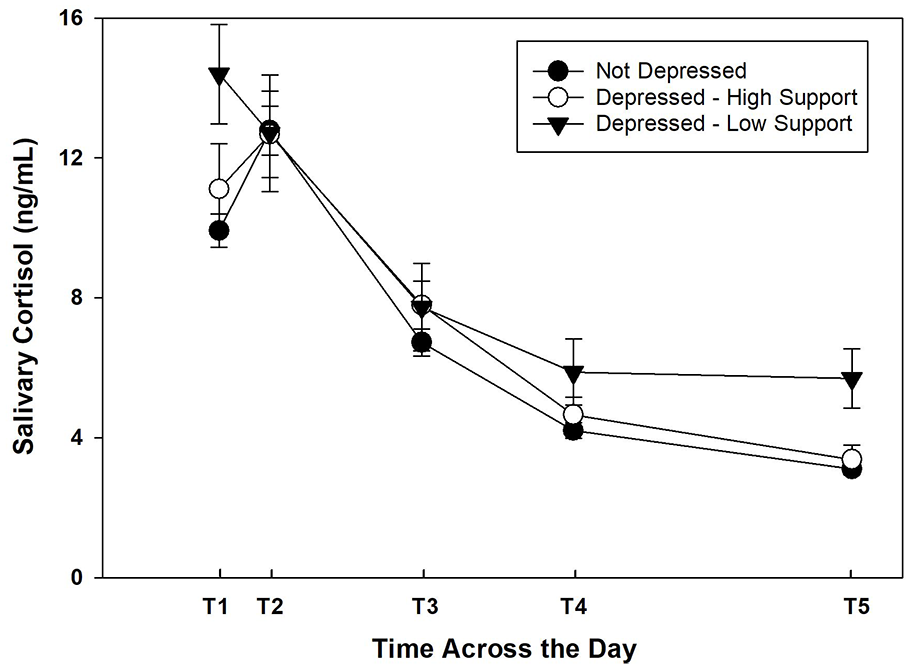
Comparison of diurnal cortisol among not depressed, depressed–high support, and depressed–low support groups.
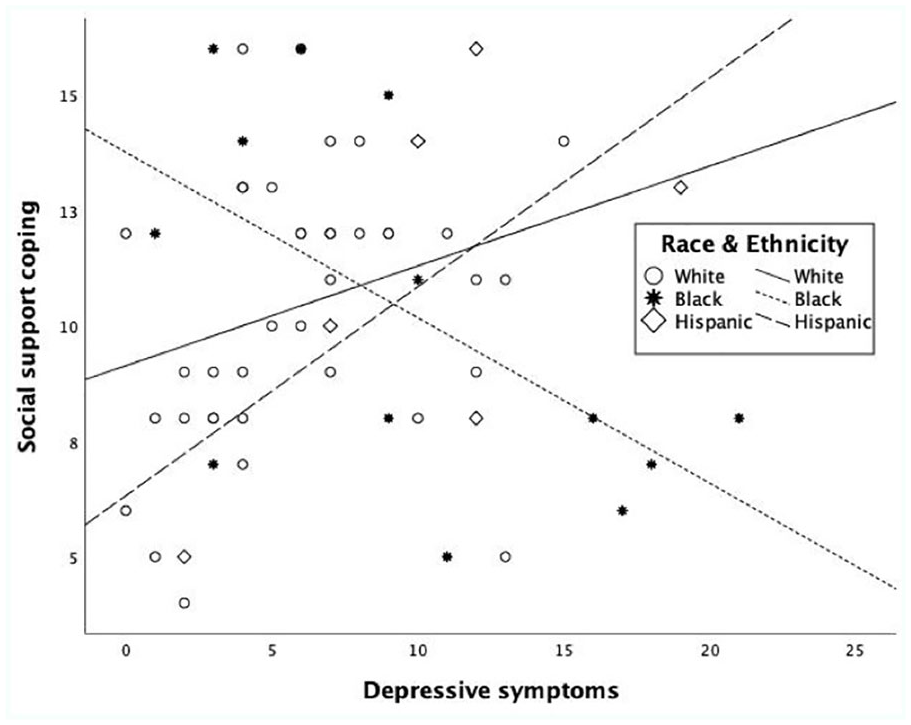
Relationship between depressive symptoms and social support coping by race/ethnicity.
Qualitative Findings
The qualitative analysis focused on describing sociocontextual factors that explain why some women use less social support coping. Compared with the larger sample, the qualitative subset was more likely to be single/unpartnered (30%), and have lower income. Notably, over half (58%) of the qualitative subset reported an annual household income less than $20,000 (United States), which is considered below the federal poverty line for a family of three (Table 1). Figure 3 illustrates the integration of qualitative and quantitative findings.
