
Abstract
To foster bottom-up innovations, health care organizations are leveraging interdisciplinary frontline innovation teams. These teams include workers across hierarchical levels and professional backgrounds, pooling diverse knowledge sources to develop innovations that improve patient and worker experiences and care quality, equity, and costs. Yet, these frontline innovation teams experience barriers, such as time constraints, being new to innovation, and team-based role hierarchies. We investigated the practices that such teams in federally qualified health centers (FQHCs) used to overcome these barriers. Our 20-month study of two FQHC innovation teams provides one of the first accounts of how practices that sustained worker engagement in innovation and supported their ideas to implementation evolve over time. We also show the varied quantity of engagement practices used at different stages of the innovation process. At a time when FQHCs face pressure to innovate amid staff shortages, our study provides recommendations to support their work.
Introduction
Federally qualified health centers (FQHCs) serve as the backbone of the health system in the United States, providing primary care and supportive services for underserved populations and areas (Health Resources & Services Administration [HRSA], 2023). In the last few years, FQHCs have faced unprecedented and enduring challenges: to meet the needs of both patients with increasingly complex health and social needs (Corallo et al., 2020; Quiñones et al., 2022) and frontline staff experiencing physical and emotional exhaustion from their work (Longo et al., 2023). These challenges point to an imperative to (1) capture the voice of frontline FQHC staff—who regularly and directly interface with patients and workflows and do not hold senior management positions—as they are intimately familiar with improvement needs and opportunities (Jung et al., 2023) and then (2) innovate, or develop novel and useful ways of working to improve organizational outcomes such as care quality and costs and patient and staff experience (Greenhalgh et al., 2004).
To foster bottom-up innovations that help health care organizations better serve patients and frontline staff, some organizations have relied on interdisciplinary innovation teams (e.g., Atkinson & Singer, 2021). These teams comprise frontline staff representing a variety of hierarchical levels and professional backgrounds, enabling them to pull from diverse knowledge sources to gauge what may be most impactful (Jung et al., 2023; Tucker & Edmondson, 2003). Prior research suggests that interdisciplinary innovation teams have the potential to implement process changes that positively impact organizational outcomes and help employees feel heard (Atkinson & Singer, 2021; Kerrissey et al., 2022; Satterstrom et al., 2021).
Despite their potential, interdisciplinary innovation teams in health care contexts face challenges. Prior research conducted in hospitals and health systems notes that frontline staff are already stretched thin with core tasks, leaving no bandwidth for other activities (Tucker & Edmondson, 2003). Innovation team members may also vary in their level of exposure to change methodology and mindsets, with some team members engaging in change work for the first time, requiring training and coaching in innovation (Lozano et al., 2022). Furthermore, these teams may mirror the hierarchy and silos found in many health care organizations, limiting members who sit lower in the hierarchy from speaking up (DiBenigno & Kellogg, 2014; Nembhard & Edmondson, 2006). Even when they do speak up, Satterstrom et al. (2021) found that ideas voiced by lower-level team members (e.g., medical assistants [MAs], front desk staff) were rejected at higher rates than higher-power members (e.g., physicians and managers), requiring collective efforts for these ideas to reach implementation.
In this study, we explore how newly formed interdisciplinary innovation teams of frontline staff and managers in FQHCs manage their limited time, unfamiliarity with change methodology and mindsets, and hierarchy to take on innovation work. Such challenges may be especially salient and onerous in FQHCs as they face severe staffing shortages and care for patients from underserved populations and areas with complex health and social needs (Jung & Cummings, 2023). We investigate the practices used by teams and their innovation coaches that cultivated and sustained frontline engagement in innovation and supported their ideas to implementation.
New Contributions
Our study makes several new contributions. First, we provide one of the first accounts of how and when teams use practices to engage each other and support ideas through the innovation process. Our data—recordings of teams’ work meetings and interviews—allowed us to uniquely observe how microprocesses underlying the team-engaging practices evolved in accordance with the stages of the innovation process. Second, we offer evidence on when during the innovation process these practices were in high, medium, and low use, providing a more nuanced understanding of how these practices responded to teams’ needs. Third, our findings highlight the importance of building a foundation for innovation work for many frontline staff and managers who are trained and paid to carry out clinical tasks and may be new to innovating. Fourth, we illustrate practices that make the challenges faced by middle managers visible to team members and the strategies that teams can use to support these managers and prevent the teams’ work from stalling. Fifth, we zoom in on interdisciplinary innovation teams in FQHCs. While FQHCs face pressure to innovate amid simultaneous demands to expand access, provide equitable and affordable care, and improve care quality, prior research on process innovation teams has mostly focused on large, often better funded, health systems (e.g., Atkinson & Singer, 2021).
Theoretical Background
Interdisciplinary innovation teams bring together frontline staff so that they can contribute to developing a new product, service, or way of working (Greenhalgh et al., 2004). Such teams enable bottom-up frontline innovation work, in contrast to top-down efforts dictated by policy or institutional changes (Stouten et al., 2018). In general, health care workers face barriers when trying to engage in innovation. Research on frontline innovation conducted in hospitals and other health care organizations shows that workers’ formal responsibilities seldom include tasks related to innovation; tasks like generating creative ideas, championing ideas, and securing resources to implement them are considered discretionary for workers whose jobs center on care delivery (Jung et al., 2022). In FQHCs where workers are already time-constrained and experiencing burnout (Longo et al., 2023), expecting them to participate in innovation beyond their required job may be unrealistic. Moreover, health care workers who are invited to participate in innovation work must deal with the tension between the nature of clinical work and innovating; while clinical work often requires adhering to standardized protocols, innovating entails experimenting and considering alternatives that are outside of standardized practices (Edmondson, 2008; Gilson et al., 2005). Sustaining consistent clinical work while also carrying out interpersonally risky and unpredictable innovation work implies that workers must switch back and forth between learning and executing mindsets (Singer & Edmondson, 2008). In addition, interdisciplinary innovation teams face hierarchical and heterarchical barriers, imposed by senior managers and professional groups, respectively (Atkinson & Singer, 2021).
