
Abstract
Quality improvement (QI) work is critical, particularly in federally qualified health centers (FQHCs) that treat underserved populations. In a national sample of 45 FQHCs, we examined how patients’ sociodemographic characteristics were associated with employee engagement in QI, via innovation contests that solicited ideas for improving care and offered opportunities to vote on ideas. We posited that patients’ sociodemographic characteristics influence the complexity and intensity of clinical work and thus employees’ capacity to engage in QI. Regression results indicated that the percentage of patients living in poverty was negatively associated with employee participation in idea submission and voting. Moreover, the percentage of Hispanic patients was negatively associated with participation in voting. The percentage of Black patients, however, was not associated with either outcome. FQHCs that serve a higher share of low income and/or Hispanic patients may face resource and personnel constraints that reduce employees’ capacity to contribute to QI efforts.
Keywords
Introduction
A great many opportunities exist for improving the quality of care provided by health care organizations (McGlynn et al., 2016; Schneider & Squires, 2017). One key to capturing these opportunities is engaging frontline employees in quality improvement, via behaviors such as generating and sharing ideas for improvement and participating in organizational problem-solving (Jung et al., 2022; Nembhard & Edmondson, 2006; Scott & Bruce, 1994). These behaviors have been shown to improve the quality of care and patient safety (Frankel et al., 2008; Franklin et al., 2020; Tucker & Singer, 2015).
In federally qualified health centers (FQHCs), in particular, improving the quality of care is of paramount importance, amid simultaneous pressures to expand access to care and reduce costs (Cole et al., 2021; C. Lewis et al., 2019). FQHCs are the backbone of the primary care system in the United States, especially for underserved populations. Of the nearly 29 million patients served by more than 1,400 FQHCs in 2020, 91% of patients had family incomes below 200% of the federal poverty level, 68% had incomes below 100% of the poverty level, and 62% were patients from racial and/or ethnic minority groups (Health Resources and Services Administration [HRSA], 2021). FQHCs have been shown to provide similar quality of care compared with other primary care settings (Casalino et al., 2018; Laiteerapong et al., 2014; V. A. Lewis et al., 2021), as well as reduce income- and racial/ethnic-based disparities in quality of care (Fontil et al., 2017; Lebrun et al., 2013; Shi et al., 2013). Thus, it is essential to protect and strengthen the health centers’ ability to provide high-quality care to patients of underserved populations, as these patients would often be without access to such care otherwise.
There are reasons to believe that sociodemographic characteristics of patients in a given FQHC are associated with employees’ engagement in quality improvement. First, with respect to socioeconomic status, patients living in poverty are more likely to have low literacy, reside in poor-quality housing, and have more complex health care needs—all of which can increase the overall workload and work-related stresses of primary care providers working in underserved areas (Hayashi et al., 2009). Second, with respect to the racial and ethnic composition of an FQHC patient population, health centers that serve a higher (vs. lower) percentage of Black and Hispanic patients have been shown to have less access to medical supplies and referral specialists and be more likely to have physicians who report working in chaotic work environments and low job satisfaction (Varkey et al., 2009). Furthermore, compared with non-Hispanic Whites, Black and Hispanic patients may add to the complexity of clinical work; in FQHCs, Black and Hispanic patients have been shown to have more comorbidities, more chronic pain, and lower levels of health literacy compared with non-Hispanic Whites (Dobbins et al., 2018; Varkey et al., 2009). Overall, these studies suggest that patient characteristics can affect the amount, complexity, and intensity of clinical work (Hayashi et al., 2009; Varkey et al., 2009), and consequently, employees’ ability to engage in quality improvement.
In this study, we examine the relationship of the percentage of patients living in poverty and the racial and ethnic composition of patients to employees’ engagement in quality improvement in FQHCs. We use primary data that we collected as part of a broader interventional study, merged with data from Uniform Data System (UDS). The intervention comprised innovation contests, which invited employees’ engagement in quality improvement by submitting ideas that would improve patient care and then voting on ideas that they would like to see implemented. We discuss the implications of our findings in light of ongoing efforts to implement quality improvement interventions in safety-net settings.
Quality Improvement and Innovation Contests
Improving the quality of care processes and outcomes requires effort and engagement from clinicians and staff (Wee & Lai, 2021). Following Kahn (1990) and Nembhard and Edmondson (2006), we define engagement in quality improvement as being physically, cognitively, and/or emotionally connected to the improvement work. Engagement in improvement work, such as idea generation and organizational problem-solving, can be challenging for frontline clinicians and staff because it is often not part of their formal responsibilities. Instead, it is considered discretionary and above and beyond the prescribed, remunerated job (Blasco et al., 2019; van Dyne & LePine, 1998). Participating in these types of quality improvement efforts thus necessitates intentional and extra dedication of time and effort.
Innovation contests, which expand the locus of idea generation and problem-solving, can be used to engage employees in quality improvement efforts (Malhotra et al., 2017; Terwiesch et al., 2013). Contests are a well-established mechanism for problem-solving. They broadcast a problem statement or a call for ideas and invite any and all willing and able individuals to contribute solutions (Guinan et al., 2013; Jeppesen & Lakhani, 2010). Innovation contests have been used in industries beyond health care to learn from frontline employees’ knowledge and encourage internal innovation (Adamczyk et al., 2012; Malhotra et al., 2017).
