
Abstract
Health Pathfinder is a multilevel system change intervention initiated to transform the health response to domestic violence and abuse in eight sites in England. The current study drew upon interviews with health professionals (n = 27) and victim-survivors (n = 20) to provide a realist account of how this intervention achieved its goals. Findings show that five change mechanisms explain why Health Pathfinder was effective as an ecological intervention: awareness, expertise, relationships, empowerment, and evidence. Positive progress in respect of each mechanism had meaningful impacts on victim-survivor experiences of enquiry, disclosure, and uptake of services and had the potential to meaningfully impact health inequities.
Introduction
Every year an estimated 5% of people aged 16 and over in England and Wales experience some form of domestic violence and abuse (DVA) 1 and approximately 20% have experienced it since the age of 16 (Office for National Statistics, 2022). The high prevalence of DVA means that a large proportion of people attending accident and emergency departments, primary care, family planning, and reproductive and sexual health settings are likely to have experienced DVA at some point (Alhabib et al., 2010; Feder et al., 2009). The detrimental physical and psychological health effects associated with experiencing DVA are myriad and well evidenced (Afifi et al., 2009; Boyle & Jones, 2006; Devries et al., 2013; Oram et al., 2017). When seeking help, four out of five victim-survivors do not call the police, but almost all victim-survivors use health services at some point, especially those with complex needs (Dheensa et al., 2020). Despite its scale and scope to intervene across the lifespan in both mental and physical health problems, to date the health system response to DVA can be described as at best variable.
Bespoke programs often focus on single-factor initiatives, such as training health professionals to screen for DVA, which tend to be limited to certain settings, dependent on short-term funding and subject to mixed results (Garcia-Moreno et al., 2015), resulting in uncertainty about the effectiveness of health-based initiatives (Feder et al., 2011). Additionally, multiple barriers to professional DVA screening are well-documented, including limited resource and capacity (Beynon et al., 2012); perceived incompetence relating to identifying, asking and responding to DVA (Taylor et al., 2013); and resistance to healthcare roles and responsibilities in DVA intervention (Sprague et al., 2012). These problems feature both in the UK's National Healthcare Service (NHS) and in most countries (Garcia-Moreno et al., 2015).
These short-comings have highlighted the need for multicomponent system-level interventions, attending to organizational change and partnership working, in addition to training and support, to improve health-based responses (O’Campo et al., 2011). Considerable effort has therefore been invested in recent years to improve the system-level response to DVA across the full range of health care settings. In the UK, this was accelerated by the National Institute for Health and Care Excellence (NICE) issuing public health guidance advising healthcare professionals to cooperate with partner agencies to identify, prevent, and reduce DVA (NICE, 2014). More proactive participation from healthcare providers strengthens multiagency partnerships to address DVA, helping to overcome the barriers highlighted above. It also provides victim-survivors alternative remedies that can be sought, separate or in addition to recourse from the justice system, helping to identify “hidden” victim-survivors of DVA.
There are two main system-level health-based initiatives in the UK (Macdonald, 2021). The first is the Identification and Referral to Improve Safety (IRIS) model for general practitioners; a collaboration between primary care physicians and DVA organizations that deliver victim advocacy, which includes training and education for doctors by specially trained and co-located Advocate Educators, the implementation of clinical enquiry to identify DVA, and establishing a referral pathway to a specialist DVA support and advocacy service. Randomized trials have highlighted its effectiveness in professional identification, referral, and response to DVA, highlighting the benefits of partnership working to increase professional responsibility, capacity, and confidence in responding to DVA. Additionally, IRIS was particularly beneficial for addressing DVA in “hidden” victim-survivors, that would not necessarily come to the attention of criminal justice agencies, enabling victims to access community-based advocacy as their first or only point of contact (Othman et al., 2014), which is known to be effective in preventing re-abuse (Feder et al., 2011). The second initiative is the co-location of Independent Domestic Violence Advisors (IDVA) in hospital settings. This also results in the identification of “hidden victims” not known to other agencies, who have higher levels of complex problems such as severe anxiety and depression and who can benefit from specialist support (Halliwell et al., 2019). While effective and cost-efficient, these programs are not consistently implemented across all areas of the UK.
Intervention Principles and Evaluation Rationale
The Health Pathfinder intervention was independently designed to transform UK healthcare's response to DVA by ensuring a coordinated and consistent approach across the health system including acute, mental health, and primary care services, known as a “whole health” response. The crux of the Health Pathfinder intervention is to improve the awareness, knowledge, and skills of health professionals and their systems to increase professionals’ ability to enquire about DVA routinely and sensitively, and to increase the healthcare system's ability to support professionals in doing this work effectively and consistently. Intended outcomes included increased confidence of victim-survivors to disclose and increased likelihood that victim-survivors would receive a professional response to their needs, including a timely referral to specialist services—resulting in more people helped to safety and sooner. These intended outcomes would be made possible through individual and system-level initiatives including training professionals, reviewing clinical policies relating to DVA, integration of DVA services and related governance structures, co-location of DVA services, coordinated partnership working, enhancing data collection strategies, and commitment to whole health response.
As Health Pathfinder involved a range of healthcare roles and functions operating at multiple levels to achieve diverse individual and system-level outcomes, the intervention was understood to be a complex, ecological intervention from the outset. Hence, we followed the MRC guidance for developing and evaluating complex interventions (Skivington et al., 2021), to not only establish intervention effectiveness using outcome evaluation but also theorize how Health Pathfinder achieved its intended outcomes using realist evaluation. While the outcome evaluation focused on statistical inference, showing Health Pathfinder achieved its key intended outcomes, i.e., generating meaningful system-level changes in the identification and referral of cases, with victim-survivors of DVA receiving support at an earlier stage in the process (Melendez-Torres et al. 2021, p. 9), in this paper, we focus on the realist evaluation. Realist evaluation (Pawson & Tilley, 1997) is explanatory—focusing on generative causation, seeking to understand “what works, for whom, under what circumstances and how” (Pawson et al., 2005). It does this by developing tentative accounts of how interventions generate their outcomes by setting off mechanisms in specific contexts, otherwise known as “context-mechanism-outcome configurations” (Pawson & Tilley, 1997). This collection of propositions describing how interventions generate their effects is known as the program theory. Nascent research has underscored the importance of contributing to the program theory needed to understand how DVA interventions achieve their impacts (Velonis et al., 2020). Thus, the aim of the realist evaluation was to contribute to the program theory of the Health Pathfinder intervention through interviews with health professionals and victim-survivors.
