
Abstract
This 24-month inductive study examined the practices provided by a variety of supporters to six frontline-led innovation teams. Analyzing 86 interviews with 35 team members and 17 supporters, we propose a comprehensive, idealized framework of dynamic and multisource support. These practices offered critical aid as teams dealt with limited innovation experience, limited relationships, and limited contextual awareness. We categorized the practices we identified into six sets—Ensure Foundational Support, Transmit Knowledge and Skills, Nurture Teams and Teamwork, Cultivate Relationships with Decision-Makers, Scaffold Project Work, and Foster a Holistic View of Innovation Work—and discussed their benefits and boundaries of effectiveness. Our framework challenges the notion of “one-size-fits-all” support, emphasizing the value of adaptive support instead. We also highlight the critical role of coaches and identify significant roles unexpectedly played by the funder, insurer, student fellows, and research-observers that provided instruction, resources, and encouragement.
Keywords
Introduction
Health care organizations increasingly rely on frontline-led innovation teams to improve care delivery and employee morale (Atkinson & Singer, 2021; Jung et al., 2024). Frontline-led innovation teams involve clinicians, staff, and managers who are closest to care delivery and, thus, most aware of improvement opportunities and how they can be implemented well (Jung et al., 2023; Satterstrom et al., 2021). Innovation entails identifying problems and then generating, testing, and implementing solutions, which encompass activities related to process or quality improvement (QI) (Jung & Cummings, 2023). We use the terms innovation and quality or process improvement interchangeably. These bottom-up efforts complement top-down efforts, which are dictated by policy or institutional changes (Stouten et al., 2018). To ensure frontline teams live up to their potential, they need to be properly equipped and supported.
Individuals and groups provide various forms of support to help frontline-led innovation teams deal with numerous barriers (Rushton et al., 2023). We describe anyone providing such support as a “supporter.” Supporters help innovation teams when they are stretched by core tasks, have limited exposure to improvement methodology and mindsets, and work in hierarchies and silos that hinder some team members from fully participating in innovation (Atkinson & Singer, 2021; Jung & Cummings, 2023; Satterstrom et al., 2021). To equip and bolster innovation, organizations have created innovation centers and provided QI training and opportunities to frontline staff, and partnered with federal, state, and local learning collaboratives (Meer et al., 2023). These supporters have engaged in many activities to motivate, facilitate, and sustain innovation teams and their work.
However, less is known about the dynamic and multisource nature of support, particularly who could provide it and when it might be needed. Prior research has described support features that teams found “helpful for advancing their improvement efforts overall and knowledge acquisition,” such as collaborative faculty and learning session interactions (e.g., Nembhard, 2009, p. 359). We build on this work and explore supporter practices that respond to different barriers, who delivers the support, and the benefits and boundaries of these practices, including unintended consequences. Without adequate understanding of how to effectively support innovation teams, support may vary in an unguided way or be provided in a “one-size-fits-all” approach without considering the team’s idiosyncratic context and needs.
In this study, we systematically examined the support practices provided by multiple supporters in response to barriers encountered by frontline-led innovation teams, who provided the support, and how the teams perceived the support. We studied an innovation incubator through which teams interacted with a range of supporters employing a variety of support practices.
Conceptual Framework
Innovation teams require multifaceted support—including resources, motivation, information, task-based knowledge and skills, relationships, structure, and contextual awareness—to function effectively and achieve their goals. Foundational support, such as access to adequate resources, relevant data, and a clearly articulated motivation for engaging in work, is essential for team performance across industries and experience levels (Hackman, 2002). Without such support, even skilled teams may struggle to develop and implement innovations.
The innovation and organizational change literatures have long underscored the interdependence of technical and relational dimensions of work (e.g., Battilana et al., 2010). In the context of innovating health care delivery, research has emphasized the importance of fostering both task and relationship skills in teams by not only leveraging static frameworks but also hands-on coaching (Dixon-Woods et al., 2011; Nembhard, 2009). Innovation teams can use frameworks and methodologies to systematically engage in improvement and innovation tasks—such as identifying the root cause that warrants innovation, generating innovative solutions, implementing validated changes, and scaling and sustaining interventions. The Model for Improvement, developed by the Institute for Healthcare Improvement (IHI), encourages teams to define a clear and specific aim for improvement work, identify measures to track progress and evaluate the impact of the improvement work, and use plan-do-study-act (PDSA) cycles to test, learn, and refine improvement ideas (Langley et al., 2009). Guided innovation communities—including learning and QI collaboratives, incubators, and innovation centers—offer programs to help teams build task-related skills and relationships (Bardach et al., 2024; Cardenas et al., 2023; Nembhard, 2009; Weaver et al., 2015). These communities bring together teams of clinical and administrative staff to enhance problem-solving by combining diverse perspectives on the realities of patient care and workflows, and operational logistics (Atkinson & Singer, 2021; Jung et al., 2024). Nembhard (2009) and other researchers have described features of innovation communities, yet less is known about when and which practices supporters could use across different teams.
Teams—particularly novice teams—also need structures to help scaffold their innovation work (e.g., Cardenas et al., 2023; Weaver et al., 2015). To this end, guided innovation communities often include structured programs that bring together innovation teams from different organizations to address health care challenges (e.g., reduce surgical site infections, improve safety culture) and learn from each other (Bardach et al., 2024; Nembhard, 2009). These communities typically encompass a series of meetings, conference calls, or online discussions, allocating dedicated space and time for innovation, away from day-to-day clinical or administrative responsibilities. Such structures allow full engagement of frontline workers in learning how to innovate and carry out the innovation work. Project management skills or roles that structure the team’s work by creating plans to ensure timely coordination of tasks and updating plans when the situation changes are also key to team-based innovation work (Edmondson & Nembhard, 2009).
While innovation work often involves understanding and addressing a particular problem or opportunity, teams also need to hold a larger strategic view of their work. The success of innovation work depends on the policy and financial landscape, and ongoing changes at the national, state, and community levels that can affect reimbursement and workforce issues (Damschroder et al., 2009). To ensure an innovation is sustainable, teams should know what policy levers can be used to save costs and demonstrate improvement. However, many frontline teams lack such a contextual picture, and teams’ frontline and middle managers may be unable to provide a more holistic view for the team. Teams may benefit from a network of experts and community partners that enable teams to obtain technical expertise and guidance to ensure that innovations are evidence-informed and avoid reinventing the wheel by learning from prior work; receive feedback on feasibility, acceptability, and potential unintended consequences; and attain additional funding for project work as needed.