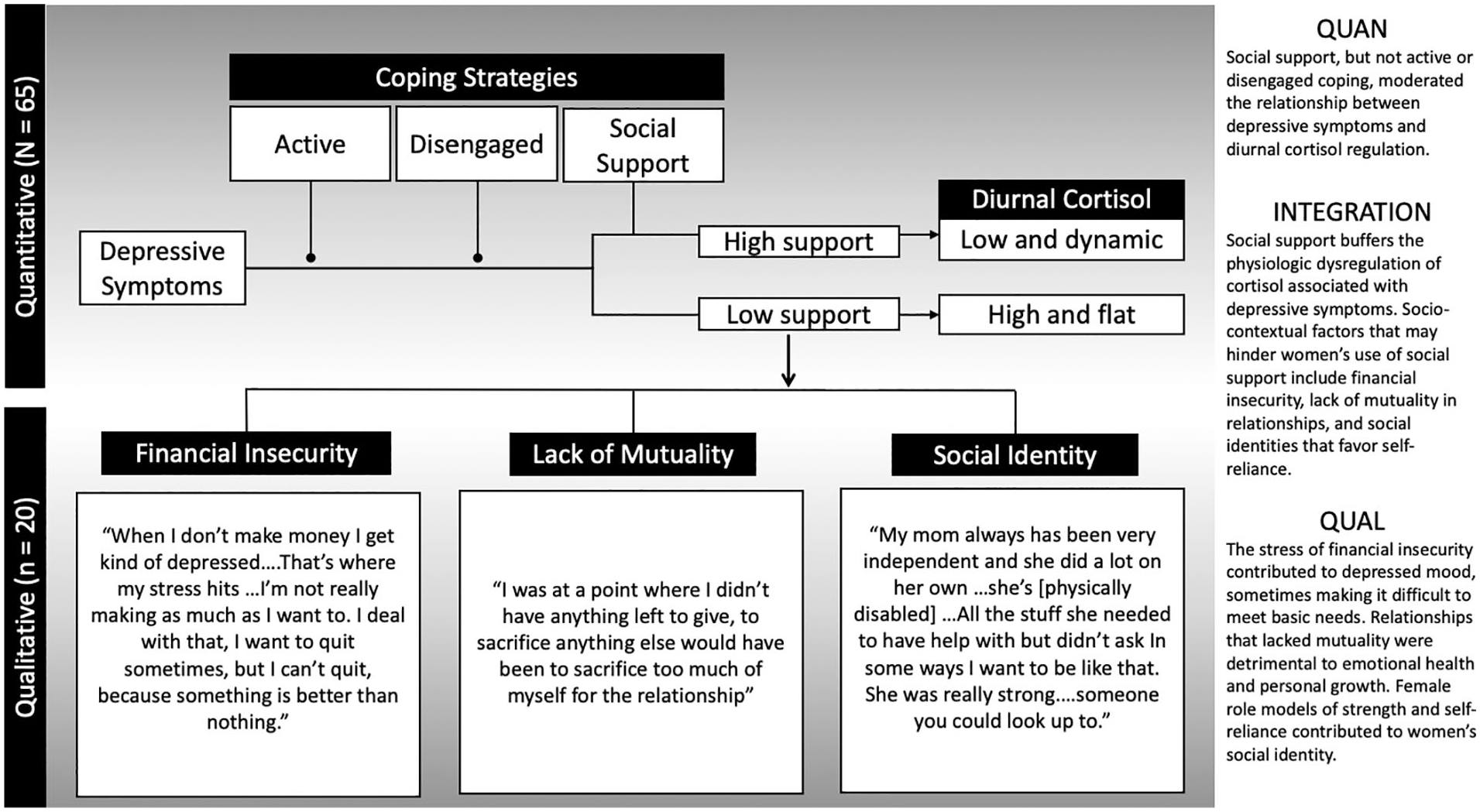
Integration of quantitative and qualitative findings.
Financial Insecurity: “That’s Where My Stress Hits.”
The stress of financial insecurity made it a struggle for women to meet their basic needs, such as housing and food. One participant described her depressed mood as normal response to financial insecurity: “Everybody has their financial depression going on at some time.” Another participant explained: When I don’t make money I get kind of depressed. . . . That’s where my stress hits. . . . I’m not really making as much as I want to. I deal with that, I want to quit [my job] sometimes, but I can’t quit, because something is better than nothing.