Methods
Research Design
Health Pathfinder was a complex ecological intervention and therefore we used a realist evaluation method (Pawson & Tilley, 1997) to understand how the intervention achieved its intended goals, for whom the intervention achieved its intended goals, and in what contexts these goals were achieved.
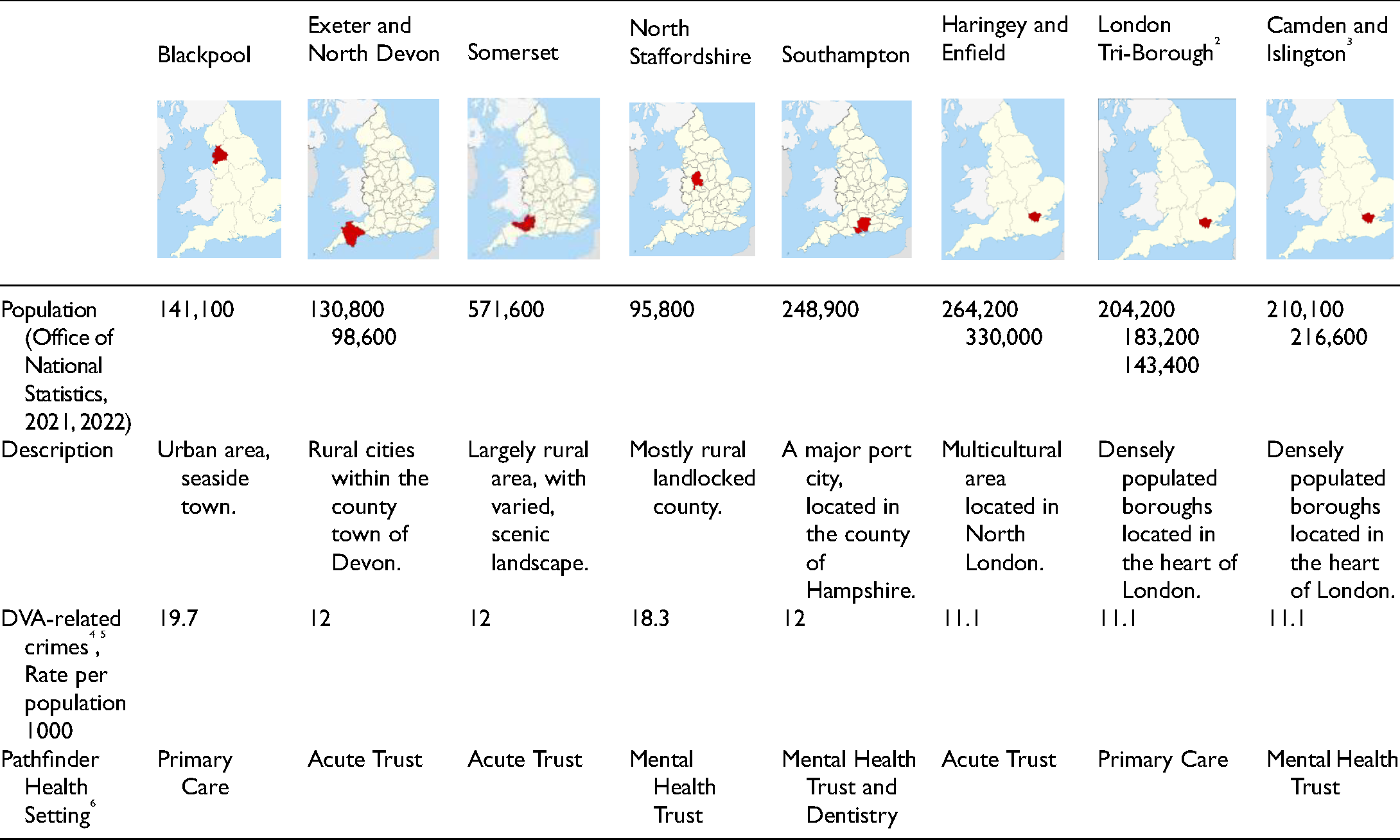
Health Pathfinder was implemented across eight sites in England comprising acute trusts, mental health trusts, and primary care between 2017 and 2019, and our evaluation began in Spring 2019. In line with best practice (Skivington et al., 2021), we began our study by developing an initial program theory and associated logic model from which to evaluate from—based on intervention materials and in collaboration with key stakeholders (see Figure 1). Thus, despite differences in the nature and scope of the projects, the program theory shows all eight sites (see Table 1) shared a set of underpinning principles, intervention components, mechanisms for change, and intended outcomes.