Bringing together such multifaceted elements of support for innovation teams, we offer a comprehensive, idealized framework for supporting innovation teams that builds on prior research and addresses key gaps in existing models. Our framework offers a robust and holistic perspective that extends beyond process change. The sets of support we describe are dynamic and multisource in nature. Rather than solely examining what individual supporters should do, we emphasize the importance of understanding the broad, idealized system of support for teams. Articulating the idealized sets of support practices can enable teams and organizations to proactively assign supporter roles or cultivate them as needed. Moreover, the comprehensive support framework allows teams to tailor the support to their local context, such as a respective team’s prior experience with innovation and the idiosyncratic barriers they may face in their innovation work.
Given the inductive nature of this study, we did not begin with a reference to a specific theoretical framework. Instead, we induced our conceptual framework from patterns that emerged through iterative analysis of the data. This process led to Figure 1, which we present in the Findings section.
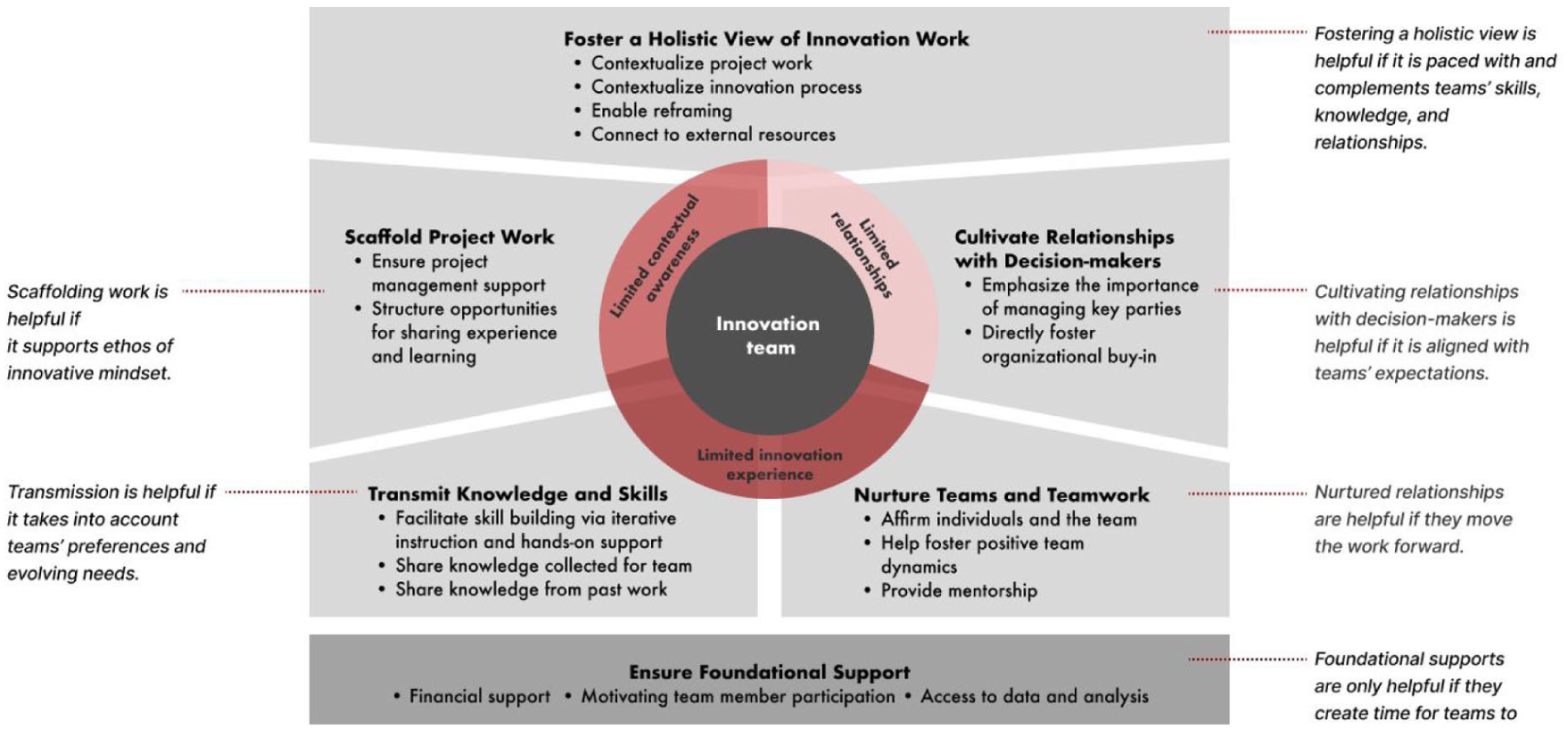
Idealized Framework of Support Practices for Frontline-Led Innovation Teams.
New Contributions
This study makes several new contributions. First, we provide a comprehensive idealized framework of practices for how supporters responsively engage frontline-led innovation teams from onboarding through developing, implementing, and scaling innovations. Using longitudinal interview and archival data, we develop sets of practices that range from providing financial support, affirming individuals and teams, facilitating skill building via iterative instruction and hands-on support, to contextualizing project work. These sets work together to provide a net of support for teams, especially those who have limited innovation experience, limited relationships within and outside their health care organization, and limited contextual awareness for how to engage with innovation work while completing their day-to-day tasks. Second, our findings show that evidence-based methods and support practices are not “one size fits all.” Rather, innovation team members perceived supporters as most helpful when they were responsive, shifting the pace and focus of their support to teams’ multifaceted and dynamic needs. While some barriers, like limited time, were common, other barriers, like limited innovation experience or relationships, were more idiosyncratic, underscoring the importance of supporters’ understanding of each team’s experience of barriers to innovating. Third, we build on earlier work documenting benefits of coaches for innovation teams (e.g., Dixon-Woods et al., 2011). We highlight multiple, often unexpected, sources of support, including the funder, insurer, student fellows, research-observers, incubator advisory board, and community organizations, all of whom engaged in critical support practices.
Methods
Study Context
We followed six interdisciplinary innovation teams in federally qualified health centers (FQHCs) that participated in a year-long incubator designed to help teams generate and implement innovations to improve patient care while lowering costs. Three teams participated from 2021 to 2022 and three teams participated from 2022 to 2023. Team members included senior leaders, middle managers, and frontline clinicians and staff, such as physicians, nurse practitioners (NPs), nurses, medical assistants (MAs), and call center agents. The incubator provided training, coaches, and data, and a US$150,000 stipend per clinic to offset personnel time to engage with innovation work.