Prior research has investigated conditions and interventions that increase worker engagement in innovation and support workers’ voiced ideas to implementation (Satterstrom et al., 2024). For example, the literature on employee voice—“informal and discretionary communication of ideas, suggestions, concerns, problems, or opinions about work-related issues with the intent to bring about improvement or change” (Morrison, 2023, p. 80)—has identified challenges to fostering employee voice, particularly those pertaining to power asymmetries between frontline staff who voice ideas and those who hold the authority and resources to act on the voiced ideas (Morrison, 2023; Satterstrom et al., 2021). However, even when employees manage to voice ideas, only a fraction of the voiced ideas are followed through on and implemented (Satterstrom et al., 2021). Other examples of engaging staff include structured processes to capture worker input. These efforts include Leadership WalkRounds for which hospital executives conduct regular rounds to elicit concerns and suggestions for improving safety, and then link frontline input to operations committees that institute needed changes (Singer & Tucker, 2014); innovation contests that invite all FQHC frontline staff, regardless of their position or organizational tenure, to share ideas and then participate in selecting ideas to implement (Jung et al., 2023); improvement methodologies, such as plan-do-study-act cycles that provide a template for iterative testing (Langley et al., 2009; Taylor et al., 2014); and training on organizational change and quality improvement methodologies (Block & Manning, 2007; Lozano et al., 2022).
However, these efforts tend to focus on one part of innovating, though the innovation process spans generating and speaking up with ideas to implementing of those ideas (Baer, 2012; Perry-Smith & Mannucci, 2017). For example, the voice literature has not deeply examined what happens to voiced ideas and how to help them reach implementation (Morrison, 2023; Satterstrom et al., 2024). Similarly, structured processes that solicit ideas also typically stop at idea generation and selection, rather than seeing the ideas through to implementation (Jung et al., 2022). The use of improvement methodologies has been found to vary, with key principles frequently not followed (Taylor et al., 2014). Moreover, while change tactics used to institute top-down changes (Stouten et al., 2018) cover all parts of the innovation process, they assume that all tactics are equally important, at all points of the innovation process. More research is needed to advance our understanding of the complex dynamics and the nuanced approaches required for ideas to become innovations across stages of an innovation process.
Methods
Study Setting
We partnered with an initiative (the “incubator”) designed to support FQHCs to generate and implement innovations that would improve the health care they provide while lowering overall costs. The incubator was organized and sponsored by a university center and a managed care organization, with funding from a private donor. In 2021, the incubator recruited three FQHCs to participate in a year-long program and provided each FQHC with a $150,000 stipend to offset personnel time and other expenses. Having such support to undergird an innovation process, such as access to training and coaches and carving out time for participation, is not uncommon (e.g., Agency for Health Care Research and Quality [AHRQ], 2015). Each FQHC assembled an interdisciplinary team that could include senior leaders, middle managers, and frontline clinicians and staff, such as physicians, nurse practitioners (NPs), nurses, medical assistants (MAs), and call center agents. Team members were drawn from multiple sites within each FQHC. Two medical students from the organizing university each joined a team.
The incubator comprised three phases. In the first phase, clinic teams went through a 3-month “Design Camp,” which provided an applied curriculum on human-centered design. During this time, teams were coached by professional designers on how to empathically interview patients, staff, and other stakeholders to identify a pressing problem or opportunity, understand its underlying causes from multiple perspectives, and create storyboards and prototypes. In the second phase, lasting 9 months, teams transitioned to experimenting, iterating, and implementing innovations. During both phases, university faculty coaches joined team meetings to provide support. Both phases concluded with presentations to incubator staff, FQHC senior leaders, and other invited guests. After concluding the incubator programming, the clinic teams continued to work on implementation and had monthly check-ins with their faculty coaches to discuss their post-program progress. The design and faculty coaches were considered part of the “incubator staff.”
Data Collection
We conducted fieldwork from September 2021 through April 2023, engaging as observers of three teams and incubator staff, though we chose to focus on only two teams for this paper. Each team selected its own specific aims for its project. The “integration team” sought to improve patients’ psychosocial, as well as clinical, rehabilitation. The “hospital avoidance team” sought to reduce unnecessary visits to the emergency department. The “geriatric care team” sought to improve care for older adult patients. At the time of the incubator, the integration team had identified a behavioral health services provider to partner with and focused on aligning funding mechanisms for psychosocial care during its participation. Two senior leaders worked with private and public payers and sought comparably less input from frontline staff. Thus, we excluded the integration team and focused only on the work of the hospital avoidance and geriatric care teams.
We used longitudinal qualitative methods to better understand how frontline clinicians and staff engaged in innovation work. We drew on multiple sources of data (Yin, 1994), including team meetings, incubator staff meetings, interviews, and archival materials. All meetings and interviews took place on Zoom and were recorded. We used recordings of 132 team and staff meetings and 31 interviews. We interviewed team members, as well as faculty coaches, design coaches, incubator staff, and the program’s funder. Our archival data included materials from the applications that the interested FQHCs submitted to participate in the incubator, meeting agendas and notes from incubator staff and team meetings, diagrams and process models that each team developed on online whiteboards, and presentation slides that clinic teams created to share their work (Table A1 in the Online Appendix shows our data sources).