When basic needs were unmet, social support in the form of time, money or resources (e.g., food, housing, transportation, and child care support) were the most immediate concern related to social support. However, given that financial instability often affected women’s larger social network, it was unfeasible in many instances to seek support from others in the network. For example, the father of one participant supported her with a place to live; however, food was another concern. She explained, “Since I don’t have really that much food at my dad’s house, I only get one free meal at McDonalds [as an employee]. I eat there throughout the day.” Another participant who left a college scholarship in order to care for an ill family member, in addition to working two jobs, explained: “Just me working two jobs and still feel like I don’t have anything. . . . I’m not having enough to save for myself and for the baby . . . that’s stressful.”
The precarity of day-to-day living and the persistent struggle of meeting basic needs made it risky to let one’s guard down and rely on others. One participant explained her passive stance toward receiving support as a strategy to ensure greater stability for her children: I don’t think I would ever actually be able to step down and rely on someone else. I can’t do it. . . . Relying on somebody else, putting my whole trust into somebody to do that, no way. I have two kids, no way. Too much on the line. If it was just me, fine. . . . I’ll go wherever and do whatever. I don’t need much. But no, I’ve got two people to worry about. I can’t. I wish I could, but I don’t—I won’t.
Lack of Mutuality: “I’ll Do Anything.”
When the needs for support within a network were high and resources were limited, social reciprocity within social relationships were imbalanced in ways that were not favorable for women. Women often perceived themselves to be the strongest link within their social network, leading them to see other’s needs as greater than their own. As such, social relationships were often more emotionally and/or financially draining than they were supportive. One participant who worked long hours in a physically demanding food service job explained how she financially supports herself as well as a significant other affected by drug addiction: I tried to do all the things that I could possibly do to either try to show him or coax him or do anything, to the point where it’s just like “I’ll pay all the bills—just go get help—I’ll pay for you to get help.” I’ll do anything. . . . I will give him a couple hundred dollars here or there for food—I want to make sure there’s food there. I give him money to pay his phone bill.
In light of high stress and demands, participants discussed the need for social boundaries as a way to prevent over-supporting others and/or managing stress-related social conflict. This involved setting limits on the extent to which women would tolerate the needs and demands of others. One participant described how she deliberately disengaged from a social relationship with an older female family member: “It just comes to the point where I get disrespected for no reason and get names called at me. . . . I just cut the strings off with that lady. I’m not going to stress over her.”
Social boundaries were also important when relationships had a counterproductive effect on women’s life goals. One participant explained how she decided to distance herself from a large social network of friends: I have a lot of different friends but I wouldn’t consider them friends now. We didn’t do anything together besides keep each other down. We wouldn’t lift each other up, we wouldn’t encourage each other to go get a job or stop using drugs. We’d be hanging out real late, stealing each other’s mom’s cars . . . drinking and just doing some of the most irresponsible stuff. . . . I don’t want them at the hospital [when I deliver the baby]. I asked them already not to. I’m setting boundaries for myself. . . . I’m happy that I can do that, that I’m able to voice that I don’t want to be friends with them and I don’t want them around me when I’m at a different place in my life. I feel like I need to stand my ground so that they take me seriously. I don’t live like that.
Social Identity: “I Want to Have a Big Heart Like She Had.”
Women spoke of female strength as a part of their social identity, particularly as it related to managing emotion and asking for help. One woman described her own mother: She’s the type—she wouldn’t cry in front of us. I kind of want to be like that too. . . . doesn’t like expressing her emotions and that’s probably where I get that too, not wanting to show my feelings and talk about my feelings. My mom, she doesn’t show her emotions. She will when she is behind closed doors or by herself. That’s when she will cry, but in front of people she wouldn’t do it. When she found out about my dad’s [death], she actually broke down for the first time and I was like “Wow.” That was the first time I ever seen her actually break down before ever in my life. She just holds stuff in.
Another participant described her mom, who had a physical disability, as a model of strength: My mom always has been very independent and she did a lot on her own . . . she’s [physically disabled]. . . . All the stuff she needed to have help with but didn’t ask. In some ways I want to be like that. . . . She was really strong . . . someone you could look up to.
Models of social identity extended across multiple generations, as another participant described her grandmother: My grandma was just a one of a kind. I’ll never find nobody ever in my life like her. Even though she was sick, she was always a helping hand. Even on her deathbed, she was still trying to help everybody. I want to have a big heart like she had.
In contrast to giving support, women had more ambivalence toward seeking support from others, such as mental health care providers. One participant described how she avoided formal support as was a way of protecting herself and her children from “the system”: I don’t want to go to these people. I know that they are there to help, and that’s what their job is, but I’m just the kind of person, I don’t want everybody in my business. I been to therapy and all that—my whole life (sniffling). I don’t want to have to go through it again. I’ve been through all that just being a kid, not having to go through it for my kids. (Sniffling) I don’t want us to be in the system.