The incubator provided a range of “supporters” that included: experts who offered support based on years of clinical and QI experience (“content coaches”), with two of the content coaches serving as incubator leaders; experts who taught teams human-centered design principles and supported teams as they learned to use this methodology (“process coaches”); and medical and business students from the organizing university (“student fellows”). Other supporters included researcher-observers, a managed care organization (“insurer”), the incubator’s private funder, and the incubator’s advisory board. The incubator organized didactic and shared learning sessions, presentation workshops, and opportunities for teams to present their work to internal and external parties. Each team, with input from clinic leadership, selected the problem/opportunity to focus on, e.g., funding and spreading a behavioral health add-on service, preventing unnecessary emergency room visits, and increasing patients’ portal use. Perhaps because of the depth of resources, all teams completed the program and made progress on stated goals. The teams and supporters worked via a mix of in-person, online, and hybrid meetings. The incubator offered similar support across the two years with the exception of an in-person launch event in the second year.
Data Collection
This study was part of a larger project that gave us access to recordings of the teams’ work meetings, meetings with supporters, and archival data, such as teams’ application materials to the incubator and presentations about their work throughout the teams’ innovation work. We conducted interviews of team members and supporters that were informed by our observations of the teams’ meetings, incubator leaders’ meetings, didactic sessions, and presentations.
Over 24 months we conducted 85 interviews: 50 with 35 team members and 35 with 17 supporters. The supporter interviewees included four content coaches, three process coaches, six student fellows, and three employees with the insurer (CEO, data analyst, project manager), one incubator project manager, and one funder. We had the opportunity to interview some team members and supporters multiple times (e.g., at the beginning, middle, or end of the year’s program) depending on the individual’s availability. All interviews were conducted on Zoom. During the interviews, we sought to understand the kinds of support that were provided and how teams and supporters experienced the support provided. We developed our interview questions based on our observations of team meetings (see Appendix for a sample interview guide).
Analysis
Our analysis involved four stages. In the first stage, we wrote memos and engaged in extensive discussions about the six teams (anonymized to Teams Coral, Emerald, Maroon, Orange, Teal, and Beige) and their supporters (anonymized using Roman numerals) based on our observation of team meetings and presentations, as well as our interviews with the teams and supporters. We were struck by the different types of support the teams received—some of it expected and some not. This led us to review the literature to better understand what is known about supporting multidisciplinary frontline teams engaging in innovation work. In the second stage, we tried to better understand the support provided by each role and the incubator programming. This involved compiling a preliminary list of support practices by supporter role, which included going back to the data to create descriptions of each practice. For example, we saw in meetings, and noted during interviews, that process coaches imparted skills related to the human-centered design process and teamwork (“facilitate skill building”), role modeled interpersonal skills to elicit participation and manage disagreements (“help with team dynamics”), and validated team members’ strengths and efforts (“affirm”). Those formed the support practices for process coaches. We also noted that the funder gave inspirational talks to teams (“motivate teams”) and financed the incubator to defray the cost of team members’ time (“provide financial support”). Those formed the support practices for the funder. These preliminary support practices by supporters became our initial codebook. In the third stage, we used the initial codebook to first code four interview transcripts from interviews with a process coach, content coach, student fellow, and clinic team member. Through this process, we refined the codebook and standardized our coding work. Next, we divided the remaining transcripts among four authors to code using the codebook. All authors met weekly to discuss the coding progress and questions that arose while coding, which helped us to further refine and iterate on the codebook. During coding, we saw that some practices were thematically similar and enacted by multiple roles, so we grouped the categories into different sets. While we saw these practices occurred throughout the study period, some practices were more foundational than others. In the fourth stage, we further explored the responsive and dynamic nature of the support practices that supporters provided in response to the various barriers that teams encountered in their innovation work. We organized the support practices that responded to specific barriers. For example, we observed limited relationships among team members of some teams (as members came from different roles, departments, and positions) that hindered the team’s work, and supporters would help foster positive team dynamics in response. We also observed limited relationships between some teams and their organization’s senior leaders, and in response, supporters would emphasize the importance of obtaining buy-in from key parties or cultivate buy-in on behalf of the team. We noted that while teams viewed these practices as beneficial, they did not always uniformly view them that way. We indicated the shortcomings of the practices and of how they were implemented.
Results
The teams we observed varied in their experience with innovation work. Some teams had members with no innovation experience, while other teams had one or more members with innovation experience. Even among those with innovation experience, however, members differed in which methodologies they were familiar with (e.g., human-centered design, IHI toolkits, lean methodologies). Teams also varied in their access to senior leaders, external partners, and other key parties. Some teams included senior leaders or middle managers, while others were composed entirely of frontline employees with limited experience in partnering with or influencing others. Finally, most teams struggled with how to fit innovation work into the broader context of their day-to-day work.
Figure 1 depicts an idealized framework of support for frontline-led innovation teams. We characterize the sets of support that can be enacted for teams with varying levels of limited innovation experience, limited relationships, or limited contextual awareness. We depict the types of support that helped innovation teams push forward new programs and processes, including Ensure Foundational Support, which encompassed financial and data support; Transmit Knowledge and Skills that helped teams learn how to use innovation frameworks and methodologies; Nurture Teams and Teamwork that helped teams work more effectively together; Cultivate Relationships with Decision-Makers that helped teams get the buy-in needed to carry out their work; Scaffold Project Work that ensured teams had necessary structures for innovation work; and Foster a Holistic View of Innovation Work that oriented teams to their work and context while helping to build an innovation mindset. These sets of support acted in concert to respond to teams’ needs as they faced initial barriers and ongoing challenges. We also describe when and how these support practices helped the team.
Ensure Foundational Support
We have a growing health analytics unit that can help provide feedback on what’s working or what’s not working. But really, I think foremost it’s [the insurer] functioning as a trusted partner to the health centers, being with them and showing support and encouragement, providing feedback that we can on their performance.
Benefits and Boundaries
These foundational supports were critical to ensure that innovation teams had the resources and motivation to learn and make progress; without these, we expect team member participation to have collapsed under the weight of their day-to-day work. Yet while funding was critical to support team members’ time, all team members we observed still struggled with time constraints. They had to prioritize their clinical or administrative responsibilities during working hours and engage with innovation work during early mornings, lunch breaks, evenings, and weekends. Those who had administrative roles were able to more flexibly manage their schedule. Those who worked directly with patients became overwhelmed more quickly; it was therefore critical for their organizations to provide them with meaningful adjustments (e.g., be taken off from other projects, cross-training staff to step in for them in the clinic) even if they were unable to hire temporary replacements due to national staff shortages.