Analysis
We analyzed our data using inductive, iterative approaches (Charmaz, 2014). We examined the meeting recordings, interview transcripts, and archival materials through multiple rounds of coding, supplemented by a continual review of the literature. In our first round of analysis, we engaged in memo writing about the two teams to better understand the problems they were tackling; relationships between team members and their coaches; and teams’ work practices over time. After observing that teams’ engagement with frontline members varied at different times, we sought to better understand how teams engaged frontline members. In our second round of analysis, we conducted open coding to understand the practices that invited frontline voice in the moment and also used frontline voice and work in team decision-making over time. We iterated on these codes until we agreed on a codebook describing the practices that teams used to support frontline members and their ideas. In the third round of analysis, two authors (OSJ and PS) used the codebook to analyze the team meeting recordings. We excluded sessions with limited team member interactions (e.g., when design principles and skills were taught, when community partners joined to explain their role in the community), incubator staff meetings, and meetings where team members worked in person and their conversations were too jumbled to parse and code. We coded 31 meetings, which amounted to 32 hr and 17 min of work for the hospital avoidance team. We also coded 34 meetings, or 48 hr and 26 min of work for the geriatrics team. Throughout coding, all three authors met regularly to discuss questions related to coding and analysis.
We then investigated the extent to which teams used these practices over the course of the innovation process. Based on the innovation literature (Perry-Smith & Mannucci, 2017), we coded each meeting as being in one of four stages of the innovation process: problem identification, idea generation, idea elaboration, and idea implementation. We coded “problem identification” for meetings where teams conducted interviews to understand the problem space. We coded “idea generation” for meetings where teams brainstormed ideas to address the problem they chose. We coded “idea elaboration” for meetings where teams selected promising ideas to develop and test, created storyboards, and updated ideas using the feedback they received. We coded “idea implementation” for meetings where teams piloted ideas, interpreted learnings, refined prototypes, and continued experimentation until the prototype became institutionalized. Meetings mostly followed a linear progression across stages, but some meetings involved activities pertaining to more than one stage, reflecting the iterative nature of innovating. In those cases, we settled on coding the dominant stage. For example, meetings where teams piloted prototypes and brainstormed ideas to refine prototypes were coded as idea implementation, as the team’s work centered on implementing rather than generating ideas.
Importantly, we made three key observations in this analytic process. First, we observed that both teams used the engagement practices that we noted above even before the actual work related to innovation (e.g., problem identification and idea generation) started. Second, we observed that the nature of the practices that we noted above evolved over the course of the innovation process. And third, we observed clusters of practices that built on and reinforced each other at different points of the innovation process. Based on these observations, we organized three cycles of engagement practices that facilitated teams’ innovation work.
We then counted the number of engagement practices used during each cycle to explore when practices were employed, following prior qualitative research that used a similar counting approach (DiBenigno & Kellogg, 2014; Satterstrom et al., 2021). As teams varied in the number of meetings, we adjusted for this number by taking the number of practices used in each cycle and dividing this number by the number of meetings from each cycle. As teams also varied in the number of people who joined meetings, we adjusted for this number by taking the average number of practices per meeting and dividing it by the average number of meeting attendees during each cycle. We followed this counting approach for each practice and graphically depicted results. For one practice, voice cultivating, which comprised five sub-practices—amplifying, building, developing, issue raising, legitimizing (more detail in Table A2 in the Online Appendix)—we took the average number of practices used per meeting per member. We also characterized the extent to which practices were used in each cycle as high, medium, or low. The median number of practices used per member per meeting from all three cycles was 0.14 and ranged from 0 to 0.60. We characterized practice use for each cycle as “high” if this number was higher than 0.20, “medium” if ranging from 0.1 to 0.19, and “low” if ranging from 0 to 0.09. More detail is provided in Figure A1 in the Online Appendix.
In parallel to the analysis of the team meetings, we also analyzed the reflections and relationships articulated by team members in interviews, which provided insight into how team members experienced this time. Moreover, as we reviewed the interview and meeting data, we noted different streams of the teams’ work and the extent of progress made in each stream (e.g., discontinued, piloted, formalized). We then met with the team leads a month after the end of data collection to confirm the status of each team’s project work.
Results
Barriers to Project Work
In line with the innovation literature, the teams that we studied faced barriers, such as limited time to work on tasks beyond core work, lack of or limited innovation work experience, and role hierarchies among team members. In terms of time, one physician from the geriatric care team articulated in an interview: When I am asked to do something outside of my allotted 90 minutes, it’s literally time that takes away from. . . I have 295 patient-related documents to review and 22 patient calls, 61 lab results awaiting my attention. This is the tension of like, you want busy clinicians involved, because we do the work, understand the problem, and have a rich sense of patients’ needs. At the same time, like what is the appropriate allotment of our time?
In terms of feeling inexperienced, one nurse said, “On-the-spot creating, like brainstorming, was new to me and was a little difficult.” In terms of hierarchies, another nurse said, “In the clinic we talk about, you know, parity among staff and not having a hierarchy. But in reality, there’s always a hierarchy, because the providers are ‘provider-ing’ and everybody else is support staff.” Similarly, we heard that team members were used to working in their silos and lacked cross-disciplinary relationships in the clinic. We found that the effects of these barriers were felt more resoundingly for managers than for staff. On top of the barriers mentioned above, frontline and middle managers also had to ensure their staff were adequately equipped for the project work in terms of time and skill, manage staffing shortages affecting not only the project work but also the health center’s clinical work, and be responsible for the project.