Within health care organizations, innovation contests present a new and fun vehicle to engage all frontline clinicians and staff to voice suggestions for improvement based on their idiosyncratic knowledge and experiences (Jung et al., 2020). Similar to brainstorming and reflection exercises that leaders can employ to solicit quality improvement ideas from clinicians and staff (Lee et al., 2021), contests encourage frontline employees to generate and share ideas. Unlike these exercises that engage a small, select group of employees on a quality improvement team or committee, however, innovation contests provide the structure and process that facilitate the generation and selection of ideas to broadly engage all frontline employees. Any interested employee, regardless of professional expertise, job title, or organizational tenure, can contribute input and play a proactive role in quality improvement via innovation contests.
However, prior research on organizational innovation contests and similar platforms that decentralize behaviors related to quality improvement underscores limited time and resources among frontline employees as barriers to engagement. Examples of such barriers for frontline employees include hesitation about involvement because they are rarely asked for ideas and because their time at work is primarily spent serving customers (Malhotra et al., 2020). Furthermore, employees often have the perception that core tasks leave no bandwidth for other activities (Gallus et al., 2020). In FQHCs, particularly those that see more patients who have fewer resources and greater health care needs associated with complex and intense clinical work (Bor et al., 2017; Hayashi et al., 2009; Varkey et al., 2009), frontline clinicians and staff may feel that they are unable to engage in quality improvement. When employees are too busy or overstressed, their ability to diagnose a problem and learn from experiences is compromised (Garvin et al., 2008).
Thus, we hypothesize that employees who work in FQHCs serving a high percentage of patients living in poverty and higher percentage of racial and ethnic minorities are less likely (or less able) to engage in quality improvement via idea generation and voting in innovation contests.
In addition, we also explore the association between the sociodemographic characteristics of patients and the quality of the ideas submitted by employees. It is possible that employees in FQHCs that serve patients who require intensive resources in their care are well-positioned to identify improvement opportunities and think of novel uses of the limited resources at hand (Gibbert et al., 2007; Weiss et al., 2017). At the same time, it is also possible that employees in such FQHCs perceive a low sense of control over their work, which in turn may diminish their ability and motivation to be creative (Hennessey & Amabile, 2010; Shalley et al., 2004).
New Contributions
We make the following new contributions to research and practice. First, we consider how the sociodemographic characteristics of patients in FQHCs (i.e., percentage of patients living in poverty, percentage of patients who are Black/African American, and percentage of patients who are Hispanic) are related to employees’ engagement in quality improvement. Understanding and enhancing the extent to which FQHC clinicians and staff participate in quality improvement is crucial, given the increasingly critical role of FQHCs in the U.S. health care system. Second, we explore the extent to which patient sociodemographic characteristics are related to the quality of the improvement ideas shared by employees. Specifically, we aim to find out whether patients’ sociodemographic characteristics relate to employees’ ability to generate creative, feasible, and impactful ideas. Third, we leverage data from a novel intervention that the lead author conducted with FQHCs across the United States and merge these data with variables from the UDS to test the study hypotheses. In building our hypotheses, we bridge the literatures on innovation contests and quality improvement. We do so by conceptualizing the contest participation (i.e., idea generation and voting) as engagement in quality improvement. In this way, we suggest that innovation contests can be used as a relatively simple and inexpensive quality improvement intervention (compared with implementing patient-centered medical home [PCMH] or enhancing health information technology, for example) that invites all interested clinicians and staff to contribute ideas to better patient care and work processes.
Method
This research is part of a multi-method study that examined the impact of innovation contests on frontline employees’ voice and innovative behaviors in FQHCs. In 2018, the lead author invited 1,367 FQHCs funded by the Health Resources and Services Administration (HRSA) Health Center Program to participate in this study. The directors of 203 FQHCs attended an informational webinar, during which the first author discussed the experiences of various health care organizations with innovation contests and what would be provided to participating FQHCs (e.g., promotional materials, contest infrastructure, prizes). Afterward, 54 directors signed the participation agreement. This sample size is comparable or higher than other interventional studies in the health care setting (e.g., Curry et al., 2018; Tucker & Singer, 2015). The participating FQHCs were evenly distributed among the four geographic regions in the United States (the Northeast, the Midwest, the South, and the West, Table 1).
Sample Characteristics and Variable Descriptive Statistics.