With the insurer’s data provision, while teams found this support critical to their ability to determine problem areas and evaluate their work, getting fine-grained data specific to their project was often difficult. When teams needed data that deviated from standardized report templates, preparing such data required time, effort for the analysts at the insurer, and ongoing communication between teams and the insurer, creating obstacles to data sharing. One team was able to work around this by partnering with epidemiologists from local agencies and universities.
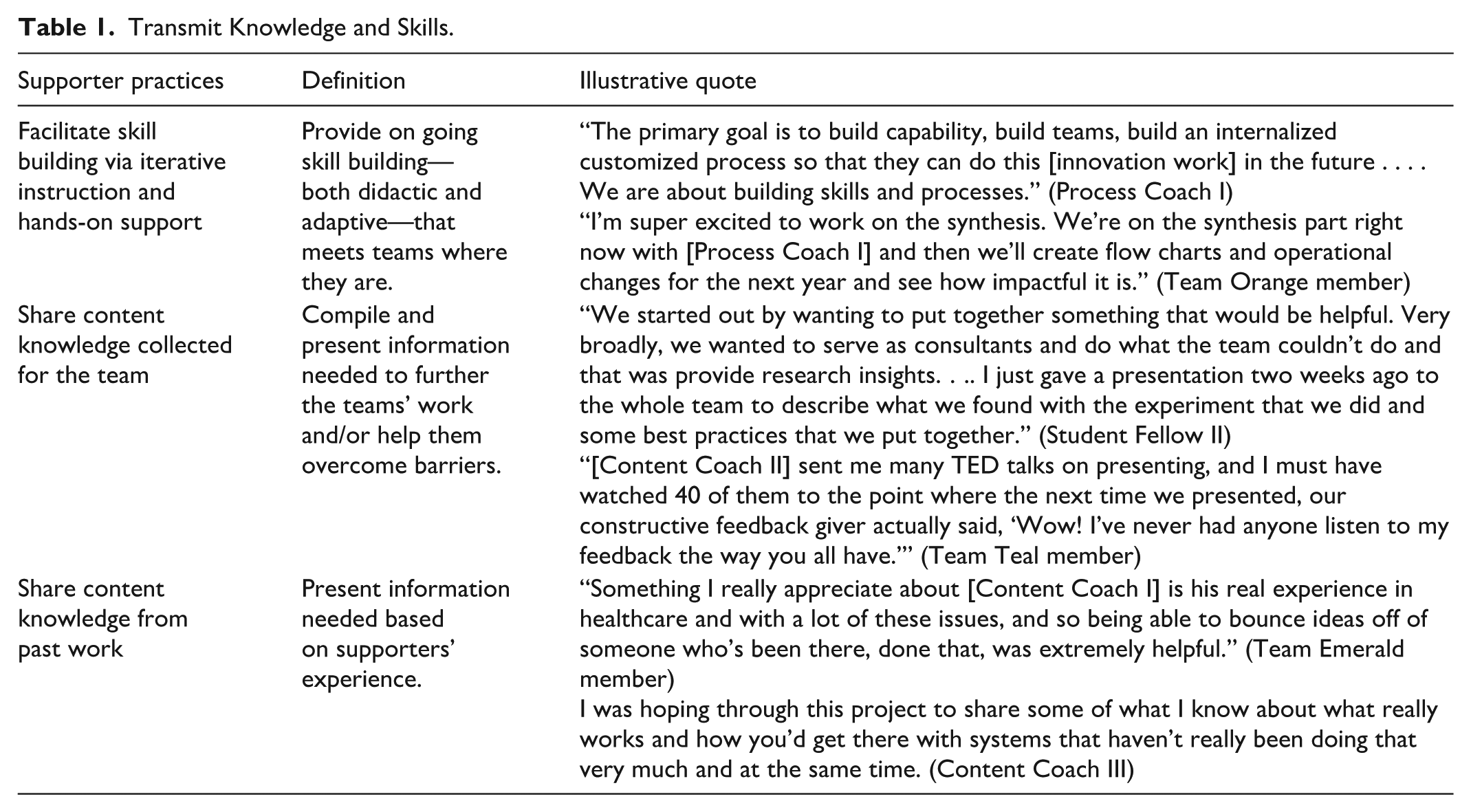
Transmit Knowledge and Skills
This set of support practices responded to teams’ varying experience with innovation work. Supporters helped teams gain shared knowledge and skills to conduct innovation work. Table 1 describes these practices, who enacted them, and illustrative quotes.
Transmit Knowledge and Skills.
I remember we made three teams: somebody takes charge of patient interviews, somebody takes charge of expert internal interviews, and someone takes charge of clinician interviews . . . . I’ve been forceful about saying, ‘Here’s how to break this task up into chunks.’
Process coaches also role-modeled and engaged in ongoing work to help the teams learn skills and tools that matched where they were in the process. A Teal team member said: [Process Coach III] is a magician. She can go in on the Miro board, move things around, take our ideas and cluster them together . . . . not something beautiful–she was very clear about that. The goal is not to make it pretty but to cluster our ideas together and data together, to produce the path ahead.
Given teams’ limited time, they appreciated hands-on support through which they learned how to use new tools for the first time. Team members commented that, while didactic instruction was helpful, it was critical to have help applying the learning to their own idiosyncratic context.
Benefits and Boundaries
Teams welcomed the new skills they were learning; however, some teams embraced and applied the content knowledge that the supporters provided, while others felt that such support took time away from their project work or was not always applicable to their context. A team member highlighted this tension: [Content Coach I] has strong opinions about our specific topic, so we’re trying to balance his opinions with some ideas we have. Staying open minded to the things that he’s saying, while also not letting some of his personal preferences sway us.
Supporters similarly felt tension between letting teams discover how they wanted to proceed and providing input. Coaches varied in their willingness to learn alongside team members– some were willing to expand their repertoire and approach to be responsive to teams and their context, while others focused on what they knew to be best practices.