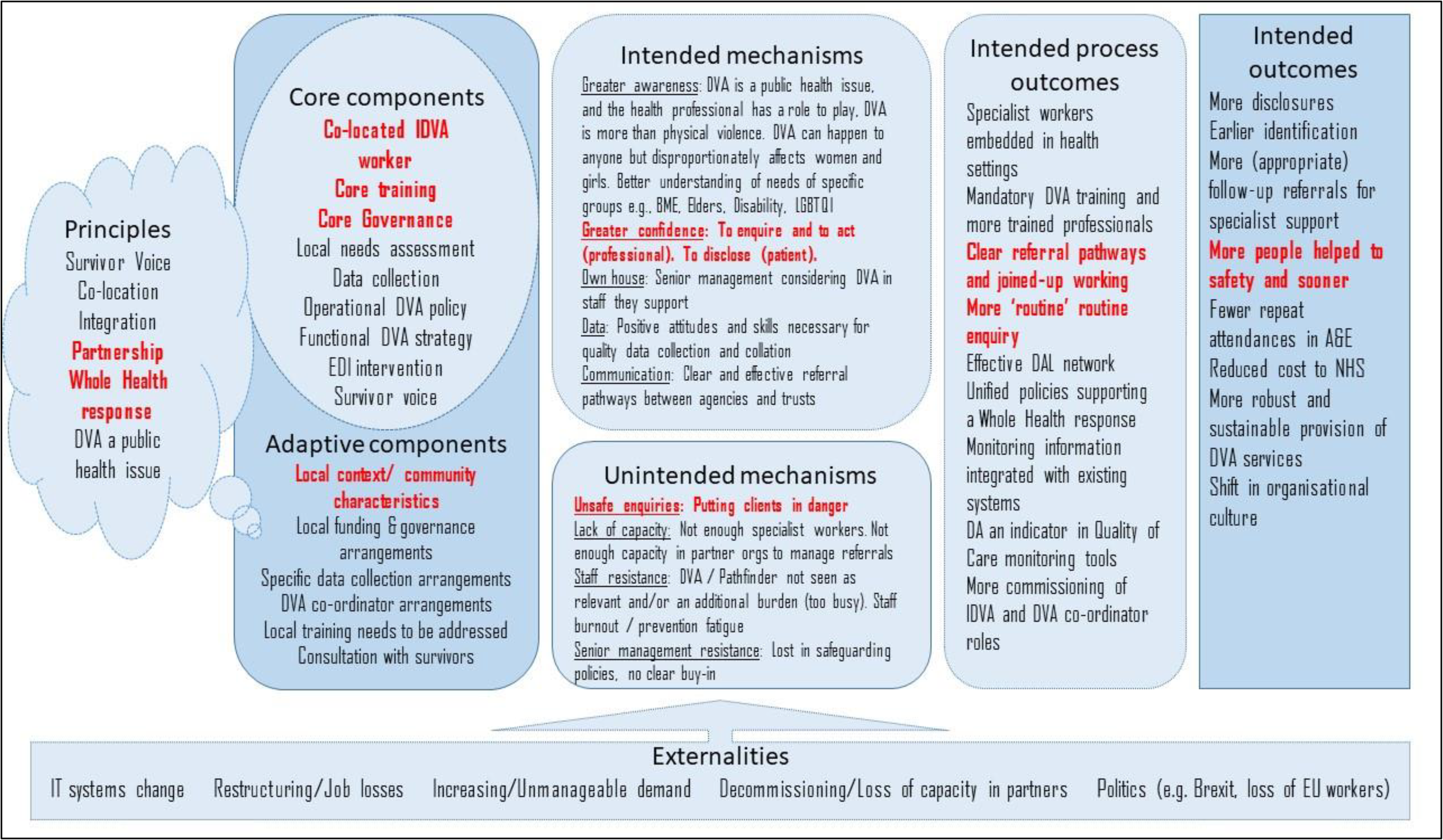
Graphical depiction of the Health Pathfinder logic model.
Pen Portraits of the 8 Sites.
The goal of the realist evaluation was to clarify and refine the program theory needed to understand how Health Pathfinder achieved its effectiveness, through interviews with health professionals and victim-survivors. Our overarching research questions were: How did Health Pathfinder achieve its goals? How were system-level and victim-survivor-level impacts achieved? Who does Pathfinder work for and in what contexts?
Participant Recruitment
We conducted semi-structured interviews with health professionals and victim-survivors. Ethical approval was provided by NHS Wales Research Ethical Committee 3 on 21st August 2019 (REC Ref: 19/WA/0206). The interviews were conducted after a period of intervention implementation, between September 2019 and March 2020, to account for any potential latent factors in results. Both victim-survivor and health professional participants were provided with information about the study in advance of data collection, detailing confidentiality, anonymity, and the process of informed consent. This information was discussed with the participant, ensuring questions or uncertainties were addressed, prior to providing informed consent.
For health professional recruitment, we worked with coordinating staff from the organizations leading Health Pathfinder to identify those involved in different aspects of the intervention, staff who had received training, strategy group members, or DVA specialists (i.e., IDVAs, Advocate Educators, and DVA services). After an initial contact email, we sent consent forms to health professionals who expressed an interest and arranged a mutually convenient interview date and time. Completed informed consent forms were obtained via email before telephone interviews took place. Consent was verbally checked and audio-recorded before interviews commenced.
We interviewed victim-survivors with recent experience of service use in Health Pathfinder areas, as the goal of our study was to focus on their experiences of Health Pathfinder's implementation. Consistent with the contractual terms of our evaluation, we focused on recruiting women victim-survivors and this paper uses data collected from the 20 women victim-survivors who consented to take part in the evaluation. The process for recruiting victim-survivors was agreed in consultation with DVA specialists in intervention sites and included consideration of risk and safety at point of contact. DVA specialists approached victim-survivors using the information sheet and completed a consent to contact form, alongside safety information relevant to contacting the victim-survivor. Victim-survivors were contacted by the research team and invited to take part in an interview. Interviews were undertaken either face-to-face or over the telephone and undertaken by female members of the research team. Victim-survivors were offered a £20 shopping voucher to thank them for their contribution and advised they would receive a follow-up safety telephone call from their DVA specialist. Written informed consent was obtained for all face-to-face interviews. For telephone interviews, each consent statement was read out to the victim-survivor to check their understanding and agreement, which was audio-recorded and then quality checked by another member of the research team for final sign-off.
Data Collection
Each Pathfinder site had an interview recruitment target of 2–3 professionals and 2–3 victim-survivors. This was seen as an acceptable, yet feasible target with a focus on in-depth accounts to provide theoretical insight (Emmel, 2013). The overall interview sample is representative of professionals working in acute trusts, mental health trusts and primary care, and victim-survivors with ages ranging from 19 to 63 and entering the service with low to high-risk needs and a range of different DVA experiences (e.g., physical, psychological, sexual, etc.). In total, 47 participants took part in interviews (n = 20 victim-survivors and n = 27 professionals). Interviews ranged in length from 16 min to 83 min (average = 30 min). All interviews were audio-recorded and transcribed verbatim by a professional transcription service. Interview guides and questions were based on and informed by the intervention logic model (see Melendez-Torres et al. 2021).
Data Analysis
Our analytic orientation was realist in nature (Pawson & Tilley, 1997), focused on developing accounts to explain how the intervention generated outcomes, for whom, and in what contexts. Consequently, our analysis consolidated around a set of context-mechanism-outcome configurations (Pawson & Tilley, 1997) that related salient contextual factors, key mechanisms that drove intervention impacts, and the outcomes these mechanisms produced in different contexts within an explanatory framework. To develop this explanatory framework, we used qualitative analysis informed by Straussian grounded theory methods (Corbin & Strauss, 2015) of constant comparison, open coding, dimensionalization, and designation to work from fine-grained observations within sites to regularities between sites, to develop an explanatory framework that balanced analytic power across diverse sites with site-specific observations. Recent innovations in realist methods have also focused on “emergence,” understood as how contexts and mechanisms can create the conditions for a further set of mechanisms to fire (Jagosh, 2019). We incorporated this innovation in our analysis by considering how mechanisms were linked sequentially and iteratively in the contexts in which they unfolded. The analysis was consensus-based, working across the research team to develop shared understandings, and drawing on a shared data library (NVivo, QSR International), thus resulting in explanatory accounts to demonstrate how Health Pathfinder initiated causal mechanisms within specific contexts, to achieve its outcomes.