Three Cycles of Engagement-Facilitating Practices
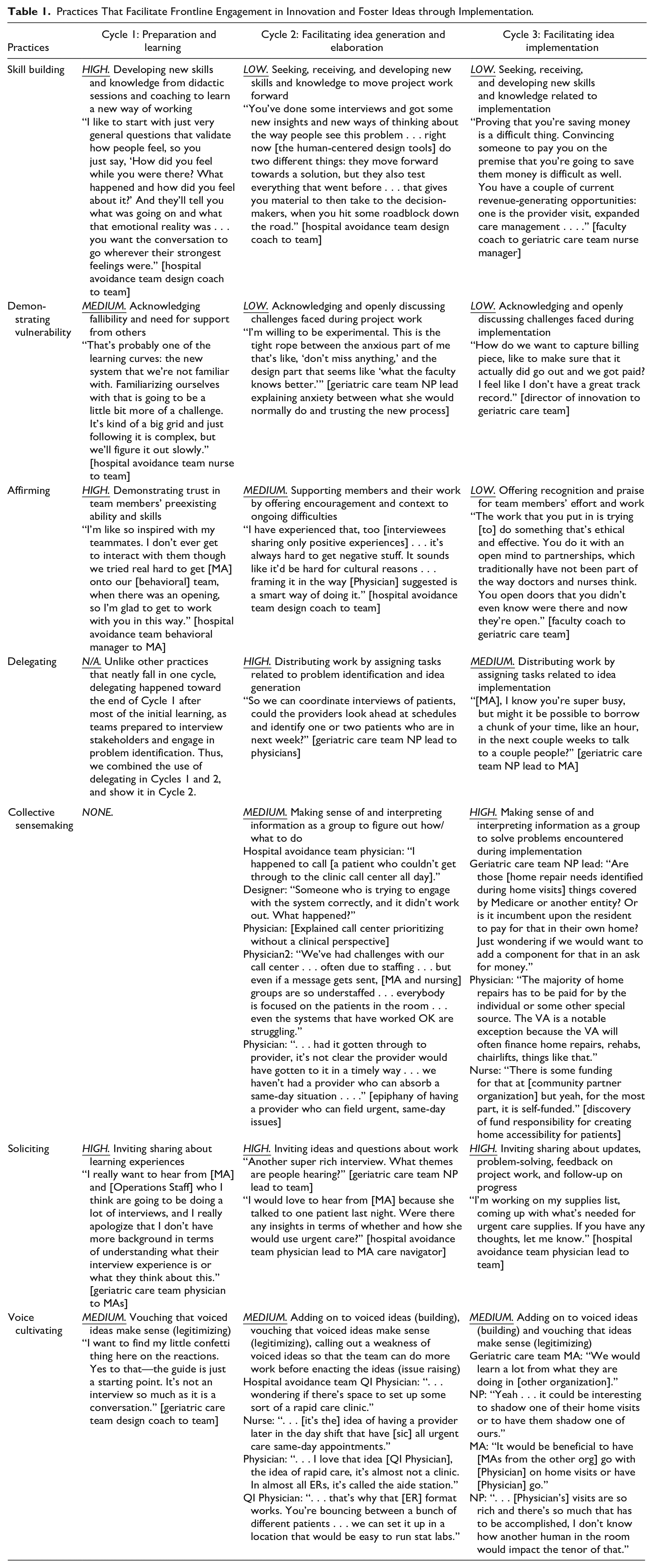
In the backdrop of these barriers, three cycles of practices facilitated frontline engagement in innovation and fostered ideas through implementation. These cycles were inductively generated as we sought to understand the behaviors and interactions that supported the different stages of the innovation process. These cycles elucidate the evolution of practices since practices may look similar but serve different purposes across the cycles. Table 1 defines the practices, describes how the practices evolved over the course of the innovation process, and provides illustrative examples of practice use.
Practices That Facilitate Frontline Engagement in Innovation and Foster Ideas through Implementation
Next, Figure 1 shows the three cycles of practices that teams used to engage frontline members and foster ideas to implementation. Only the practices that reached medium or high use are shown.