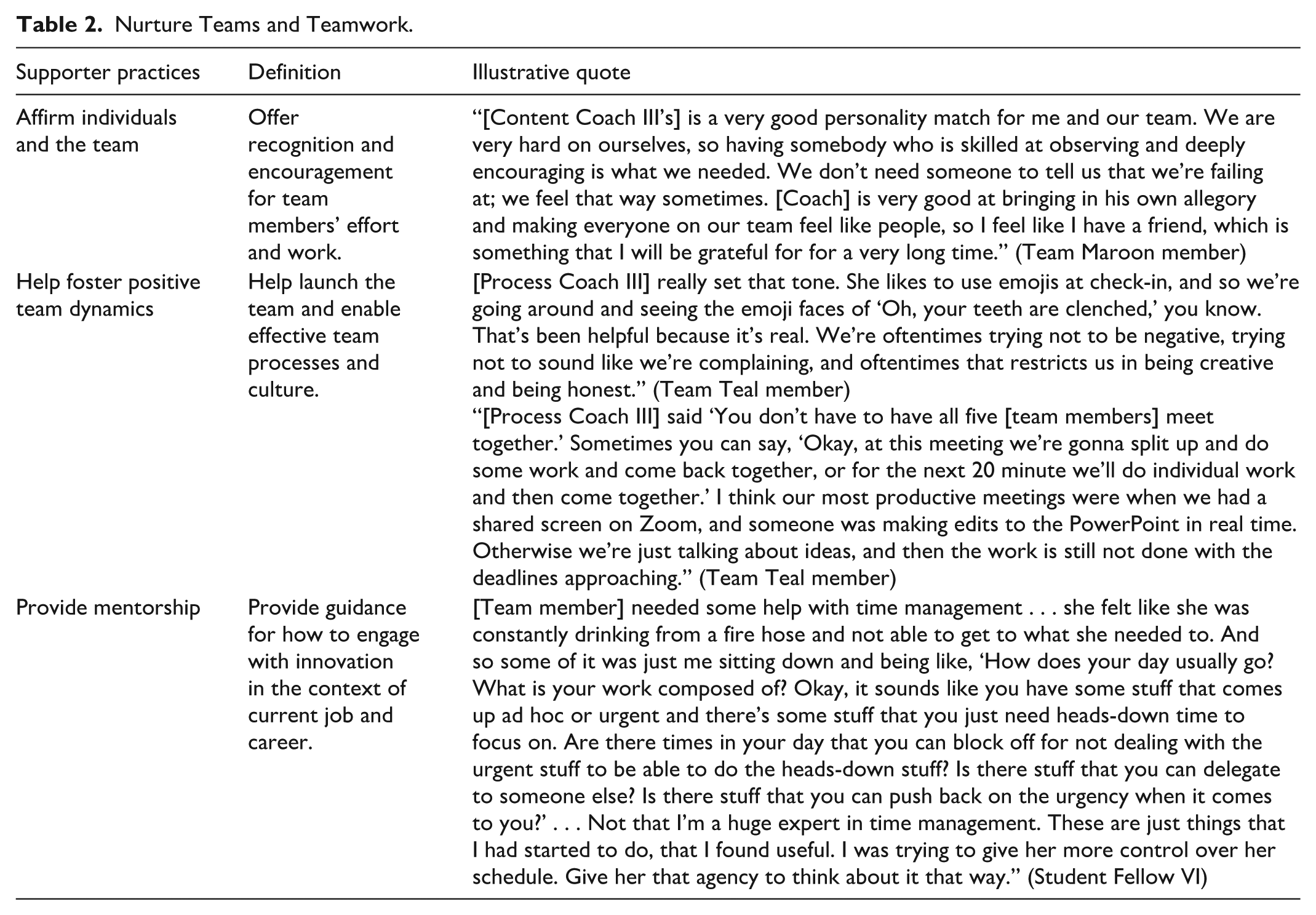
Nurture Teams and Teamwork
Teams benefited from support that responded to their emotional and social difficulties (Table 2). Often, team members were new not only to one another but also to the kinds of roles represented on the team.
Nurture Teams and Teamwork.
She had a way of doing our check-ins, making sure that everybody got to speak their piece, and that was a game changer . . . . Everybody had their 5- to 15-minutes, and she kept everybody accountable for what our responsibilities were for the next meeting. After that it was just a wildfire, but in a good way. It just blossomed, exploded.
A Team Maroon member shared her experience with a process coach, [Process Coach III] is very skilled at observing team dynamics and navigating around hitches on the road. That’s something that we relied very hard on her for. Our team needed somebody to say, I see this dynamic is happening, don’t get discouraged by it, this happens all the time, just keep going. Or I see this dynamic is happening, I have an idea, let’s try this.
Benefits and Boundaries
Team members expressed appreciation for affirmation and troubleshooting team dynamics, especially in the face of uncertainty and tasks that diverged significantly from day-to-day work. A Team Maroon member said that two members from her team would have side conversations with [Process Coach III] who helped work through some of the difficult team dynamics. She gave us suggestions about how to make that shift when things were not working well for us to make progress with our oversized team.
It was, however, difficult to balance time in meetings for interpersonal check-ins with work time. Some teams found a balance by using relationships to further the work, while others began to resent time spent on small talk and exercises that they felt could have been better spent on project work.
Team members described a sense of relief in knowing that they were individually supported when they had questions or concerns about the project, their organization, or careers. A Team Teal member described gratitude at being pushed to take on new work and encouraged to develop skills: [Content Coach II] made it clear from the beginning: he wants to be more of a coach than a leader, so that set the stage for more mentorship and coaching rather than the way I wanted to initially go to him, to just give me instructions . . . Our team was apologetic in our PowerPoint presentation [describes how work shifted]. [Content Coach II] came in and basically said, ‘Own it and present where you are.’ We are evolving. This work is evolving as it should. That really helped us move along, and that’s where we absolutely need mentorship.