Results
In the next section, we discuss the contextual factors relevant to understanding effectiveness and the mechanisms that were “set off” by Health Pathfinder to achieve specific outcomes. Our analysis revealed five mechanisms that together can account for an improved response to DVA in the Health Pathfinder sites. These are described in the subsequent sections as step-changes in the nature and scope of (1) awareness, (2) expertise, (3) relationships, (4) empowerment, and (5) evidence across the sites.
Contextual Factors
Even though one of the ways in which the effectiveness of Health Pathfinder was most directly “felt” was via more effective and more timely contacts between victim-survivors and DVA services (see self-citation), achieving this meant a range of people working together and across multiple domains of health. The power of compassionate enquiry and effective follow-through were key concepts that were most clearly evidenced in our interviews with victim-survivors. While this was most manifestly facilitated by co-location of DVA services, successful co-location required successful coordination, which in turn was closely linked to senior management support: “[Co-location] I think really helped the practitioners to know who you are, know what service you’ve come from and help to develop that partnership working. It really did help, but then a lot of that encouragement did come from management I found” (P29).
This DVA coordination work occurred in many cases behind the scenes of patient contacts, but this makes it no less important. DVA coordinators primed health professionals to engage with, and be empowered in, the work of appropriate enquiry and referral; worked to embed the principles of Health Pathfinder in trust policies; and organized training for health professionals. In addition, a range of components that extended beyond co-location and coordination and that may be less immediately linked to outcomes—such as technical assistance and training around trust and practice policies, data collection and evidence generation, and responding to the needs of groups of victim-survivors that have traditionally been marginalized—played a central role in the generation of positive outcomes.
The delivery of any complex intervention is informed by multiple contextual factors. Our research identified the salience of the individual victim-survivor's life (e.g., life history/experiences; experiences with DVA; experiences with health professionals; readiness for change; mental and physical health issues; etc.) alongside features of the particular intervention site (e.g., organizational and community contexts) as key for understanding how this intervention was delivered. One significant contextual factor underpinning victim-survivors’ engagement with Health Pathfinder was their fear. Patriarchal beliefs, negative preconceptions, and the perceived unwelcoming, judgmental, and disbelieving attitudes of some health professionals were mentioned by victim-survivors as greatly contributing to their levels of fear, which subsequently impacted upon their willingness to disclose: “When it was all sort of happening it was like, they’re not going to believe me” (S9).
This was exacerbated for many by shame, self-blame, and other negative consequences of DVA on their mental health. For these victim-survivors, presentation to health services was usually for mental health symptoms without DVA being disclosed as the underlying cause. Consequently, health professionals would focus only on treating mental health, by prescribing or signposting to mental health services, without providing any access to DVA services: “Just cos someone's depressed it might be deeper than that. It's not always, ‘Oh you’ve got depression. Shove tablets down your throat. You’ll be fine’” (S8).
In contrast, victim-survivors further along the journey of change, who recognized that they were experiencing DVA, were more likely to attend health settings with the intention to disclose: I just decided I’d go to doctors and just say, “I need help because my ex-partner's mentally abusing me” (S8).
This distinction emphasizes the importance of health professionals being able to accurately identify each victim-survivor's own “window of opportunity” for action, and then knowing how to support, signpost, and refer accordingly. Victim-survivors’ individual needs were more likely to be met when they felt comfortable with a professional who had communicated empathy and care, and whom they felt they could trust.
Funding, culture, and environmental characteristics were important contextual elements in each of the sites. The Health Pathfinder intervention was clearly tailored to each site's most urgent and significant gaps in provision to determine the best use of funds, which had to be allocated in diverse ways, especially since some areas had more “ripe” funding environments than others. All eight sites implemented some combination of a full and/or part time co-located IDVA, an Advocate Educator as part of IRIS, a DVA coordinator post, and/or training and policy improvement work alongside efforts to improve the quality and scale of data collection around DVA. Sites were at different “starting points” in relation to their existing policies and practices and therefore had different desires in relation to Pathfinder's input. For example, some sites were treading relatively new ground implementing DVA interventions in areas of health such as mental health and dentistry: “I must say it has also raised the profile of dentistry across the system” (P21).
Furthermore, each of the sites had their own distinctive environment and occupational culture that the intervention needed to fit into. For example, primary care and mental health seemed to lend themselves well to not only partnership working but also co-working on individual cases. In contrast, Accident and Emergency (A&E) was described as a chaotic environment where clinicians faced significant time and workload pressures and where most IDVAs reported struggling to find private space to talk with patients: “They were a little bit more tricky and resistant, partly because of the volume of their work and it's very hard to get privacy in an Emergency Department” (P15).
Management commitment to tackling DVA was an important factor in understanding the local culture. This ranged from an explicit attitude of “it's not our responsibility” (P25) to a blank slate with nothing “there to really start off with” (P10) and “fantastic individuals” (P17) who had already won over hearts and minds in relation to DVA. This often related to a site's pre-existing local partnerships: some described themselves as already having a strong base in relation to policy, practice, and local partnership working, whereas others had little existing or dysfunctional relational infrastructure. Around half of the sites were able to point to previous projects that helped create a local DVA partnership culture, which were regarded as beneficial to the effectiveness of Health Pathfinder: “Pre-Pathfinder I’ve been involved with another department domestic and sexual abuse project and that was to embed a cultural change in domestic and sexual abuse. So … that was the groundwork that was kind of already there when … we were approached to sign up to the Pathfinder project” (P13).
In sum, sites were at different levels of readiness for change, meaning that in some areas Health Pathfinder landed on fertile ground, whereas in others it did not. Rurality and physical remoteness, along with community demographics (e.g., an aging population), were other contextual factors that were identified as important for understanding how Health Pathfinder operated locally.
Mechanism 1: Awareness Generation
The first mechanism by which Health Pathfinder achieved effectiveness was by generating awareness of DVA, for both victim-survivors and professionals, and was the necessary foundation from which the subsequent intervention mechanisms could be built. Victim-survivors needed to be aware health services could act as an entry point. They highlighted the importance of visible services in health-based settings, reflecting on the “traditional” boundaries between health and DVA services. Integrating across these boundaries was one way in which Health Pathfinder increased access to services: “I wanted some kind of support, or someone that could talk to [me] about my … abusive relationship, the counselling through NHS Wellbeing, I thought well that will help me with depression and anxiety, but … the counsellor isn't a domestic abuse expert” (S6).