Another participant explained her ambivalence around seeking support from mental health care providers: I don’t really feel comfortable signing up for a therapist, or opening up to one. . . . Ever since I was a kid, I’ve had to tell the same stories. But as I am getting older, there’s more to tell. It’s just hard. I do talk, I just talked to you. I cried for a little moment. I got it out. Somebody heard my pain. Somebody knows what I am going through. But for me to just go sign up for a counselor myself, or just go start seeing one out of the blue, it’s just not that easy for me. But then again, I do feel good when I talk to people—certain people. I just can’t talk to everybody.
Discussion
The findings of this study suggest that social support coping buffers the physiological effects of antenatal depressive symptoms, but these strategies are shaped by sociocontextual factors such as financial insecurity, lack of mutuality within relationships, and social identities patterned on individual strength and self-reliance. Depressed women reporting high social support coping had more dynamic diurnal cortisol patterns, characterized by a robust cortisol awakening response and better recovery of end-of-day cortisol levels, a pattern comparable to nondepressed women. Depressed women reporting low social support showed marked mood-related alterations in cortisol regulation, including the total absence of a cortisol awakening response and higher bedtime cortisol. The use of social support relative to depressive symptoms differed by race/ethnicity, with White and Hispanic women reporting more use of social support when depressive symptoms were high, whereas Black women reported less use of social support.
The quantitative findings are in line with theories on social buffering of hypothalamic–pituitary–adrenal axis regulation of cortisol (Gunnar, 2017; Hostinar et al., 2014). Although numerous laboratory studies have demonstrated the effects of social support on the acute stress response (Frisch et al., 2015), emerging evidence also suggests that social support influences day-to-day regulation of cortisol. For instance, Giesbrecht et al. (2013) found that higher social support from a partner decreased what they termed “biobehavioral coherence” between subjective psychological distress and cortisol response. Social support was associated with a 50% reduction in cortisol response to distressing situations as compared with women with less effective social support (Giesbrecht et al., 2013). Similarly, other studies have reported that social relationships during pregnancy moderate prenatal cortisol levels, as well as the association between maternal cortisol levels and infant cortisol (Bublitz et al., 2014; Thomas et al., 2017; Thomas et al., 2018). Thus, the physiological, rather than the psychological, response to stress may be especially sensitive to social support.
Variation in the stress-buffering effects of social relationships are patterned, in part, by early life social experiences (Gunnar, 2017). Early life social relationships serve as the foundation for forming supportive social relationships in adulthood, allowing children to develop mental representations of safety and an internalized sense of security over time, ultimately leading to an internal working model for supportive relationships in adulthood (Hostinar et al., 2014). In the absence of supportive early relationships, individuals rely more on avoidance as a coping strategy, have difficulty regulating emotions, and experience extremes in both overexpression (anger) and underexpression (stoicism) of emotion (Gruhn & Compas, 2020). In a recent study that considered both the social context (i.e., stable vs. harsh living environments) and the quality of maternal caregiving early in life, findings revealed that quality of maternal care acted as a social buffer on cortisol only among children who were raised in low-stress contexts (Yirmiya et al., 2020). This finding raises the possibility that social buffering of cortisol dysregulation has diminished and/or absent effects in women, who as children, grew up in stressful environments.
In this study, depressed Black women reported more use of active coping and less use of social support coping. This may reflect greater adaptive use of self-reliance, defined as the tendency to rely on one’s own capacity for problem solving rather than seeking help from others (Choo & Marszalek, 2019). On the one hand, self-reliance can be considered an adaptive strength; however, some researchers have also highlighted the drawbacks of self-reliance, finding that it can give rise to depression, anxiety, and loneliness (Choo & Marszalek, 2019; Liao et al., 2020). Self-reliance is also a defining characteristic of the Strong Black Woman schema (Beauboeuf-Lafontant, 2005; Liao et al., 2020). While is can be a source of strength and resilience, Beauboeuf-Lafontant (2005) suggest that the Strong Black Woman schema can also be limiting in that “the script of being strong enough to deal with adversity often leads [Black women] to deny the possibility of depression and to have the reality of their depression denied by others” (Beauboeuf-Lafontant, 2005, p. 108).