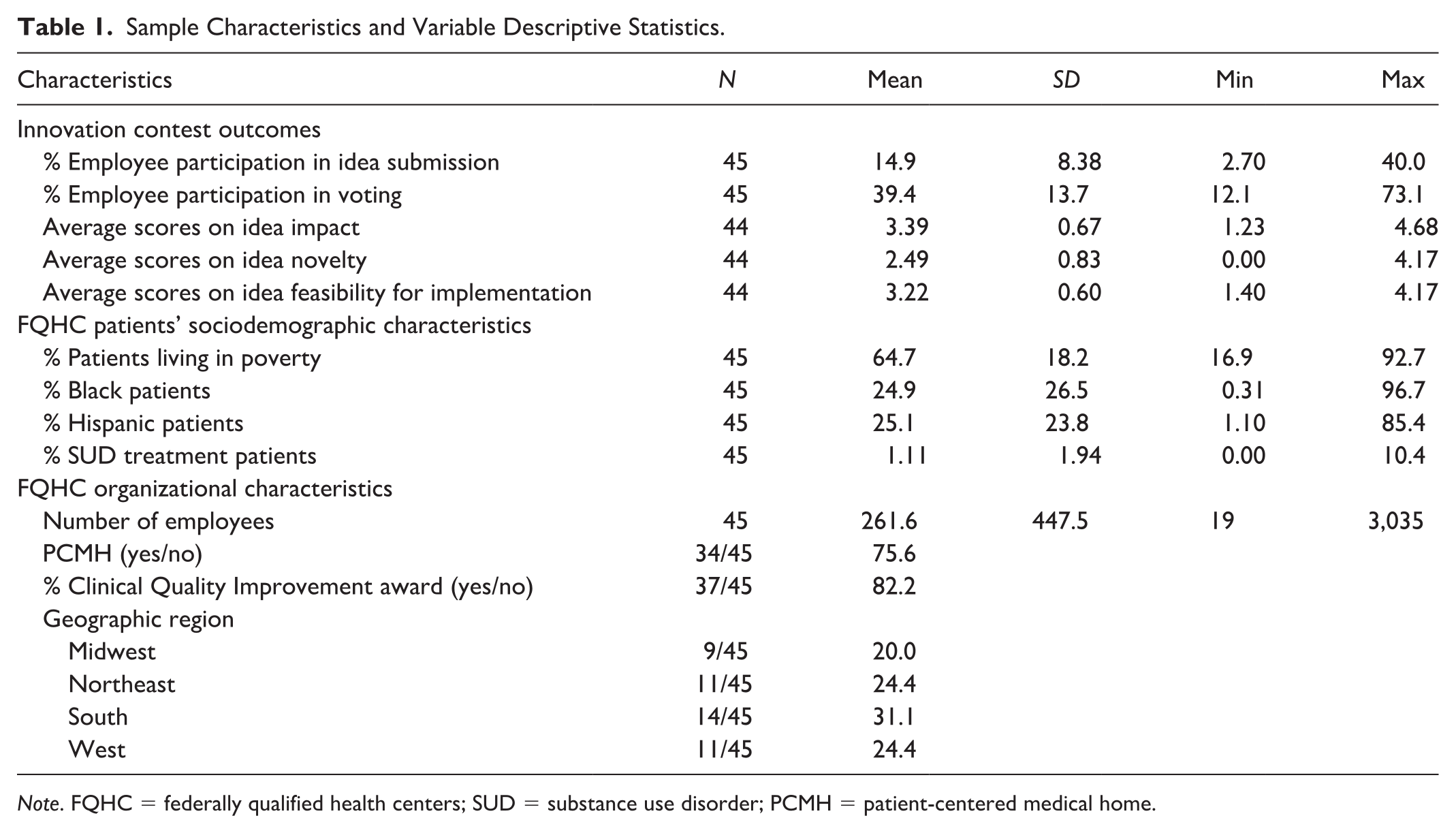
Note. FQHC = federally qualified health centers; SUD = substance use disorder; PCMH = patient-centered medical home.
Using data from this broader study, we examined the association between sociodemographic characteristics of patients served in these FQHCs and employee participation in idea submission and voting as well as senior managers’ evaluation of submitted ideas. Of the 54 participating FQHCs, nine were dropped because they had missing data on a key control variable (percentage of patients who receive substance use disorder [SUD] treatment); this yielded an analytic sample of 45 FQHCs for our study. Compared with the FQHCs that did not respond participation in the study, the FQHCs in the analytic sample had similar characteristics on all study variables described below (see Online Appendix, Table A1).
Innovation Contests
The first author coordinated with a senior manager (e.g., the chief executive officer, director of human resources) from each FQHC to implement the organizational innovation contests. 1 The contests broadly sought ideas to improve patient care. To standardize the implementation of contests in all participating FQHCs, the lead author asked senior managers to use the materials and language that she created to promote and administer the innovation contest, at the time points that she specified.
All employees, regardless of role and tenure in the organization, were invited to participate. The contests began with a 3-week-long ideation phase. Ideation entailed describing a work issue and proposing a solution, with each response limited to 250 characters. Next came a 3-week-long voting phase. Employees were asked to indicate the extent to which they would like to see each idea implemented, on the scale of 1 (do not want to see it implemented) to 5 (want to see it implemented). The average of the ratings determined the winners. One winner and one runner-up per contest won $100 and $35 gift cards, respectively.
Submitted ideas addressed a wide range of issues, including new service opportunities (e.g., conducting home visits for patients who have had multiple emergency room visits, offering acupuncture services, providing customized care for patients with HIV), tactics to address social determinants of health (e.g., transportation, financial support, case management support), community development and outreach (e.g., partnering with community organizations, involvement of community members as volunteers), and workflow improvement. One idea on community outreach proposed to “create a special team [that included a] provider, nurse, community health worker, and medical assistant to take the medical bus once a month to severely underserved areas (e.g., subsidized housing towers).” Another idea on employee morale called for a “forum for employees to thank others for their good work, ideas, or management. It can be a website or bulletin board that people can post notes on.”