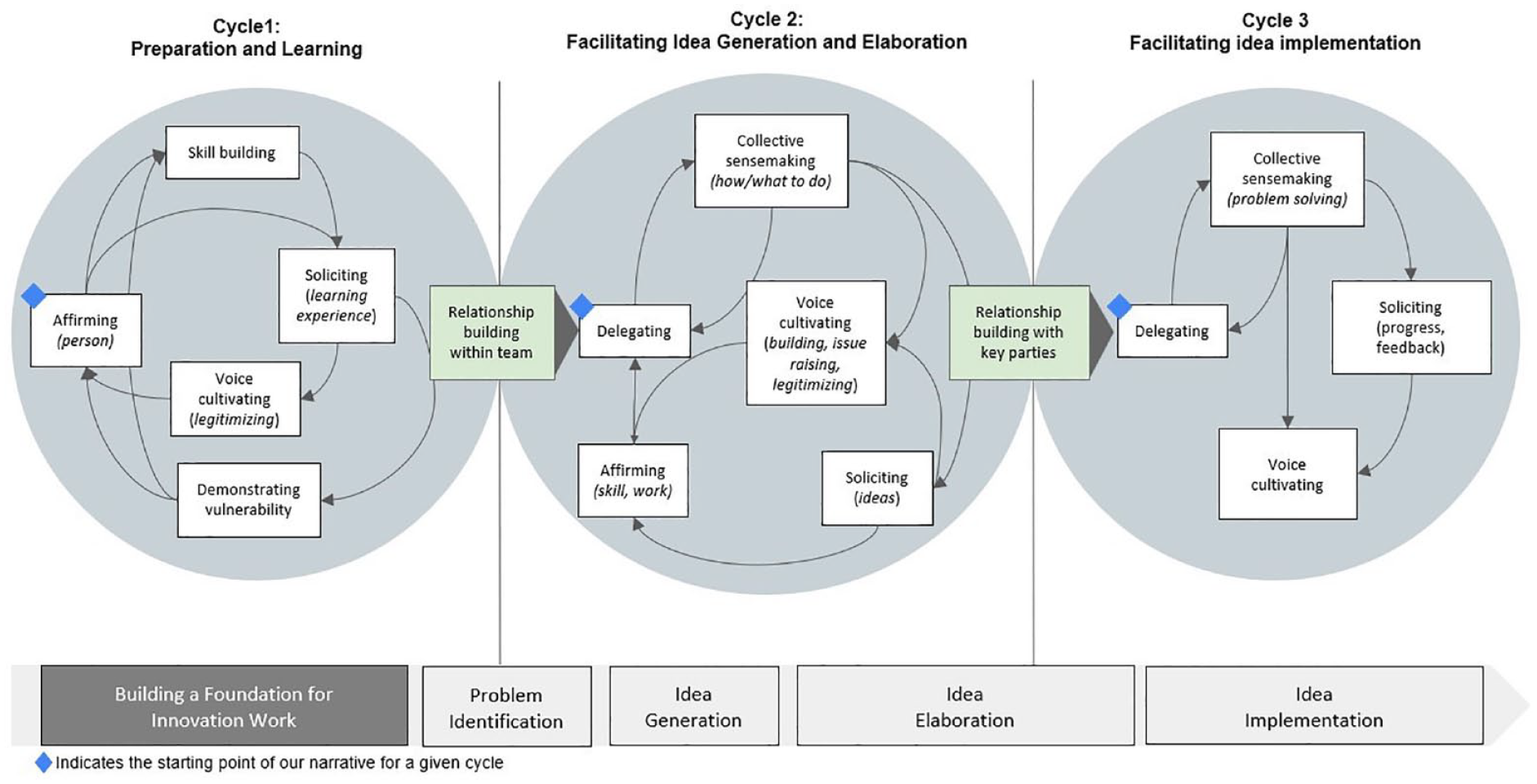
Cycles of Practices That Facilitate Frontline Engagement in Innovation and Foster Ideas Through Implementation.
A judgment that we make is about whether somebody used the emergency department appropriately or inappropriately—the system has a point of view about what is inappropriate and appropriate use. That is irrelevant right now. What’s really curious to me is what are people’s human judgment on what is and isn’t appropriate, and what are the different factors that go into that and where [patient judgment] conflicts with our ideas.
When team members struggled with the new ways of working that took them out of their day-to-day roles and hierarchies, the design coach with the geriatric care team shared, I completely appreciate that this is asking you to work in a different mode—a different mindset than what you’re used to. That’s why we talk so much about having a team dynamic where you can feel safe and feel vulnerable, because you might be doing something that doesn’t feel comfortable; it doesn’t come naturally.
As all team members gained new skills and knowledge,
When the team encountered new ways of work, team members, especially higher-power team members engaged in I think that’s what I struggle with the most, even when we practiced a few weeks ago, not being so constricted and confined to that way of thinking that we are trained to. . . I have certain ideas that are outside the clinic and what we are allowed to do and that kind of limits me.
Demonstrating vulnerability often led to or co-occurred with affirming. For example, the hospital avoidance team physician lead expressed doubts about her language skills and affirmed the skills of the team MA and nurse, by saying: I would acknowledge that I am the medical director at the clinic . . . just to put that hierarchy out there. I can imagine that we will have to break down whatever kind of dynamics are there, just because of the natural orientation of our work and the labels for our jobs. . . . In this project, I want to make sure both of you guys [team MA and nurse] can say whatever is on your mind. You are, in many ways, more experts, because of your proximity to our patient population, with respect to this project, than I am. I’m super excited to learn from you . . . you are going to take the lead on our interviews as well because of both being native speakers and better at Spanish than I am.
Acknowledging the team’s hierarchy and areas where others are more (or less) skilled encouraged team members to share their vulnerabilities as they stepped into new work.
Relationship Building Within Teams
Practices that affirmed team members’ participation and allowed members to share vulnerabilities with each other in Cycle 1 allowed members to develop a sense of camaraderie with other team members who were often outside of their immediate working groups and gain an appreciation for what they do. An MA shared, I’ve worked with providers in the past, but I was able to create more of a relationship with them [through this experience]. I’ve noticed a lot of passion from the providers, like how much they remember all of their patients. That’s a huge skill.
Another member, an operations staff, added, We’ve all been aware of everyone’s department and reached out if anything was needed for a certain project. But we never really had the opportunity to interact with each other. So [through this work] I definitely got a better understanding of my coworkers and all the amazing work that we strive to provide to our community.
A physician also similarly commented that, “For me, the most important thing was that I got to spend all this time with all these amazing people, working in a really deep way.” She added that another team member had become her “best friend at work” and that such relationships were “protective against burnout.”
Notably, the practices we observed were particularly critical for the success and well-being of middle managers. These included medical directors, quality improvement directors, and nurse managers—all of whom regularly interacted with patients—who demonstrated vulnerability, describing their work and home situations as “overwhelming,” “chaotic,” and “stressful with “limited bandwidth.” One middle manager shared with the team, It’s an intense moment to be a medical director, and a lot of people are unhappy, which I totally understand, and I also think there’s such limitations on what I can do to change anything or make it better; but [team MA] has been keeping everybody’s spirits on high.