Another finding of this study was that Black women had a significantly flatter diurnal cortisol rhythm (i.e., less cortisol decline from morning to evening), a difference that was not explained by higher depressive symptoms. This parallels other research indicating that factors such as racism and social exclusion, rather than depression per se, are better predictors of diurnal cortisol regulation in young Black adults (Adam et al., 2015; Goosby et al., 2018). The effects of perceived racial discrimination on flattened diurnal cortisol rhythms persist even after controlling for health behaviors, depression, and socioeconomic variables (Adam et al., 2015). Studies have documented a dose-response relationship between cumulative stress (discrimination, exposure to violence, and other negative life events) and flatter diurnal cortisol rhythms among Black pregnant women (Suglia et al., 2010). Furthermore, the effects of stress resonate between individuals, such that one individual’s physiological response to stress can activate the physiological stress response of other witnesses (Buchanan et al., 2012). Thus, there are multilevel structural and synergistic effects of adversity between individuals and within families and communities that affect the functional quality of social support networks in response to chronic stress.
In the United States, Black women are 3 to 4 times more likely to die of pregnancy-related causes than White women, a trend that has continued to rise in recent years (Centers for Disease Control and Prevention, 2020). Rising rates of maternal mortality align, in striking parallel, with increasing income inequality in the United States (Vilda et al., 2019) and are compounded by the effects of structural racism (Taylor, 2020). Although most pregnancy-related deaths are cardiovascular-related (Centers for Disease Control and Prevention, 2020), recent studies suggest that mental health symptoms are the first to manifest within a cascade of socioeconomically linked health outcomes over the life course (Kivimaki et al., 2020). Within the qualitative findings of this study, pregnant women reported that the stress of financial insecurity was a central contributor to their depressed mood. In turn, depression exacerbates the negative effects of physical health problems during pregnancy (e.g., hypertensive disorders; Horsley et al., 2019), suggesting that there is a close interdependence between mental and physical health during pregnancy.
Clinical Implications
Clinical guidelines recommend that evidence-based therapeutic interventions be offered to women at risk for perinatal depression (U.S. Preventive Services Task Force, 2019). Risk factors include history of depression, current depressive symptoms, or socioeconomic risk factors such as young age, low income, or single parenthood (U.S. Preventive Services Task Force, 2019). Inequitable access to health care is a major barrier to depression treatment for marginalized women (Perez et al., 2021). Black women are less likely to be screened for depression or to be offered any form of treatment (Perez et al., 2021). Inequitable access is further complicated when women do not experience the health care system to be helpful or safe. Nursing care informed by principles of cultural safety and trauma-informed care can help redress inequitable access to health care among marginalized groups (Horrill et al., 2020). For nurses, this includes practicing reflexivity (intrapersonal domain), prioritizing relationships (interpersonal domain), and considering the context (structural domain) (Horrill et al., 2020). Nurses can also utilize therapeutic approaches that emphasize social connection, healthy boundaries, and well-balanced relationships, rather than reinforcing individualistic approaches that emphasize personal responsibility and/or blame while ignoring relational or sociocontextual contributors to mental health. For example, interpersonal therapy is a brief, structured approach that frames psychological problems through the lens of interpersonal and social contexts (Barry & Wheeler, 2014). Likewise, relational–cultural theory views relationships and interdependence as a key part of emotional development, especially for women, focusing on relational authenticity, mutuality, connection and empowerment (Jordan, 2017; Lenz, 2016). Furthermore, the interdependent relationship between mental and physical health necessitate the need for an integrated approach to perinatal health care. Psychiatric nurses can support women’s access to physical health care during their childbearing years by practicing holistically, providing health teaching about the relationships between mental and physical health, and referral to primary care providers who practice within a collaborative care model (Tarraza, 2017).
Limitations
Due to the small sample size, the findings of this study are tentative. The analysis did not correct for multiple comparisons due to a small sample size, which can increase the risk for Type I errors. Although there was power to detect moderating effects of coping in the main analyses, it was not powered to control for confounding effects in the secondary analyses. However, the significant unadjusted mean differences in cortisol in relation to social support is an important area for further study. Finally, due to the observational nature of this study, causality cannot be determined.
Conclusions
Social support coping during pregnancy appears to attenuate the physiological effects of depressed mood during pregnancy. Higher use of social support coping was associated with better cortisol regulation in depressed pregnant women. While this study lends strength to theories that social support renders a protective physiological effect during pregnancy, it remains important to frame such effects within contextual factors and systems of power that may condition the extent to which women are sensitive to and/or have access to social support. The findings of this study underscore the value of relationship-centered nursing care for pregnant women.
Footnotes
Acknowledgements
The authors would like to thank the women who participated in this study and Taryn Derickson for her research assistance.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CME was supported by the National Institutes of Health award numbers F31NR016176 and T32NR016920 and a University of Nebraska Presidential Fellowship, University of Nebraska Medical Center, Omaha, NE. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding sources.