Data Sources and Measures
Engagement in quality improvement was measured using two variables, consistent with prior research on innovation contest participation (Jung et al., 2020): participation in (a) idea submission and (b) voting. We computed the percentage of employees participating in each phase by dividing the number that submitted ideas and voted on ideas by the total number of employees for each FQHC, respectively.
Idea quality was measured using senior managers’ evaluation of the submitted ideas in terms of impact, novelty, and feasibility, following previous research (Girotra et al., 2010; Poetz & Schreier, 2012). Senior managers from 44 FQHCs in our analytic sample evaluated all the ideas from their own organization in these dimensions on the scale of 1 (low) to 5 (high), without knowing who submitted which idea or how the ideas fared in voting. We computed the average score of all ideas on each dimension (impact, novelty, and feasibility) for a given FQHC.
Patients’ sociodemographic characteristics were drawn from HRSA’s 2018 UDS. Each year, FQHCs report standardized information about their performance and operation, including patient demographics. From this dataset, we obtained information about the percentage of patients who were living at or below 100% of the federal poverty level, who were identified as Black/African American, and who were identified as Hispanic/Latino.
Control variables included the percentage of patients receiving services for SUD gathered from UDS, as this variable has been shown to be correlated with poverty and race/ethnicity (Jones et al., 2020; Varkey et al., 2009). We also included measures of the total number of employees, whether the FQHC received a Quality Improvement Award from HRSA in fiscal year 2017 (yes/no), and whether the FQHC is a PCMH (i.e., received an additional quality improvement award from HRSA for achieving PCMH recognition; yes/no). We controlled for these variables, as they may be correlated with patient demographics and they have been shown to be associated with FQHC employee burnout and care delivery processes (Shi et al., 2017; Timbie et al., 2017).
Analysis
We summarized the means, standard deviations, and minimum and maximum values for the innovation contest outcomes (employee participation, idea quality), patient characteristics, and organizational characteristics.
To test our hypotheses that explore the relationship between patients’ sociodemographic characteristics and employee participation in quality improvement, we used linear regression models with robust standard errors. The unit of analysis was the health center. Our first two dependent variables were the percentages of employees that participated in (a) idea submission and (b) voting on the ideas. To examine these associations, we estimated four regression models for each dependent variable. In Model 1, we regressed the poverty measure on each outcome variable. In Model 2, we regressed the two variables that assessed racial/ethnic composition (i.e., percent of patients who were Black, and percent of patients who were Hispanic) on each dependent variable. In Model 3, we regressed the control variables on each dependent variable. Finally, in Model 4, we included all variables. The findings from all of these regressions are presented in Tables 2 and 3.
Linear Regression Models Associating Employee Participation in Idea Submission and Patient Population Characteristics.
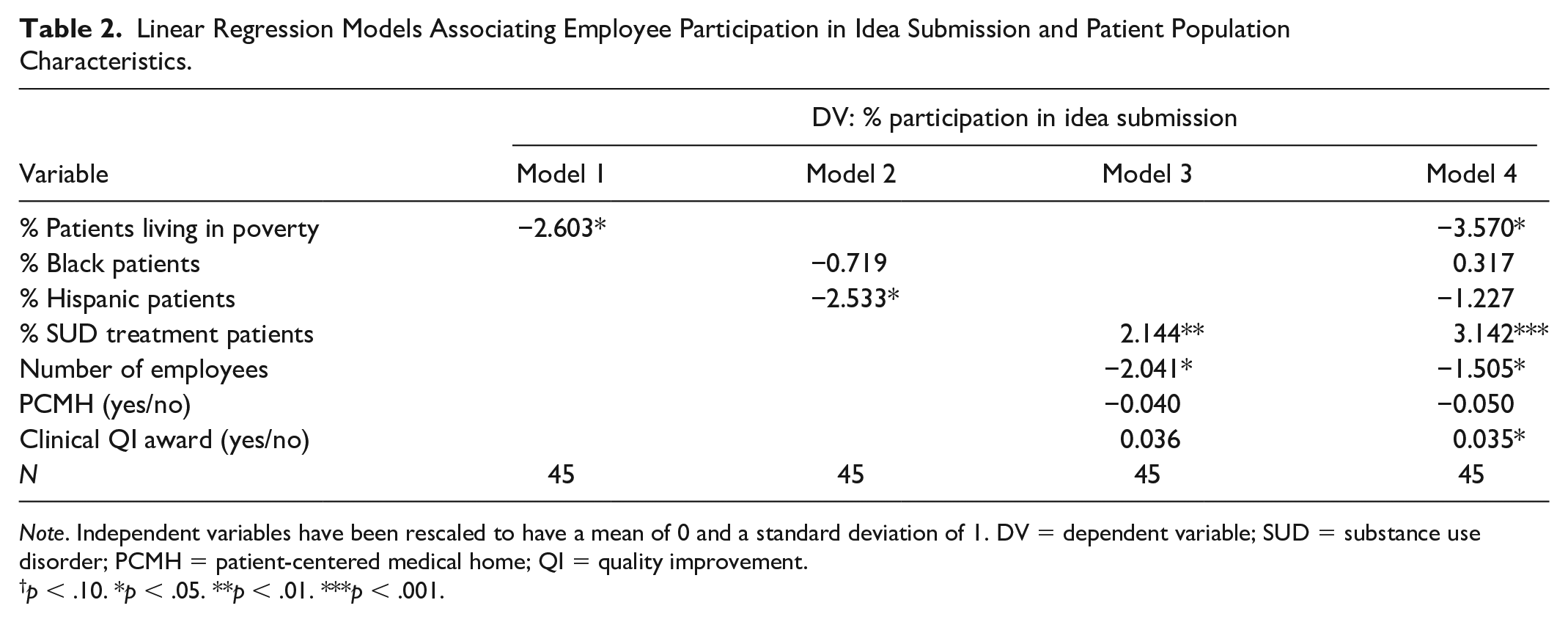
Note. Independent variables have been rescaled to have a mean of 0 and a standard deviation of 1. DV = dependent variable; SUD = substance use disorder; PCMH = patient-centered medical home; QI = quality improvement.