Being open about such struggles benefited these managers in several ways. First, demonstrating vulnerability allowed other team members and coaches to provide affirmation—especially recognition of past work and reassurance when ongoing work took longer than expected—and develop a more nuanced understanding of managerial responsibilities, which were not previously visible to many other team members. Second, it encouraged team members to use their new skills to take on needed tasks, removing work from managers. For example, the NP team lead for the geriatric care team and the quality improvement director for her FQHC, said, “Shout out to [operations staff] for jumping in and being so willing to be a leader in that work; I know that was quite something. You’re a gem.”
CYCLE 2 Facilitated Idea Generation and Elaboration by Engaging Members
In this cycle, I would love to hear from [Nurse] and [MA] about how you guys are feeling about drafting the preamble, like how much we are paying the patient interviewees for the recruitment? Can we come up with a version in English and then translate it to Spanish?
Here, delegating entailed ensuring that the frontline workers had support and guidance in carrying out their task. Since different team members were taking responsibility over different aspects of the work, the teams also engaged in I feel like I’m going to miss something if [the interview] is not recorded, but everyone makes a great point that recording will alter [patients’] response. If we do the interviews in pairs, the second person can document things that the other may miss.
These practices helped further prompt team members to
Affirming during idea elaboration in Cycle 2 emphasized why input from team members was critical—for example, a physician on the hospital avoidance team told the complex care manager, I think you and your team could probably give us a lot of insight on this because the case managers do such a great job. The case manager intake is a lot of those things—disorders, thinking about activation, thinking about social barriers.
Affirming helped people feel acknowledged and reassured, especially as they struggled with new tasks. During idea generation in Cycle 2, the design coach assured the geriatric care team, “Your team is going through the learning—the process that it takes to get somewhere new. You’re getting unstuck, and it’s hard. You’re doing amazing.” Contextualizing upcoming challenges in light of past success, the faculty coach of the geriatrics care team also shared, The thinking here is exquisite, and I think you’re coming up with something that’ll move well. You’ll have to sell it to the management that it’s not going to break the bank. You have to try it out and figure out the best way to do it; this is really exciting.
Relationship Building With Key Parties
In addition to facilitating the teams’ innovation work, the Cycle 2 further facilitated relationship building within teams and with key parties internal and external to the organization. Much of the team’s work depended on the engagement and support of key parties in the clinic and in the community. For the hospital avoidance team this meant garnering the support of organizational leadership and key parties, like the call center managers and staff. It also meant improving communication, understanding, and investment between the clinic and key external partners, like the local hospitals, as well as bringing in other parties, like insurers and their analysts and public health officers and their epidemiologists. While team members had pre-existing relationships with some of these groups, they evolved during the observation period. For the geriatric care team, engaging key parties meant developing novel partnerships with community organizations. For example, piloting home visits led to unearthing patients’ home repair and upgrade needs that relate to improving their health. This then led the team to identify and invite leaders of nonprofit organizations in the community that focus on providing home repairs and accessibility modifications for older adults and apply for grants to be able to provide this service.
CYCLE 3 Facilitated Idea Implementation
In this cycle,
I go through waves of overwhelm and despair, being so enmeshed in the needs of my highest-needs patients. I think about all these really sick people, what would make a difference for them. Many are feeling lonely and experiencing existential distress.
Because of COVID, we haven’t had our patients come back into the clinic for behavioral health groups.
Yeah, so many patients are asking me for groups.
Like every patient I’ve talked to, is like, “are the groups back yet?” The groups had had a huge impact for a lot of elderly patients.
The practice of collective sensemaking enabled the team to develop a shared understanding about the context in which they were innovating and jointly make decisions about next steps and where to prioritize. In addition, during implementation,
Though they appeared at lower levels than Cycle 1, as innovation work went on, team members continued to teach each other and learn more about project-related topics, engaging in ongoing skill building. For example, during idea implementation, the geriatric care team MA offered the physician on the team instruction on using a feature of the electronic medical record. Moreover, teams sought to gain new skills, especially in areas they all had limited experience in, like financial negotiations with insurers. Similarly, affirming during Cycle 3 was in low use compared to the previous cycles and offered recognition and praise for team members’ effort and work. The faculty coach told the geriatric care team, “I want to give you guys a high five for having a multifaceted and sensitive approach to looking at the problems of the elderly and in your community.”
Use of Engagement Practices During the Innovation Process
The practices described above were not used equally throughout the cycles that enabled the team to engage in innovation work. Figure 2 illustrates the extent to which the practices were employed during the three cycles. Figure A1 in the Online Appendix shows the number of times each practice was used. One group of practices (colored in blue shades), namely affirming, skill building, and demonstrating vulnerability, appeared to be used more frequently in the beginning of the innovation process compared to later stages, suggesting their importance in equipping team members with the right skills and mindset before starting the innovation work. The use of soliciting, delegating, and voice cultivating (colored in green shades) was relatively constant over time, highlighting their salience in engaging team members throughout the innovation process. Finally, the use of collective sensemaking went up over time, peaking during implementation, as this practice helped teams analyze and learn from data generated via small-scale pilots and experimentation.