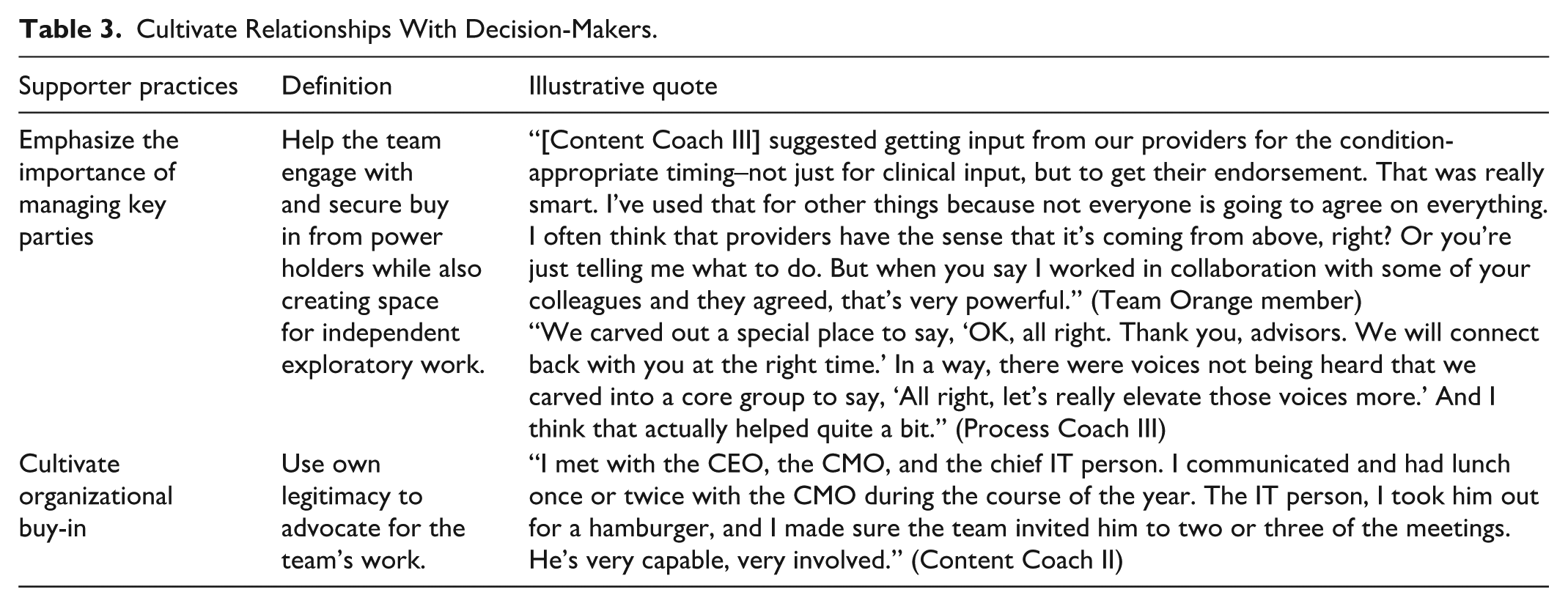
Cultivate Relationships With Decision-Makers
Many team members had no previous experience creating change with peers and leaders Table 3 shows the support practices addressing this challenge. Supporters helped team members build and expand their relationships and influence–sometimes by borrowing legitimacy from a high-status coach.
Cultivate Relationships With Decision-Makers.
The worry I had was that they [senior leaders] had signed up this group but weren’t visibly supporting them . . . I wanted to have a point to meet with both [the clinic CEO and COO], and it turns out that they’re both quite supportive. They hadn’t been in the loop getting all of the feedback as we went. We changed that, and I was impressed that they were supporting the process and they were not going to pull the rug out from underneath the team.
Benefits and Boundaries
Obtaining organizational buy-in was widely recognized as critical by supporters and team members alike; however, actually engendering organizational buy-in was difficult for time-constrained teams. For teams who had regular direct access to organizational leaders, some content coaches chose to let the team navigate those relationships on their own. Other coaches stepped in to ask for more resources, though teams did not expect or desire such support, creating tensions between team members and supporters. Teams composed almost entirely of frontline staff expressed gratitude when content coaches stepped in to advocate on their behalf. However, supporters’ advocacy on behalf of these teams also highlighted the team’s own distance to leaders and their own inability to garner leader support.
Scaffold Project Work
Even as teams learned new skills and cultivated organizational buy-in, they struggled to manage their day-to-day workload along with innovation project work. Supporters helped scaffold teams’ work by providing structured processes and connections that helped teams make progress (see Table 4).
Scaffold Project Work.
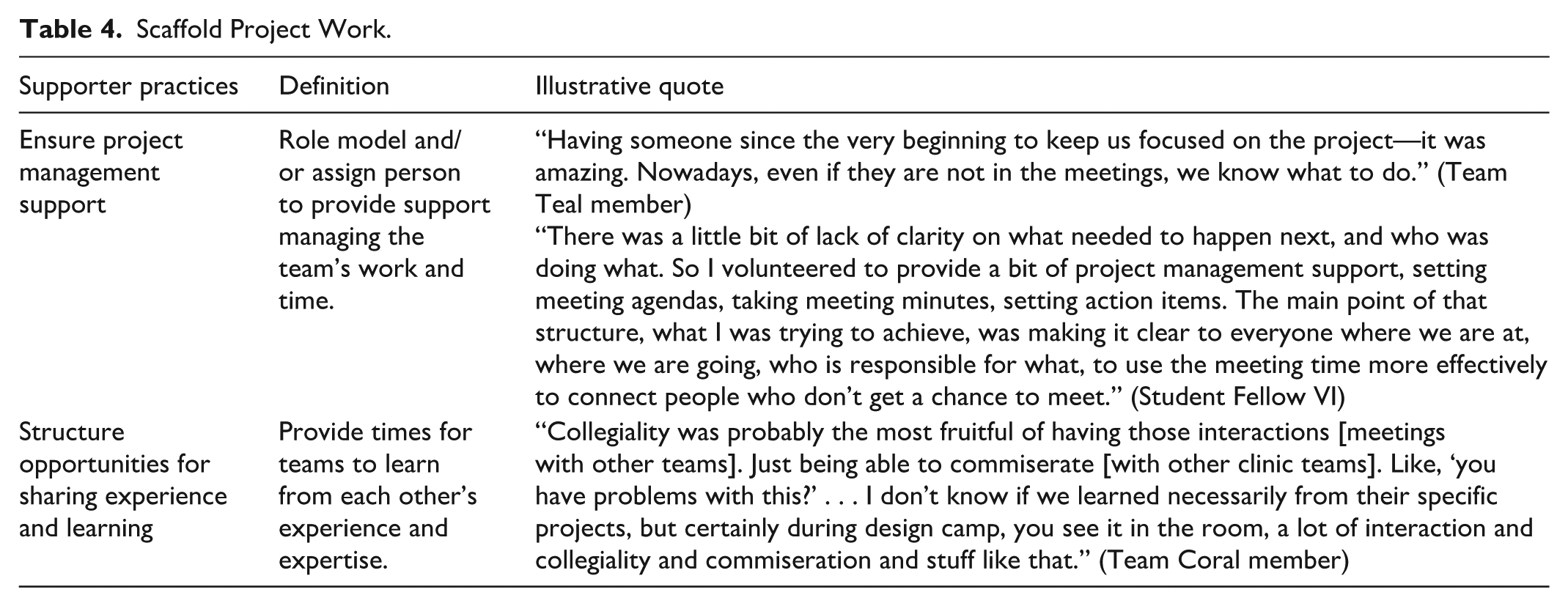
Benefits and Boundaries
While most team member-managers had project management skills, they often struggled to simultaneously contribute as a team member and as a project manager. The project manager provided by the insurer was able to manage incubator-level timelines, but unable to provide hands-on project management support to each team. Those who worked as frontline providers generally lacked project management skills and did not perceive the need to have a project manager on their team, so supporters were critically important in helping them fill this role.