p < .10. *p < .05. **p < .01. ***p < .001.
Linear Regression Models Associating Employee Participation in Voting and Patient Population Characteristics.
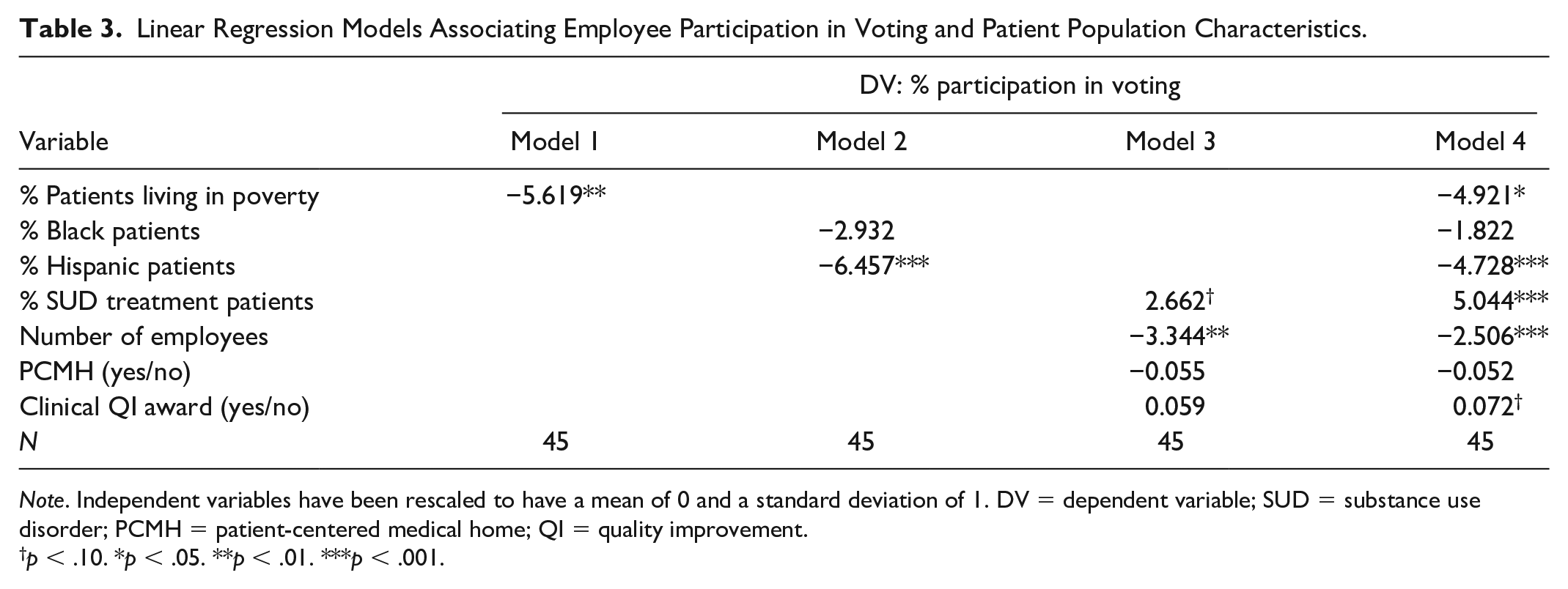
Note. Independent variables have been rescaled to have a mean of 0 and a standard deviation of 1. DV = dependent variable; SUD = substance use disorder; PCMH = patient-centered medical home; QI = quality improvement.
p < .10. *p < .05. **p < .01. ***p < .001.
To explore the relationship between the three measures of idea quality (impact, novelty, and feasibility) and patients’ sociodemographic characteristics, we also estimated the regressions in the same stepwise approach described above. For these three dependent variables, we present the fully specified models in Table 4 and the results from the other specifications in Table A2 in the Online Appendix.
Linear Regression Models Associating Idea Quality and Patient Population Characteristics.