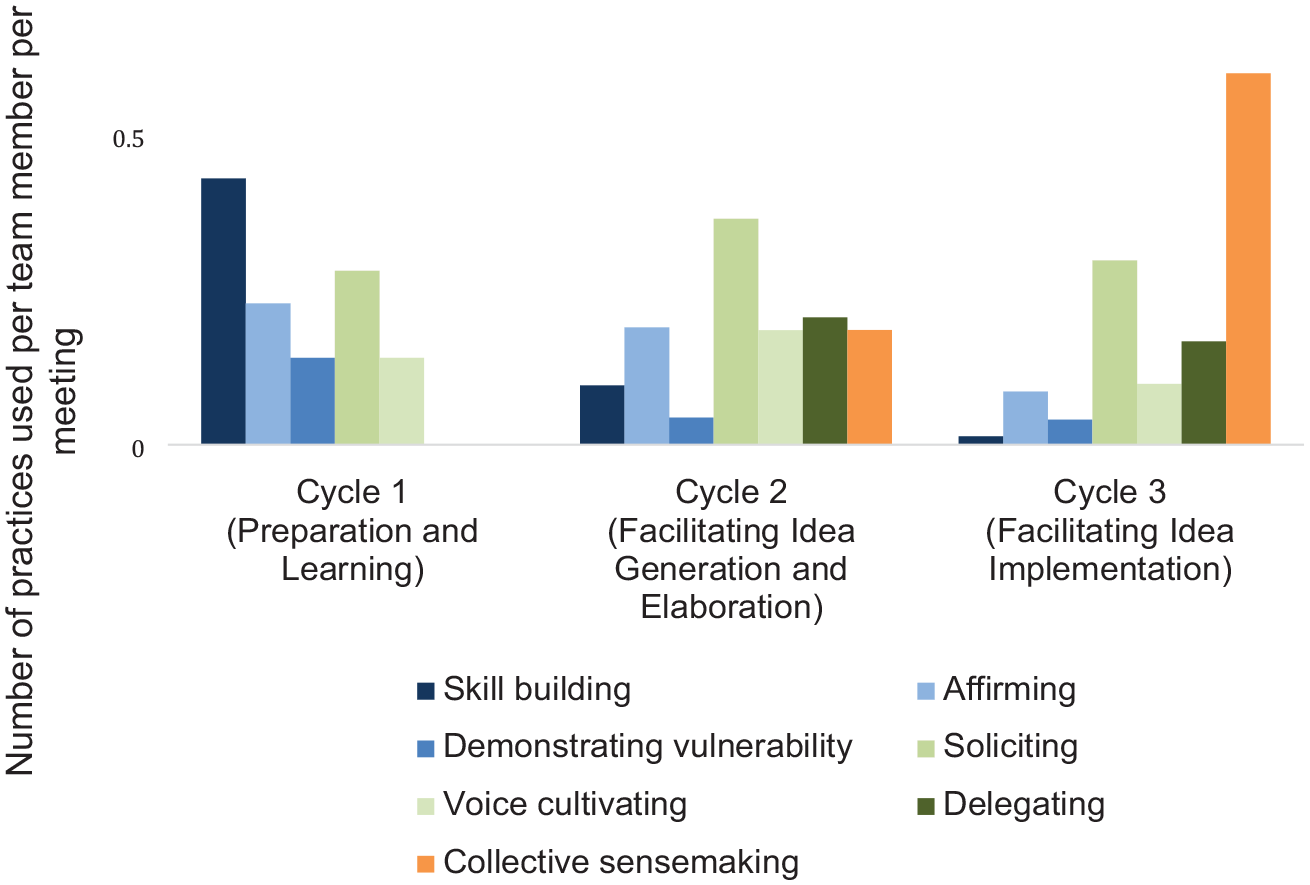
Engagement Practices Used Across Cycles.
Moreover, there were some areas of divergence in practice use between the two teams. For example, we found that the geriatric care team engaged in more delegating and collective sensemaking over the course of the innovation process than the hospital avoidance team. The differences in team size and the number of role groups represented in each team could explain this divergence; the geriatric care team had a larger team with more role groups represented than the hospital avoidance team, which meant more tasks could be delegated, and decision-making required more sensemaking among team members. We also found that the hospital avoidance team engaged in more skill building in the first two cycles compared to the geriatrics team—likely because of the differences in coaching styles of the faculty coaches and designers assigned to each team. The hospital avoidance team coach and designer took on a more hands-on, proactive role in developing members’ skills in interviewing and brainstorming than the geriatric care team coach and designer did.
Project Outcomes
The three cycles of practices allowed teams to push their ideas forward through the innovation process. The hospital avoidance team generated ideas to prevent unnecessary emergency room visits; implemented new workflows within the FQHC and between the FQHC and the two area hospitals; hired new staff; negotiated clinic space to provide in-house urgent care; increased the number of same-day appointments; and experimented with new ways to triage urgent issues through the call center. The geriatric care team brainstormed ideas to improve care for older adults, which resulted in launching home visits for high-need elderly patients and routinizing a template that facilitated structured provider-patient conversations about medications, mobility, mentation, and priorities (i.e., what matters to patients).
Discussion
This research advances our understanding of interdisciplinary innovation teams in FQHCs. The teams that we studied overcame challenges pertaining to time constraints, being new to innovation, and team-based role hierarchy to create changes in their organizations by employing practices that sustained frontline engagement in innovation and supported their ideas to implementation. Our findings provide one of the first-ever accounts of how these sustaining and supportive practices evolve over time and when team leaders, members, and coaches use them over the course of the innovation process. As FQHCs and other safety-net organizations face simultaneous pressures to innovate—to improve care quality, expand access, enhance health equity, and recruit and retain workers—growing our understanding to better enable innovation in this context is critical.