Team members unanimously agreed that having dedicated inter-team time and space for sharing learnings and troubleshooting was helpful and would have appreciated even more time with other teams. However, teams also struggled to tell incubator leaders that they preferred to meet directly with other teams without the coaches.
Some team members became disheartened upon receiving candid and sharp feedback on their presentation from an external expert. These team members felt “sideswiped” after operating in a space of safety. Coaches acknowledged the need for the different types of feedback from different experts but realized the delivery was ineffective, as these experts were not bought into the culture of the incubator. Teams’ perceived need to respond to the external expert’s feedback shifted time and effort away from innovation work and reduced psychological safety. It was difficult for supporters to know how to calibrate feedback so that it was useful but not distracting to the teams’ work.
Foster a Holistic View of Innovation Work
A significant difficulty that resulted from clinics having limited experience with innovation work or experience only with top-down innovation work was that frontline team members generally lacked context of how their project fit within the clinic, within their community, and with industry- and regulation-level changes Table 5 shows the support practices addressing this difficulty. One team did not know about prior organizational efforts to address a similar goal or how their work fit with organizational priorities. Some team members and their managers were not aware of the time and emotional ups and downs inherent in the innovation process. Many frontline team members had limited relationships with others who might have done similar work or had relevant expertise.
Foster Holistic View of Innovation Work.
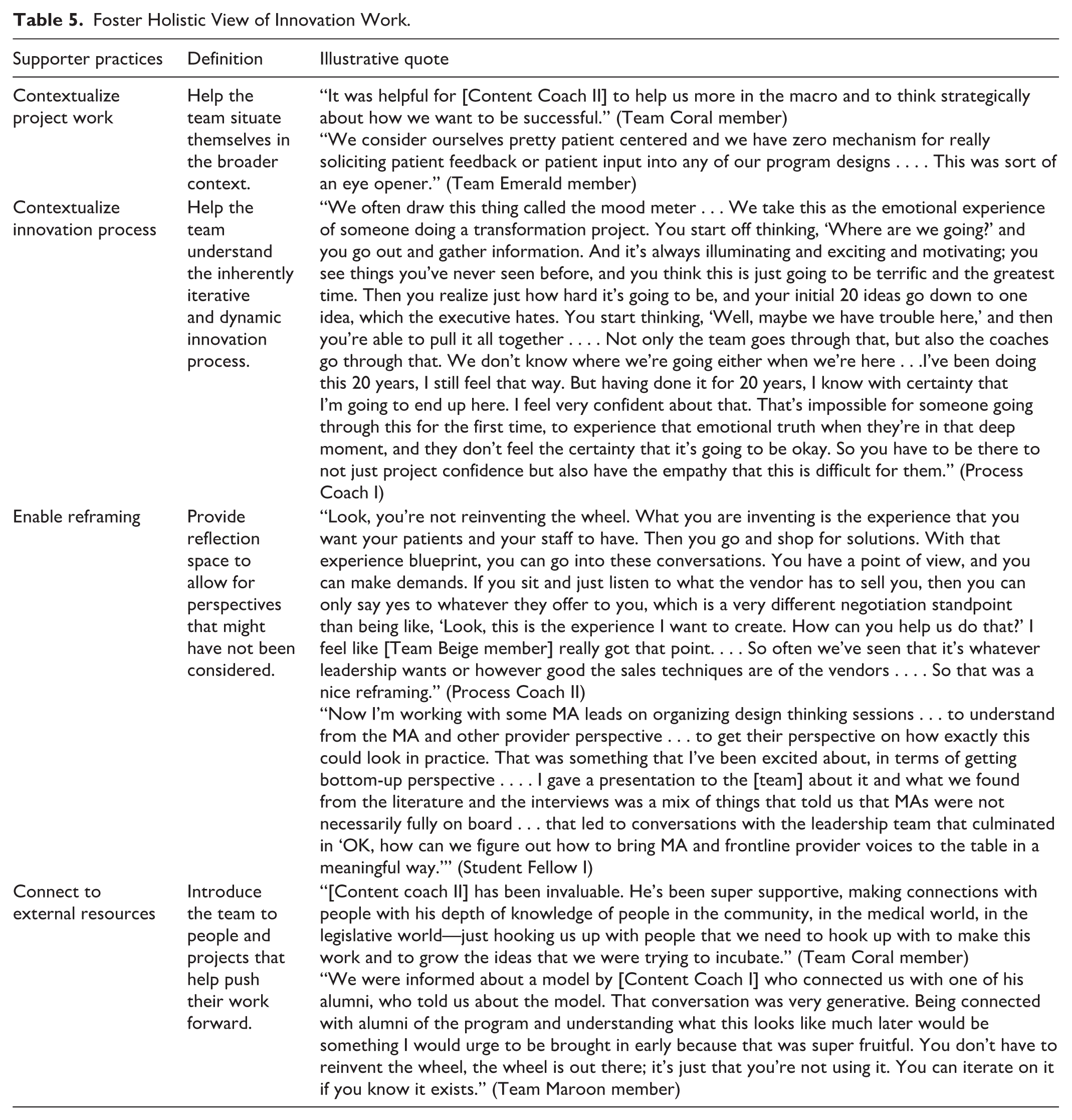
Coming up to our first set of pilots, everyone is very much prepared for them to be a disaster and then regroup and see what we learn and try something else, and just keep tweaking it until it feels like we are making progress.
In gathering research, . . . they come in with lots of new ideas and new systems. One health center has just a QR code on badges and so with patients in front of them, they could scan it with a phone, and there’s your patient education material, rather than let me try and find a printer that works and walk away.