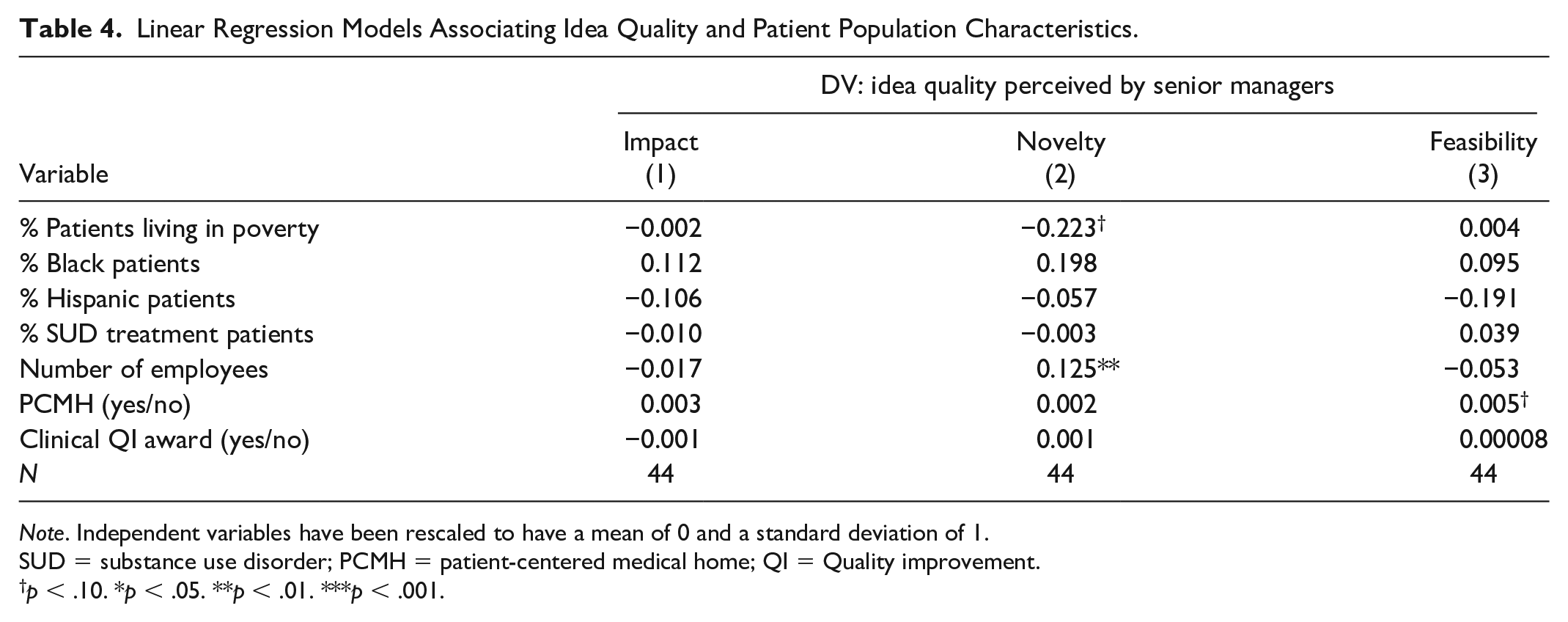
Note. Independent variables have been rescaled to have a mean of 0 and a standard deviation of 1.
SUD = substance use disorder; PCMH = patient-centered medical home; QI = Quality improvement.
p < .10. *p < .05. **p < .01. ***p < .001.
For ease of interpretation, we standardized the independent variables so that a one-unit increase corresponded to a one standard deviation increase in the measure above the mean value. A p value of <.05 was considered statistically significant. Stata 17 (StataCorp LLC, College Station, TX) was used for all analyses.
Results
Table 1 shows the descriptive statistics of contest outcomes and characteristics of the participating FQHCs and their patient populations in our analytic sample. On average, 15% of the employees submitted ideas, with values ranging from 2.7% to 40%. Various role groups participated; of those who participated in idea submission, 40% were non-clinical support staff (e.g., receptionists, referral coordinators, billing personnel), 22% were clinical support staff (e.g., medical assistants, dental assistants), 13% were health professionals (e.g., dietitians, behavioral health therapists), 8% were advanced practice nurses, 8% were physicians and dentists, and 5% were nurses. Thirty-nine percent of employees, on average, participated in voting, and this value ranged from 12% to 73%. In terms of idea quality, on the scale of 1 to 5, on average ideas received a rating of 3.39 in terms of impact (ranging from 1.23 to 4.68), 2.49 in terms of novelty (ranging from 0 to 4.17), and 3.22 in terms of feasibility (ranging from 1.40 to 4.17).
When examining patients’ sociodemographic characteristics at the center level, an average of 65% of the patients served by the FQHCs in this study sample were reported to be living at or below 100% of the Federal Poverty Guidelines, with values ranging from 17% to 93%. On average, nearly one fourth (24.9%) of the patients were Black, with values ranging from 0.31% to 97%. An average of one fourth of patients served by these FQHCs (25%) were Hispanic, with values ranging from 1.1% to 85%.
There was also variation among the control variables. Of the 45 FQHCs in our analytic sample, 34 (76%) achieved the PCMH certification. At the time of the study, these FQHCs employed a mean number of 262 individuals, with a wide range from 19 to 3,035. On average, 1.1% of the patients served by these FQHCs received SUD treatment; this percentage ranged from 0% to 10%. Of note, 19 (42%) of these FQHCs indicated that none of their patients received any SUD-related services. Table A3 in the Online Appendix shows the pairwise correlations among examined variables.