Victim-survivors suggested leaflets and posters as powerful ways to increase the visibility of and thus awareness of health's role and responsibility in addressing DVA, which could potentially inspire a willingness to disclose: “They might be there for something else that day but then they might see the poster and then think well it says on there that they're here to help” (S10).
Victim-survivors highlighted the “windows of opportunity” arising in health settings, without the perpetrator and within a safe and confidential space, which were a central and foundational aspect of how Health Pathfinder achieved effectiveness: “You can go to that appointment on your own, they [perpetrator] don't have to be with you… It's all confidential so you've not got to worry. It's a private room isn't it, no one can hear you” (S10).
However, it also highlights the importance of professional awareness around their role and responsibility to utilize and maximize these opportunities to address DVA. Awareness was generated through various components of Health Pathfinder, which created an environment where open conversations about DVA became more common and part of the culture: “We hope that would encourage people to come over and talk to us and um, make talking about DVA more open” (P29).
Most professionals stressed the importance of co-locating DVA specialists across sites as a physical and visible part of the health team to generate (and maintain) awareness of DVA in the local culture: “Having me there kept the conversations of domestic abuse alive, because just by seeing me, people were triggered to think about domestic abuse and think about the cases they had. So that led to like more enquiries even when I’m not physically present there…. But, I do think that the responsibility still does lie with literally having to physically be present” (P29).
Co-location created visibility of DVA within health that enabled victim-survivors to get in-time, same-visit access to the service internally, without the delay of waiting for a referral, helping to create those “windows of opportunity”: The biggest benefit working in the hospital is often that's the only time the victim may be left alone by the perpetrator. They can talk to the IDVA because the IDVA is onsite most of the time … the main difference is having qualified workers accessible to that support where needed. Because I do believe that a window of opportunity opened. (P14)
Attempts to integrate DVA specialists into health settings were not without challenges. Several services reported difficulties being “noticed” within health settings due to lack of space. Despite using several strategies to increase visibility (e.g., attendance at team meetings), they still experienced other practical challenges (e.g., inadequate office space, getting honorary contracts, access to health records, an NHS email, etc.), which were essential for everyday work tasks and for generating the trust and buy-in between health professionals and DVA specialists: I was allowed to sit within the team, but not having access to certain things because of the confidentiality. Even after the honorary contract came through, I still [don't have] access to NHS email or any of their care notes. So, I rely on professionals there to share certain information with me. (P30)
Increased awareness through training and co-location raised the profile of DVA, creating possibilities for more open conversations through the visibility and presence of a dedicated service and shaping the conditions for successful co-location. Generating awareness was thus the foundation for a broader cultural shift in perspective within health that encouraged health professionals to understand and consider DVA as a core aspect of their role.
Mechanism 2: Expertise Generation
Though awareness generation was foundational to the effectiveness of Health Pathfinder, expertise generation was the mechanism that was most apparent to interviewees. Victim-survivors highlighted the value of knowledgeable and skillful professionals for recognizing DVA, facilitating safe enquiry, and signposting and referring to specialist services. This included interpersonal skills to make victim-survivors feel comfortable enough to disclose, particularly those who were earlier in their help-seeking journey or who had mistrust in professionals: “Because I felt comfortable sitting with him and speaking to him … You can sort of open up to that person and say what's going on” (S10).
Confident, sensitive, and safe enquiry by health professionals required a level of expertise that Health Pathfinder generated through formal training, informal training (coaching), and co-location. The delivery of the formal training component of Health Pathfinder unfolded differently across sites, fitting into the organizational contexts. This included decisions relating to its value, particularly if existing training models were felt to be effective. In addition, other decisions included proceeding with train the trainer models, viewed to be more sustainable across a large trust vs delivery by experts, which were viewed as more credible: “The advantage of having experts in the room is that you know they really know what they're talking about, that is their bread and butter, it might come up for us every so often but it's not something that we specialise in” (P2).
Delivery of training also depended on the local NHS training policies for health professionals. Interviewees expressed the importance of mandatory DVA training for health professionals as a means of generating expertise but also recognized that DVA training competes with many other issues for mandatory status. Thus, interviewees emphasized Health Pathfinder training needed to be compressed due to time pressures and workloads of health professionals which limited their capacity to attend training: “I know the one thing is the training aspect, people being able to take time away from certain roles, because on a ward it's very difficult to be able to always commit to your training that you’re having” (P25).
Nonetheless, the upskilling of health professionals was deemed one of the main successes of Health Pathfinder, going beyond the factual aspects of DVA to include a range of topics relating to intersectionality, i.e., women of Black and minority ethnic background, women with disabilities, and women who identify as LGBTQ+: “But certainly, my understanding of the biggest impact that I've seen that Pathfinder has was really in the training” (P16).
In addition to formal training, interviewees described how DVA services made a significant contribution to expertise generation, via informal training (i.e., coaching) occurring as a result of their co-location alongside health professionals. These specialists coached health professionals through cases, providing regular opportunities to “learn by doing.” This was regarded as more beneficial than formal training because it was tailored to scenarios: “I’ve learnt more from what she's done. Where there's been people who haven't given consent to see [IDVA], she has had to train that individual up … it's coaching if you like really” (P11).
Successful informal coaching also created a level of trust between DVA services and health professionals, giving professionals the opportunity to become more independent in addressing DVA, as well as encouraging joint working: “I found that as soon as I worked with somebody on a case together, then that continued to develop, and we continued to work together more frequently” (P29).
Joint working generated by co-location also resulted in bidirectional, symbiotic expertise generation, resulting in improvements in DVA services own practice: “Mental health professionals are then able to also help the domestic abuse service, you know, and, and provide them with a bit of training as well” (P25).
Therefore, expertise was generated through the multidirectional transfer of knowledge between subject-matter experts and health professionals (as well as between other health professionals). This expertise was made “necessary” by the awareness of DVA that Health Pathfinder created.