We found three series of interrelated engagement practices (“cycles”) that supported the different phases of the innovation process. Our longitudinal data provided in-depth information about the content and quantity of the practices across these three cycles. We found that, over time, some practices spanned across all cycles but changed in their focus and approach. For example, soliciting during the first cycle focused on soliciting members’ input to aid their learning experience; during the second cycle it focused on soliciting ideas for prototypes; and during the third cycle, it focused on soliciting feedback as teams made progress on pilot-testing and implementation. Similarly, building on work by Satterstrom and colleagues (2021), we show that voice cultivation was present throughout the innovation process, but it changed in its approach at different stages of the process. The team engaged in legitimizing their ideas as they learned and experimented with new ways of working. When sharing ideas about problems and improvements, the team continued legitimizing while building on each other’s ideas, issue raising to improve their ideas, and developing to make sure everyone understood the idea. As the team worked on implementation, they continued supporting voiced ideas through building and legitimizing. We found that it was critically important for team members to support (e.g., affirm) each other and to support (e.g., voice-cultivate) their ideas, since doing only one or the other could lead team members to not feel heard.
Our findings show that the quantity of practices used varied over time. These findings add to prior work on innovation and change management (e.g., Stouten et al., 2018), by suggesting that not all practices and change tactics are equal; some may be more important than others at different time points. Practices such as skill building, affirming, and demonstrating vulnerability were most salient in the earlier cycles as they helped to form norms that encouraged staff to freely contribute input and experiment with ideas, as well as helped develop new skills and endure the struggle and uncertainty of learning to use them to enact change. While the use of these practices decreased over time, they enabled the team to build relationships which were critical for supporting later practices. The use of soliciting, voice cultivating, and delegating was sustained over time, as they distributed the team’s work and were needed to maintain members’ engagement in the work and ensure ideas were implemented. The use of collective sensemaking increased over time, as this practice built on members’ willingness to contribute input and emerged from ongoing interactions rather than one-time invitations to contribute.
Though past research and practice have often focused on the behavior of managers, team leaders, and coaches in creating climates receptive to frontline engagement in voice and innovation, the practices we observed were enacted by all team members. Some practices, like affirming and demonstrating vulnerability, were actively modeled, and thus enacted more frequently, by the incubator coaches and team leaders in the first and second cycles. By the third cycle, however, other team members also engaged in these practices (e.g., a nurse affirming the medical director, an MA affirming her team members). Unfortunately, our data did not allow us to distinguish which team member used which practice; in some of the meeting recordings, all team members were present in one room and their voices overlapped, making it impossible to discern who was saying what. Future research could compare the extent to which the practices are used by team members vs. team leaders and coaches over the course of the team’s work, to see if role-modeling behaviors of leaders spread to members to build a team culture that encourages voice and innovation.
Our findings also have practical implications. The first cycle and the practices therein demonstrated the foundational, “pre-innovation” work critical for team members who were new to innovation. While many FQHCs have trained quality improvement specialists and/or departments (Friedberg et al., 2017), frontline teams are less commonly engaged in the full spectrum of innovation work. Past efforts have included collaboratives and workshops to support teams develop the skills and resources needed to succeed (Block & Manning, 2007; Lozano et al., 2022). The teams that we studied participated in an incubator, received professional coaching and training from designers specializing in human-centered design, had access to university faculty with content expertise, and used practices that fostered relationship building among team members and their coaches that facilitated their engagement in innovation work. Receiving affirmation, learning new ways of working, and cultivating professional and personal relationships with colleagues and managers, as afforded by the incubator and the engaging practices, may have the potential to reduce burnout and moral injury among frontline workers. This was especially salient among middle managers who were often tasked with participating in change work and benefited from the support of colleagues who could take work during times of peak stress, as well as reassurance from coaches during the long time frame needed to enact change. Collectively, these practices created a team culture in which team members could openly disclose challenges they were facing and support each other while building new skills.
Our study has several limitations. First, our study is qualitative and involves just two teams, possibly limiting the generalizability of our findings. However, zooming in on two teams allowed us to uniquely study the microprocesses of team interactions. With a large number of coded text fragments (~2,700), we were able to iterate between qualitative and quantitative assessment of practices to study when they occurred and how they related to each other. Second, the two teams in our study were too different for us to explore how uses of the practices were associated with implementation outcomes. For example, the hospital avoidance team had fewer people, experienced more fluctuations in team membership, and had more active coaching staff participation than the geriatric care team. It would be interesting for future research to examine how the frequency, ordering, and use of these practices relate to clinical or operational outcomes across teams. Additional research with more teams would allow more nuanced distinctions based on team characteristics, such as team size, levels of hierarchy, experience with innovation, and more. Finally, the clinics in our study chose to take part in an incubator designed to invite frontline participation. The practices described in this study may be different in clinics with more or less interest and experience in including frontline perspectives in innovation.
Conclusion
Interdisciplinary innovation teams are one way that frontline workers can lean on each other to overcome barriers to engagement and voice implementation. These teams serve as liminal spaces for learning, experimenting, and gathering evidence of each other’s perspectives, vulnerabilities, and capabilities, but they are not all successful. These collective processes, which require sustained engagement by professionals who are especially time-constrained and stressed in FQHCs and similar safety-net contexts, can succeed when cycles of practices create conditions for ideas to flourish.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587241235244 – Supplemental material for Engaging Interdisciplinary Innovation Teams in Federally Qualified Health Centers
Supplemental material, sj-docx-1-mcr-10.1177_10775587241235244 for Engaging Interdisciplinary Innovation Teams in Federally Qualified Health Centers by Olivia S. Jung, Patricia Satterstrom and Sara J. Singer in Medical Care Research and Review
Footnotes
Acknowledgements
The authors appreciate the research support of Rachael Nisenkier, Maura Danehey, Anna Quinn, and Fletcher Dementyev. The authors benefited from insightful feedback and suggestions from Aoife McDermott, Ingrid Nembhard, and OTHC and AOM conference participants. They thank the participants and staff of the incubator who generously shared their time and thoughts for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.