Tables 2 and 3 show the association between patients’ sociodemographic characteristics and employee participation in idea submission and voting, respectively. Hypothesis 1 predicted that the percentage of patients living in poverty would be negatively associated with employee participation. We found support for this hypothesis. The percentage of patients living in poverty was negatively associated with idea submission in the bivariate (p = .022, Model 1, Table 2) and fully adjusted models (p = .021, Model 4, Table 2). A one standard deviation increase (above the mean value) in the percentage of patients living in poverty was associated with a 3.6 percentage point decrease in percent of employees who submitted an idea. When examining employee participation in voting, results were mostly similar, with larger and stronger associations. In the fully specified model (Model 4, Table 3), the percentage of patients living in poverty was negatively associated with voting (β = −4.9 percentage points, p = .032).
Hypothesis 2 predicted that the percentage of Black patients would be negatively associated with employee participation in the contest. We did not find support for this hypothesis. The associations between the percentage of Black patients and idea submission and voting were both in the expected direction (except in Model 4, Table 2), but did not reach statistical significance in any of these models.
Hypothesis 3 predicted that the percentage of Hispanic patients would be negatively associated with employee participation. We found marginal support for Hypothesis 3a (idea submission) and stronger support for Hypothesis 3b (voting). In Model 2, Table 2, which did not include the control variables, the association between the percentage of Hispanic patients and idea submission was statistically significant (β = −2.5 percentage points, p = .031) but in the full model (Model 4), the association was no longer significant (β = −1.2 percentage points, p = .193). When examining employee participation in voting, associations were larger and reached statistical significance (β = −4.7 percentage points, p = .001, Model 4, Table 3).
Noteworthy among the control variables, the percentage of patients receiving any SUD treatment was positively associated with idea submission (p = .002, Model 3, Table 2), and the coefficient became larger and more significant in the full model. According to Model 4 in Table 2, a one standard deviation increase (above the mean value) of the percentage of patients receiving SUD treatments was associated with a 3.1 percentage point increase in idea submission (p = .001). The association of the percentage of patients receiving any SUD treatment and participation in voting was also positive and significant (β = 5.0 percentage points, p < .001).
Table 4 shows the results of linear regression models associated with patients’ sociodemographic characteristics and idea quality. Patient characteristics were not associated with idea quality, in terms of impact, novelty, and feasibility, as perceived by senior managers. The number of employees, however, was positively associated with scores of the novelty of the ideas submitted (β = 0.12 percentage points, p = .007, Model 2, Table 4).
Discussion
Using a novel dataset from implementing innovation contests in a national sample of FQHCs, our study provides the first known assessment of the association between patients’ sociodemographic characteristics and employee participation in quality improvement in FQHCs. FQHCs are the foundation of the primary care safety-net for underserved populations in the United States. Importantly, we find that employees in FQHCs that serve a higher percentage of patients living in poverty and a higher percentage of patients that identify as Hispanic were less likely to participate in an organizational innovation contest, the quality improvement intervention that we examined. The effect sizes were substantial; a one standard deviation increase in the percentage of patients living in poverty (above the mean) was associated with a 3.6% decrease in the percentage of employee participation in idea submission, equivalent to about half of the dependent variable’s standard deviation. Similarly, we found that the percentage of employees that voted on ideas was significantly lower in FQHCs with a higher percentage of Hispanic patients. Considered together, our findings indicate that employees in FQHCs with a higher share of patients living in poverty and/or Hispanic patients were less likely to engage in quality improvement, even though these FQHCs would have especially benefited from this kind of a quality improvement initiative (Shin et al., 2017).
Our findings on the negative association between percentage of patients living in poverty and both measures of employee participation in innovation contests add empirical evidence to a growing body of literature on quality improvement efforts in FQHCs. Engagement in idea generation and organizational problem-solving, which are behaviors espoused by innovation contests, are related to employees’ awareness, buy-in, and participation in implementation of larger quality improvement strategies such as the PCMHs (Timbie et al., 2017), advanced health information technology (Frimpong et al., 2013), and alternative payment models (Okeke et al., 2021). Thus, the negative association between certain sociodemographic characteristics of patients and employee participation in innovation contests may have implications for employees’ engagement with more complex initiatives. For example, implementing a PCMH model, which entails a whole practice transformation and substantial engagement of employees (Friedberg et al., 2017), may be especially challenging in FQHCs that serve a high share of underserved patients. Future research is needed to examine the impact of patients’ sociodemographic characteristics on quality improvement initiatives that are more elaborate than innovation contests. It may yield important insights for policy initiatives that aim to incentivize and support quality improvement efforts in safety-net organizations.
Interestingly, while patients’ socioeconomic status was associated with employee participation in both aspects of innovation contests (idea submission and voting), the racial and ethnic composition of the patient population was not. Specifically, we did not detect a statistical significance in the association between the percentage of Black patients and employee participation assessed with either outcome. We did find, however, that the percentage of Hispanic patients was negatively associated with employee participation in voting. It is possible that the complexity and intensity of the clinical workload may be differentially affected by the specific racial and ethnic composition of patients, and consequently, the employees’ bandwidth to engage in quality improvement. For example, compared with Black patients, Hispanic patients may face greater language barriers and require more support related to health literacy and translation/interpreter services (de Alba et al., 2016).