Mechanism 3: Relationship Generation
Generating and maintaining effective working relationships were central to the effectiveness of Health Pathfinder and appeared to be crucial pre-conditions to implementation. Relationships were multifaceted and manifested in a range of ways, including coordination-led spearheading; strategic networks; as passionate leadership and communication; and as buy-in across all levels, from senior management to frontline staff. Several sites benefited from strong pre-existing relationships and years of partnership working. In these sites, any initial misunderstandings or sources of conflict around governance and operations were resolved long before Pathfinder was implemented: “The one thing I haven't said, which I think has been really key, is that we've got incredibly good relationship with [DVA service] and historically we've worked really, really well together. Um, and that's so important isn't it?” (P12)
Most professionals acknowledged that having a key, invested, person within health to drive and “champion” the intervention forward was vital: “It did require someone to sort of be passionate about it and tenacious and to get other people on board” (P15).
The quality of relationships generated depended on leadership within the NHS. Shared responsibility for DVA was sometimes absent or met with resistance at different levels of seniority. Where investment from senior management was absent, DVA was less likely to be viewed as a core priority in addressing health inequities experienced by women: “There is some ignorance … at the top of the NHS, so one person that I spoke to sent me an email with a link to Refuge, which says they’re open twenty-four hours a day and they will provide accommodation, and so therefore, we don't need an IDVA” (P11).
Additionally, DVA services highlighted examples where resistance from frontline staff impacted on the quality of relationships generated. Interviews suggested that the onus was on the DVA service to build the relationships with health rather than the other way around: “It wasn't easy. There was initially a reluctance and a resistance because of the possible change … it did take a lot of effort to build the relationship and once you built it with one person it started to flow from there” (P17).
Trust was an underlying factor which shaped the generation of working relationships between partners and was something most professionals felt needed to be built over time. In many sites, information sharing was raised as a particular issue relating to trust, particularly if the co-located DVA specialist was external to the NHS. Physical and visible presence of a co-located IDVA helped to build trust to generate good partnership relationships: “If they have an NHS email, it shows staff that they’re part of the Trust and that they can be trusted. Because they worry about sharing information otherwise” (P11).
Higher level strategic relationships were considered a potential lever for intervention sustainability. Strategic networks meant people were no longer “lone wolves” in the NHS and were able to use support from other agencies to strengthen funding requests and create sustainable changes beyond Health Pathfinder: “It allowed us to say this is a consortium of people who were trying to do something … so it gave us something to hang our demand on” (P17).
Therefore, building high-quality relationships between intervention partners was shaped by the nature of relationships that pre-dated Pathfinder and the buy-in or resistance to accepting DVA as a shared responsibility between all partners. While victim-survivors rarely explicitly discussed the value of professional relationships, their accounts of successful and unsuccessful encounters with health services pointed to the ways in which positive working relationships were important (e.g., they led to quicker responses and access to support). This was especially highlighted in referrals to a co-located DVA specialist, who could instigate fast and decisive action when a victim-survivor was in crisis: “They were on the ball with it … they got back to me very quickly and they did the assessment really quickly … so there was no waiting round so that was quite good” (S16). Conversely, services with no co-located DVA specialist appeared to raise barriers to engagement and support: “At first, I was just like, well, that was pointless. I’ve just geared myself up to come here … And then just be sent away with a load of numbers” (S9).
However, although co-location can facilitate the development of positive working relationships, it does not completely guarantee this; nor is co-location unquestionably effective without the relationships co-location and coordination should cultivate. Victim-survivors described how “mere” signposting to DVA services could erode their trust in health services, perpetuating health inequities along axes of oppression, especially where victim-survivors have been let down by health services in the past. Delays in receiving support, limited information about the service, and signposting for self-referral could all impact on engagement with the DVA service. This emphasizes the value in developing strong working relationships to promote multidisciplinary working and shared responsibility to improve victim-survivor outcomes, regardless of co-location.
Mechanism 4: Empowerment Generation
Awareness and expertise were not enough to facilitate action; our analysis revealed that generating relationships led to greater empowerment of health professionals, which was a central mechanism for the effectiveness of Health Pathfinder. This complex mechanism was generated by the previous three mechanisms (awareness, access to expertise, and relationships), which all empowered health professionals to enquire safely and confidently about DVA in the knowledge that Pathfinder structures provided security to enable them to effectively deal with a disclosure. Victim-survivors highlighted the importance of professionals feeling empowered to ask questions that would invite disclosure, emphasizing the acceptability of safe enquiry: “Just making sure that if they do go to see their doctor and they're struggling with depression or whatever, just maybe probably ask a few more questions about relationships at home” (S4).
The empowerment of health professionals to ask was most keenly felt by victim-survivors when opportunities to conduct safe enquiry, signpost to specialist services, or submit referrals had been overlooked and resulted in mental health crisis, eroding trust in health services and reinforcing health inequities: “And because of the relationship, I was very, very depressed … tried to end my life once and nearly did it a second time” (S3).
However, health professionals needed to be not only empowered to ask but also empowered to act, in terms of knowing exactly how to respond to disclosures: “One of my big things is it's all very well to ask the question and feel confident to ask the question around domestic abuse but if you have nowhere to send that person, if you have no response for that, if you have no way to support them following that, it, it's not worth asking the question at all” (P19).
Empowered action appeared to be driven by the work of DVA coordinators and steering groups, whereby relationships generated with DVA specialists helped to create clear signposting and referral pathways for health professionals to respond following disclosures. However, different forms of action were felt to have different levels of impact on victim-survivors. Signposting was only helpful when health professionals clearly communicated the service's role and how they can help, ultimately providing reassurance about involvement of an additional service due to the inherent fear that victim-survivors can experience with disclosure, particularly for groups of women where health services have a pronounced history of structural and symbolic violence (e.g., migrant women who may be in legally precarious situations): “I thought oh God, they didn't explain … she just said ‘I’m putting you through to somebody…’ And I was panicking then” (S11).
There is a clear role for training and policy to equip professionals with this knowledge and information about services, yet referrals were felt to be more valuable for victim-survivors than simply signposting as they did not have to call the service themselves and repeat their stories, deemed important by victim-survivors when accessing specialist services: “Because every single time I’ve spoken to somebody I've had to start again … repeating the whole story” (S12).
Victim-survivors illustrated how empowered health professionals can, in turn, empower victim-survivors. Leaving a relationship and achieving safety appeared strongly linked to the victim-survivor's own journey through readiness for change and the value of these contacts—even where a decision to leave the relationship was not taken—speaks to the additional impacts of Health Pathfinder on victim-survivors’ wellbeing: “I know whichever way I go I’ve got that support that I need” (S7).