Benefits and Boundaries
By knowing what to expect and being supported through failure, teams were able to focus on learning and trying again. Team members shared that gaining a big-picture perspective and additional support on contextualizing their innovation work and process were valuable. A Team Teal member explained, “This [experience] has helped us to go outside our little borders to learn what’s out there.” However, given their limited time, some team members struggled to absorb the contextual information, engage in reflective activities, and follow up with their new connections, especially if this was their first time engaging in this work. We observed that supporters had to be cognizant of how much individuals and teams could absorb at one time.
Discussion
Dynamic and multisource support efforts across roles and programming are critical for the success of frontline innovation teams. The innovation teams we observed were motivated and hard working. Yet, they were also time-constrained, and many members lacked substantive experience with innovation, with each other and their organizational leaders, and with balancing forward-looking change work with day-to-day work. A “net of support” that included a range of supporters and support practices were critical for teams as they learned and engaged with innovation work.
Our study builds on prior work that underscores the importance of considering the context under which innovation teams operate and the barriers that teams may face at the onset (Rushton et al., 2023). Our findings suggest that supporters needed to be able to read the room and determine when to encourage team building and frame the innovation work in a way that team members did not feel like it was a waste of time. Supporters also needed to determine when to provide advice and when to let the teams work through an issue; when to advocate for teams with organizational leadership and when to step back and let teams make those asks themselves; and when to jump in and help with project management and when to help the team develop the roles and skills to do so on their own. Supporters, however, varied in their ability to read the room and adapt (Satterstrom et al., 2019). For example, coaches who could adjust the pace and provision of content knowledge were viewed as helpful because teams needed this support at select key periods rather than at a steady pace. More work is needed on how to sensitize supporters to understand how to effectively calibrate their support and know when to step back or step up their support.
Our findings illustrate benefits of multisource support of innovation teams. A wide range of supporters helped the six teams make progress on their innovation projects by providing an array of instructions, resources, and encouragements. Such support helped to build not only the team’s capacity to carry out innovation work, but also the relationships that teams needed to be successful. At the same time, however, the support, particularly when it involves different groups of supporters, is necessarily dynamic, messy, and interactive. As more supporters work to enable and empower innovation teams, collaboration and alignment become increasingly difficult and important. More research is needed as collaborative coaching of teams is novel and requires more careful attention, especially in light of differences in team and supporter expertise, experience, and power dynamics.
The multisource nature of support demonstrated the critical role of both content and process coaches, and also identified significant roles unexpectedly played by other supporters. In particular, the student fellows differed widely in their impact, ranging from being seen as not very helpful to being lauded as the most essential support. The wide-ranging degree of helpfulness among student fellows could be attributed to their having the least defined roles. Moreover, having the least experience in these settings (i.e., healthcare clinics) allowed them to contribute fresh perspectives and tailor their support based on observations. While experts are commonly associated with providing helpful support, novices like the student fellows (Zhang et al., 2023) may be untapped high-potential resources for health care innovation teams. Their contributions warrant further study.
Limitations
Our study draws on one incubator, with FQHCs in one state undergoing many regulatory changes. While this context may have influenced the teams’ motivation to engage in innovation—possibly limiting the generalizability of our findings—it also provided a naturalistic setting to observe how teams carry out innovation work. Moreover, the six teams we studied exhibited many heterogeneities—in terms of prior experience with innovation, team size, roles and positions represented on the team, and complexities and scope of the projects they undertook—enhancing the robustness and potential relevance of our findings across diverse organizational contexts.
Practical Implications
Our study has implications for practitioners, especially those who support healthcare teams engaged in innovation work or organize, train, or sponsor supporters. While a wide range of supporters who can role model and provide hands-on support may not be readily available for most clinics, recognizing the benefits of various support practices can help innovation teams overcome their day-to-day barriers and create successful changes to their clinics. Many organizations have recognized the need for a trained QI specialist, and there may be opportunities to tap other roles in the organization. Our findings suggest that teams benefit from having supporters who can help contextualize project work within the larger health care system; help teams navigate organizational goals, policies, insurance plans, financial expectations, and other knowledge that frontline teams might not otherwise by privy to; or bridge frontline teams with organizational functions like information technology or external key parties like the insurer and the local public health department. Moreover, our findings suggest that information and expertise could arise from unexpected sources. Student fellows, who had the least defined roles and most limited work experience, were able to bring fresh perspectives and tailor their support to what they observed.
Teams that do not have the time for innovation work may feel burdened by support that they cannot afford to benefit from and may create resentment and additional stress. At a time when clinics are struggling to attract and retain frontline staff, there is recognition that giving people the opportunity to learn new skills, improve their workplace and patient care, and have a say in organizationally meaningful decisions can alleviate burnout (Jung et al., 2024; Kerrissey et al., 2022). Yet, if this work and associated support add to employees’ day-to-day work, requiring them to work nights and weekends, it may end up exacerbating burnout. This study was conducted in FQHCs, where, as in other resource-strapped organizations, financial support was needed to create the bandwidth necessary for innovation teams comprising frontline clinicians and staff.
Reflecting the work of Hackman (2002) and Ancona and Bresman (2007), team support structures should be designed with multifaceted goals, so that supporters are able and understand how to help teams with project work, help teams develop their ability to work together, and help team members develop individual skills. Yet balance helps. On one hand, too much support may feel frustrating if it impedes progress on innovation work and limits teams to working within existing models and methodologies. On the other hand, too much focus on getting work done and too little support can hinder building capacity, requiring longer ongoing support, and teams may default to working in a hierarchy instead of as a team and spend their time “rediscovering the wheel.”
Footnotes
Appendix
We created slightly different interview guides by role and time period. Below is a sample guide from our
Acknowledgements
We thank the supporters and participants of the incubator who generously shared their time and thoughts for this study. We appreciate Eric Singleton’s insightful and expert input that went into designing our figure. We also thank Sally Retecki, Ingrid Nembhard, Chris Rubeo, and many others who gave thoughtful and critical feedback on this study at the Relational Coordination Collaborative’s 14th Annual Roundtable.
Ethical Considerations
This study was approved by the institutional review boards at New York University, Emory University, and Stanford University.
Consent to Participate
We sought and obtained written consent from participants at the start of their engagement with the incubator.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge funding from Stanford Medicine’s Clinical Excellence Research Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data from this study are not publicly available but are available from the authors upon reasonable request.