When examining other covariates in our model, we also found that employees were more likely to participate in idea submission as well as voting in FQHCs that serve a higher percentage of patients receiving services for SUD. The effect sizes were considerably large and significant, even though the model also controlled for other organizational-level characteristics. One explanation for this positive association may relate to resource availability. Studies have shown, for example, that FQHCs that received federal funding and supplementary grants related to SUD service expansion were more likely to offer addiction counseling, provide medication-assisted therapies, and employ more psychiatrists and addiction counselors (Jones et al., 2020; Pourat et al., 2020; Saloner et al., 2020). Thus, it is possible that FQHCs that treated a higher share of patients with SUD were better resourced in terms of funding and personnel, and consequently, better able to invest and encourage workers to engage in quality improvement. Relatedly, it is also possible that FQHCs that provide SUD treatments had more experience with innovation, and that in these FQHCs, employees were more likely to believe that their center is open and willing to experiment with and implement new ideas.
Across all independent variables related to patient sociodemographic characteristics, we observed that their relationship to voting (vs. idea submission) entailed larger coefficients and stronger statistical significance. We believe that the barrier to participating in voting (vs. idea submission) may be smaller, because voting takes less time and effort than generating, writing up, and submitting ideas. Indeed, we noted a higher level of employee engagement in voting than in idea submission in this study, as well as in a prior study conducted among hospital workers (Jung et al., 2022). Thus, it is possible that the relationship of employee participation in voting and patient sociodemographic characteristics was more pronounced because it is easier to participate in voting than in idea submission, regardless of the patient mix in a given FQHC. It is also possible that there is a conceptual difference in how workers perceive and engage with these two activities. Future study should explore these differences to better understand ways to encourage workers to engage in quality improvement work.
As for the quality of the ideas submitted, we did not detect significant associations between patients’ sociodemographic characteristics and perceived impact, novelty, and feasibility of the ideas. We did, however, find that ideas that emerged in larger FQHCs (with more employees) were more likely to be rated as novel. Prior research on quality of care in FQHCs has shown that the number of full-time physicians and other service providers is associated with positive quality outcomes (Shi et al., 2012, 2017). Moreover, workers in larger practices are less likely to experience burnout than those who work in small practices (Edwards et al., 2021). Thus, it may be the case that workers in FQHCs that are well-staffed, compared with those that are not, are able to practice more creativity in their idea generation for quality improvement, because they have had more exposure to quality improvement efforts and have more bandwidth to think of novel improvement opportunities (Woodman et al., 1993). This finding further highlights the importance of personnel resources in FQHCs (Wakefield, 2021).
These findings should be considered in light of the following limitations. Our sample size is small and there may be concerns that this sample of FQHCs, where the senior managers elected to conduct innovation contests with their employee population, does not represent a typical FQHC. However, we show that FQHCs in our analytic sample are not different from non-participating ones in terms of the patients’ sociodemographic characteristics that we examined in this study as well as performance in quality metrics (results are reported in Table A1 in the Online Appendix). In addition, while we conducted our analysis at the organizational level (due to the lack of site-level identifiers in the UDS data), there may be important variations in patient characteristics and worker engagement in quality improvement at the site level. It may be helpful for future research to examine the relationship of worker engagement and patient characteristics and other contextual factors that affect quality improvement work at the site level. Finally, while we did not have data on employee morale, burnout, and satisfaction, examining the mediating role of these variables could have enriched our analyses. Future research should investigate the extent to which patient characteristics influence job demands, reflected in measures like morale and burnout, and how this affects employees’ engagement in quality improvement.
Conclusion
There is a national emphasis among U.S. policymakers, practitioners, and scholars to transform practice and improve the quality of care in safety-net settings and beyond. Many health care delivery organizations face resource and personnel constraints in efforts to improve quality of care. Our study shows that such constraints may be more present in organizations that serve a higher share of low-income and/or Hispanic patients. Our findings suggest that considering the sociodemographic characteristics of the patient populations may be critical when implementing quality improvement initiatives, as they may provide information about the ability and bandwidth of the workers to participate. Further examinations of the impact of patients’ sociodemographic characteristics on quality improvement initiatives that entail time- and energy-intensive implementation would be informative to develop policy that aims to support quality improvement efforts. Moreover, as increasing job demands and the imperative to improve quality are common concerns facing many health care organizations beyond FQHCs, replicating this study in other settings (e.g., primary care clinics, urgent care clinics) would help expand our understanding about the relationship between patient characteristics, clinical workload, employee burnout and morale, and engagement in quality improvement.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587221118157 – Supplemental material for Employee Engagement in Quality Improvement and Patient Sociodemographic Characteristics in Federally Qualified Health Centers
Supplemental material, sj-docx-1-mcr-10.1177_10775587221118157 for Employee Engagement in Quality Improvement and Patient Sociodemographic Characteristics in Federally Qualified Health Centers by Olivia S. Jung and Janet R. Cummings in Medical Care Research and Review
Footnotes
Acknowledgements
We thank the federally qualified health centers—all managers and frontline clinicians and staff—that participated in the study.
Correction (July 2023):
The ‘Geographic region’ section in Table 1 has been updated accordance with the changes made in the text on page number 48. Additionally, appendix ‘Table A1. Participating versus non-participating FQHCs’ has also been revised.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
We received financial support from Schmidt Futures for this research.
Ethical Approval
All study procedures were approved by the Institutional Review Board at Harvard University.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.