Co-location of DVA specialists was the most powerful way of engendering professionals’ confidence to act, as they knew an expert was on hand: “It means I think the staff are more confident at bringing something up … you know a hunch about something because somebody's there to talk to as opposed to now I have to make a referral to another service … you don't need to make a referral, they’re already there” (P13).
Additionally, top-down, trust-wide policies in relation to enquiry were considered important contextual factors to support consistent, safe enquiry and ensure that referrals following disclosure were sensitive to individual circumstances. These policies supported the empowerment of health professionals to ask about DVA because the approach to enquiry was clear and validated from senior management: “So, we have targeted questions for some professionals, but others … like … in-patient admissions, people should be asking this of patients … and giving them a chance to disclose” (P11).
Together, policy foundations, training and coaching, clear referral processes, and the reassurance of the visible presence of a co-located IDVA leading to strong relationships can cultivate health professionals who are not only aware and have expertise, but are empowered to both ask and act. Empowered health professionals unlock the possibility of, and create the conditions for, empowered victim-survivors who feel safe and confident to disclose.
Mechanism 5: Evidence Generation
The final mechanism, evidence generation, came after awareness, expertise, relationships, and empowerment and was often the last mechanism to be unlocked by Health Pathfinder. While improving data collection methods was an important part of Health Pathfinder, our view of what constitutes “evidence generation” is necessarily more expansive, including clinical and professional knowledge, evidence of effectiveness and breadth of impacts on victim-survivors, and the communication to professional peers of this knowledge and evidence.
One of the intended purposes of the logic model (see Melendez-Torres et al. 2021, p. 9) was to create an evidence base to inform future decisions relating to funding of services, assessing needs and monitoring reach. These data are particularly important to support action on health inequities, either in access to the whole-health response or in onward referral by professionals and uptake of services by victim-survivors. Most of the sites mentioned challenges from sub-optimal or poor data capture systems: The data collection side of things was really challenging, because we have a system in the council that we use to sort of gather all our data, where we view all our casework on, but it's not a system that's been specifically made for us, as a domestic abuse service. The reporting outcomes from that … I had to do quite a lot of that manually over a spreadsheet. (P29)
However, in most sites, Health Pathfinder was able to transform understanding about the importance of better data capture and analysis. The extent to which the data collection processes were able to generate evidence was highly context-specific, depending on existing processes, information sharing and records access, perceived needs for different types of data, approaches to data collection, and the possibilities offered by sites’ current resource and infrastructure. While poor existing systems created extra burden on services, it also initiated a process of system improvement in some sites: “Anyone who's wanted to … interface with any of our systems to get any data about benchmarking … it's really almost impossible … I think the senior management have utilized the fact we’re doing the Pathfinder … and somebody's just been appointed to really look at all of that and improve our systems” (P13).
However, in some sites where the need to improve data collection systems was flagged, the demand to use other tools was either too resource-intensive or outside the power of professionals involved in Health Pathfinder, resulting in additional burden. Furthermore, in two sites, interviewees felt that the time period of the intervention was too short to establish more appropriate reporting systems: “I can't really give you anything to evidence change at this moment post-Pathfinder because … in this time period that we’ve been working with Pathfinder which is a relatively short cycle, it seemed very much about actually getting the infrastructure and the foundation right” (P9).
Co-located DVA services and victim-survivors alike argued that the evidence generated should focus on less readily quantifiable outcomes and should accurately represent workload of health-based DVA services. In particular, IDVAs voiced their frustration that evidence of their work was not accurately captured through existing data collection processes: I mean we'll hear from sort of top management that you're saying you're very busy, you're overwhelmed … but your stats, you know don't show all these outcomes. And because with a lot of the clients that we work with actually a lot of them are not at that stage … it's such a long process. Sometimes they can be with the service for a year and all you're doing is talking to them and empowering them. And those are the things that are not being recognised or acknowledged or captured. (P28)
Victim-survivors presenting at an earlier stage of change pointed out that although DVA service involvement did not result in leaving the relationship, the support and help they received was beneficial and generated improved trust in health services, demonstrating the difficulty of capturing this nuance within existing systems: “I have my emails and messages that she has texted, she has sent the link [to the DVA Service] but I haven't attended any [of their programmes]. It's not her fault, it's up to me if I go or not … I think they’re doing their job perfect” (S15).
These views reflect that the positive effects of Health Pathfinder may not be readily quantifiable in terms of victim-survivors’ access to a wider array of services, greater readiness to take up services, improved wellbeing, and health services’ greater readiness and responsiveness to the needs of victim-survivors across the system. These are all important outcomes that are crucial for addressing health inequities. As one professional described, the amount of supporting and consulting work, particularly for victim-survivors with complex needs, was not readily captured by data collection systems: It's not entirely representative of the number of clients we support, with a mental health support need… [With some cases] I’ve done a lot of work, working directly with the care coordinators, or managed to see a client once, like that might have taken ages… Or you might be doing a lot of work behind the scenes, that doesn't necessarily get caught on these systems. So, a way forward, might be actually to record the amount of time you spend, on calls, or through how many consultations and things like that, that might help to record how much work you do. (P29)
This mechanism was the most challenging to implement but appears to be the most important for evidencing effectiveness to sustain the intervention long-term. The evidence generated clearly needs to be adapted, expanded, or improved to acknowledge that the co-located DVA role encompasses more than practical, quantifiable outcomes. It also highlights the importance of generating an evidence base, which accurately reflects whether and how their roles meet victim-survivors’ individual needs.
Discussion
In this paper, we drew on interviews conducted with health professionals and victim-survivors to provide an explanatory account of how the Health Pathfinder intervention achieved its intended outcomes. Our aim was to make a much-needed contribution to the literature on understanding how DVA interventions achieve their impacts, for whom, and in what circumstances, by using evidence to contribute to a program theory, which can then be used as a framework to guide future research in this area. The first key aspect of the theory is that initiating a “whole-health” response to DVA requires that five distinct mechanisms be utilized, each of which requires multiple roles and partners working across multiple levels of health systems. The second theoretical insight from our research is that these mechanisms tend to unfold sequentially, with each paving the way for the subsequent one. Thus, early successes form the backdrop for subsequent positive changes and, conversely, early impasses left unresolved create contexts which can derail progress. Finally, our program theory demonstrates why one mechanism alone is “not enough” to drive forward change across an entire system. All the components and roles in the Health Pathfinder ecological intervention had to work together to transform how the health system responded to DVA in each of the eight sites. Our program theory offers insight into how critical pathways for reducing health inequities experienced by women, particularly women who experience multiple forms of oppression, can be established and maintained. Although derived from research in the British healthcare system, its utility extends to other jurisdictions and areas planning system-level change.
Awareness raising was shown to be the crucial first step in facilitating disclosures, in relation to both health professionals and victim-survivors’ understanding of health's role and responsibility in DVA. For victim-survivors, posters and leaflets were identified as a powerful way of raising awareness and communicating this (Pederson et al., 2023). For health professionals, training and education were fundamental aspects in raising health professionals’ awareness. Lack of training and education have previously been highlighted as barriers for identifying victim-survivors of DVA in health (Kirk & Bezzant, 2020), underscoring the importance of these components in Health Pathfinder and the need for mandatory training and education across the health system. In addition to training, informal coaching and co-location by on-site DVA services helped generate the expertise amongst professionals surrounding safe enquiry and disclosure, highlighted as important by victim-survivors. This included approaching victim-survivors in nonjudgemental ways, believing and validating their experiences, and communicating empathy (Hegarty et al., 2020).
However, our findings show that education and training alone are not sufficient, with positive collaborative relationships between health professionals and specialist DVA services key to ensuring clear referral pathways, which can empower professionals to act. Indeed, knowledge of local support services (Ramsay et al., 2012) and clear referral pathways have been shown to be central tenets for initiating professional action in other related research (Dowrick et al., 2021). Strong partnerships were crucial for negotiating and integrating shared responsibility for DVA between health and DVA services. However, multiagency relationships needed to exist at both operational and strategic levels to drive and champion action on DVA, highlighting the importance of building relational infrastructure across all levels to effectively address DVA (NICE, 2014).
Evidence generation in sites was highly context-specific, depending on existing processes, information sharing and records access, perceived needs for different types of data and approaches to the collection of these data, and the possibilities a particular site's infrastructure and resources presented. However, the value of quality data collection and collation were felt to be necessary for improving the quality of, and justifying the need for, a whole health response that addresses the needs of victim-survivors. Health Pathfinder sites, each working in a different set of contexts, started the journey at a different point in the implementation process. Similarly, at the conclusion of the project, sites were at different stages of the process, with some sites planning for the evidence creation stage and others still focusing on building and sustaining relationships. Though our model suggests gradual unfolding of mechanisms, we also found significant bidirectional movement between adjacent mechanisms. For example, awareness informed expertise, which then increased awareness through diffusion of expert knowledge throughout organizations. In addition, where health professionals felt empowered to ask and act about DVA, this in turn improved relationships with DVA services. This illustrates the perpetual nature of mechanisms, moving back and fore adjacently, serving to continually strengthen each one.
Limitations
There are some key limitations to note. Delays in local approvals meant that not all sites had the same amount of time to recruit victim-survivors and health professionals to the study. This, coupled with our reliance on gatekeepers to approach potential participants, led to variation in the number of both types of interviews between the sites: we were unable to meet the recruitment targets in some sites and able to exceed them in other sites. Consequently, each of the eight Health Pathfinder sites is not equally represented in the qualitative data. However, the achieved sample is representative of the range of healthcare roles across different health settings, as well as victim-survivors with diverse risk needs and DVA experience.
The number of sites involved in Health Pathfinder, and the resources available to us, meant we were unable to undertake any directed sampling strategies for health professional interviews within each site, focusing instead on the diversity of experiences across our entire sample. Additionally, due to strict safety protocols for recruiting and interviewing victim-survivors, we were unable to theoretically sample across sites or to include factors such as ethnicity or context of DVA explicitly in sampling decisions. However, we used contextual information to sensitize our analysis to key axes of variation between victim-survivors. Additionally, although we initiated recruitment after a period of intervention implementation, sites were at different stages of implementing the intervention, which may be a latent factor in results.
Conclusion
Health Pathfinder is a truly complex intervention, bringing together a multitude of initiatives spanning sectors and agencies to achieve a range of outcomes. Our realist account shows key contextual factors were relevant for understanding effectiveness and suggests Health Pathfinder is an effective ecological intervention by generating awareness, expertise, relationships, empowerment, and evidence over multiple levels in each organization. Positive progress in respect of each mechanism had meaningful impacts on victim-survivor experiences of enquiry, disclosure, and uptake of services and had the potential to meaningfully impact health inequities.
Recommendations
Effective training and clear referral pathways: Training is necessary to upskill professionals to fulfill their role in DVA. However, this must be complemented with effective referral pathways to partner agencies that can provide victim-survivors with the necessary support (e.g., referring from mental health services to DVA services). Health organizations should enhance awareness of their responsibilities for DVA by publicizing health's role, providing leaflets and posters in the waiting areas, to enhance victim-survivors’ awareness of how health can help.
Co-location of services: In addition to prior work (e.g., Dheensa et al., 2020; Halliwell et al., 2019; SafeLives, 2016), these findings also evidence the value of co-location of services, especially when the necessary partnership agreements, protocols, and practical processes are agreed and in place beforehand. However, Health Pathfinder also shows that co-located services need to be visibly integrated into the health environment, working closely with a coordinator or champion within the NHS with a specific remit to drive action on DVA.
DVA in health policies: DVA is the core business of the NHS and must be recognized in policy documents across all specialisms in all NHS trusts. Policies should clearly communicate the roles and responsibilities of partner agencies underpinning the initiation, support, and governance of Health Pathfinder specifically, as well as clearly communicating the healthcare response to DVA more generally.
A central concern for structural inequalities: Cutting across each of the previous recommendations, a concern for how structural inequalities affect victim-survivors, and the potential of the whole health response to meet and ameliorate these structural inequalities and thus impact health inequities, is important to create a response that is effective in meeting the needs of all women who are victim-survivors of DVA. Greater recognition of diversity, both where this is represented in the population taking up services and where that diversity is “masked” by barriers to uptake, is a central component of a whole-health response that works for all victim-survivors. Further research is recommended to extend our understanding of the impact of Health Pathfinder on victim-survivors with specific vulnerabilities or protected characteristics.
Footnotes
Acknowledgments
The authors would like to thank the Health Pathfinder Consortium for funding this evaluation and for their help and support throughout the conduct of the evaluation. We would also like to thank the victim-survivors who bravely shared their stories and the health professionals who gave their time to share their experiences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.