
Abstract
Background
Prolonged immobility associated with digital screen exposure-termed “e-thrombosis"-is an emerging concern for Generation Z and Alpha. While thromboprophylaxis is standard for surgical or travel-related stasis, screen-related inactivity in adolescents remains under-recognized. This study aimed to evaluate the impact of digital device–related inactivity on the development of thrombosis in adolescents.
Methods
This retrospective observational study included children followed for thrombosis at the Department of Pediatric Hematology and Oncology, Kırıkkale University Faculty of Medicine, between 2010 and 2024. Demographic data of adolescent patients were obtained from the hospital data system. Adolescents with thrombosis who reported ≥4 h of daily screen exposure included. Face-to-face interviews were conducted with patients and their parents to verify screen exposure duration, and digital usage records were reviewed in detail.
Results
Out of 71 pediatric thrombosis cases, 11 adolescents met the inclusion criteria for prolonged screen exposure. The study group spent an average of 6 ± 1 h daily on digital devices (gaming, education, or social media), with uninterrupted immobility lasting 2.7 ± 0.9 h. Clinical diagnosis included lower extremity deep vein thrombosis (n = 8), pulmonary embolism (n = 2), and subclavian vein thrombosis (n = 1). Genetic thrombophilia mutations were identified in 9 out of 11 patients.
Conclusion
Prolonged immobility associated with the widespread use of digital devices constitutes a significant, yet frequently underrecognized, risk factor for thrombosis, particularly in adolescents with a genetic predisposition. As increasing screen exposure leads to various health complications in the youth, enhancing clinical awareness and integrating prophylactic strategies into daily practice is of paramount importance.
Introduction
With today's technological developments, communication, education, entertainment and working methods have changed, and we have almost completely transitioned to a virtual life. It has been reported that the number of computers and tablets reached approximately 400 million in the 2020s. 1 It is estimated that 80% of users, whose numbers are increasing and whose ages are decreasing, will spend a large part of their lives with these devices, meaning they will remain inactive. 1 The new lifestyle, characterized by the intensive use of smartphones, tablets and computers, brings with it a sedentary lifestyle and potentially serious health problems. Particularly during adolescence, the amount of time spent sitting and being inactive is increasing in relation to increased exposure to digital screens.2-5 One significant problem associated with a sedentary lifestyle is an increased risk of thrombosis. Beasley and colleagues drew attention to this issue in 2003 with a 32-year-old male patient who developed pulmonary embolism (PE) due to prolonged sitting at a computer and proposed the term ‘e-thrombosis’ for thrombosis caused by inactivity associated with digital device use in the twenty-first century. 6
The intensive use of digital devices by Generation Z and Generation Alpha has contributed to an increase in sedentary lifestyles. Thromboprophylaxis is often recommended in situations involving prolonged immobility, such as after surgery or during long journeys. However, the immobility associated with prolonged exposure to digital screens is often overlooked. In parallel with technological developments, we aimed to highlight the role that prolonged screen exposure and sedentary lifestyles, particularly among adolescents, may play in the development of thrombosis and to evaluate the effect of e-thrombosis, a new risk factor, on thrombosis susceptibility in the adolescent age group.
Methods
In this retrospective observational study, the files of patients diagnosed with thrombosis and followed up with clinical, laboratory, and imaging examinations at the Department of Pediatric Hematology and Oncology, Faculty of Medicine, Kırıkkale University (Türkiye), between 2010 and 2024 were retrieved from the hospital data system. Demographic data and clinical risk factors were recorded based on the patient's status at the time of the event. Patients who were adolescents (10-19 years old) at the time of their thrombosis diagnosis were contacted by telephone. They were questioned about the acquired causes of thrombosis and their exposure to digital screens. Patients meeting the exclusion criteria (in Table 1) were excluded from the study. The questionnaire in Table 2 was administered to the remaining cases. Adolescents with at least 4 h of daily digital screen exposure formed the study group. The flow chart for forming the study group is presented in Figure 1. Detailed face-to-face interviews were conducted with the cases in the study group and their parent. For those under 18 years of age, both the patient and the parent were interviewed. For those who were 18–19 years old at the time of diagnosis and are now adults: The patient's own statement was primarily relied upon, but support was obtained from their families to verify past household routines. Digital screen exposure times and uninterrupted screen time were recorded. The time spent in front of the screen was determined by scanning digital records from portable devices (phones, tablets, laptops). Screen time data were obtained from applications such as Digital Balance, Digital Health, Screen Time-Parent Control, and the phone's own system settings-screen time indicator. Data covering a one-year period were retrieved from these records. Interviews with patients and parents revealed that current lifestyle habits are similar to those at the time of thrombosis diagnosis. Furthermore, for students who were sedentary due to distance learning, official educational curriculum schedules and online lesson hours were cross-referenced to verify daily exposure.

Flowchart of the study design. Abbreviations: VTE, venous thromboembolism.
Exclusion Criteria.
Questionnaire on Immobility Time in Relation to Daily Screen Exposure.

Genetic thrombosis panel records analyzed using Real-Time PCR were obtained from the files (Genetic screening was performed in patients with a positive family history).
Descriptive statistics were performed using SPSS version 27 program. Categorical data are presented as percentages. Continuous data following a normal distribution are expressed as mean ± standard deviation (SD).
Ethics committee approval has been obtained (Decision no: 2024.12.05).
Results
In this study, we retrospectively identified 71 patients with clinically, laboratory, and radiologically confirmed thrombosis. Forty-one of the 71 patients with thrombosis were adolescents (aged 10-19 years). The files of these 41 patients, their demographic characteristics, and their hereditary and acquired risk factors were examined using the hospital record system. We were unable to contact six patients, and these patients were excluded from the study. Thirty-five patients’ parents were contacted by telephone (in our hospital's registration system, contact information is primarily recorded for parents/legal guardians rather than the pediatric or adolescent patients themselves), and their family history of thrombosis and environmental thrombosis risk factors were investigated. Twenty patients were excluded from the study according to the exclusion criteria (Table 1). The questionnaire presented in Table 2 was administered to 15 patients. Screen exposure-related sedentary periods at the time of thrombosis diagnosis were obtained through a combination of digital records, including verbal accounts (patient and parent), educational programmes, social media activity (Instagram time), parental control app usage, screen time logs, and digital health app logs. Eleven patients with at least 4 h of screen exposure per day were included in the study. Of the 11 adolescents included in the study, 45.5% were female (n = 5) and 54.5% were male (n = 6), with a mean age of 15 ± 2. Face-to-face interviews were conducted with these 11 patients and their families to verify the information, and screen time data was recorded from portable devices (phones, tablets, laptops). It was found that patients spent an average of 6 ± 1 h in front of computer, tablet, or phone screens for gaming, work, or education and remained inactive for an average of 2.7 ± 0.9 h.
Additionally, sitting habits such as crossing the legs and tucking the legs under were also identified. It was learned that none of the patients had previously been diagnosed with thrombosis. Eight of them had deep vein thrombosis in the lower extremities, two had pulmonary embolism, and one had left subclavian vein thrombosis. File records showed that genetic thrombosis panels were sent to ten patients with a positive family history. Mutations were detected in nine of these patients. Major risk factors such as protein C deficiency, prothrombin G20210A and Factor V Leiden mutations were detected in five patients.
The duration of immobility associated with digital device use, reasons for exposure to digital screens, and genetic risk factors in thrombotic patients are shown in Table 3.
Duration and Reasons for Screen Exposure, Diagnoses, and Hereditary Thrombophilia Results of the Study Group.
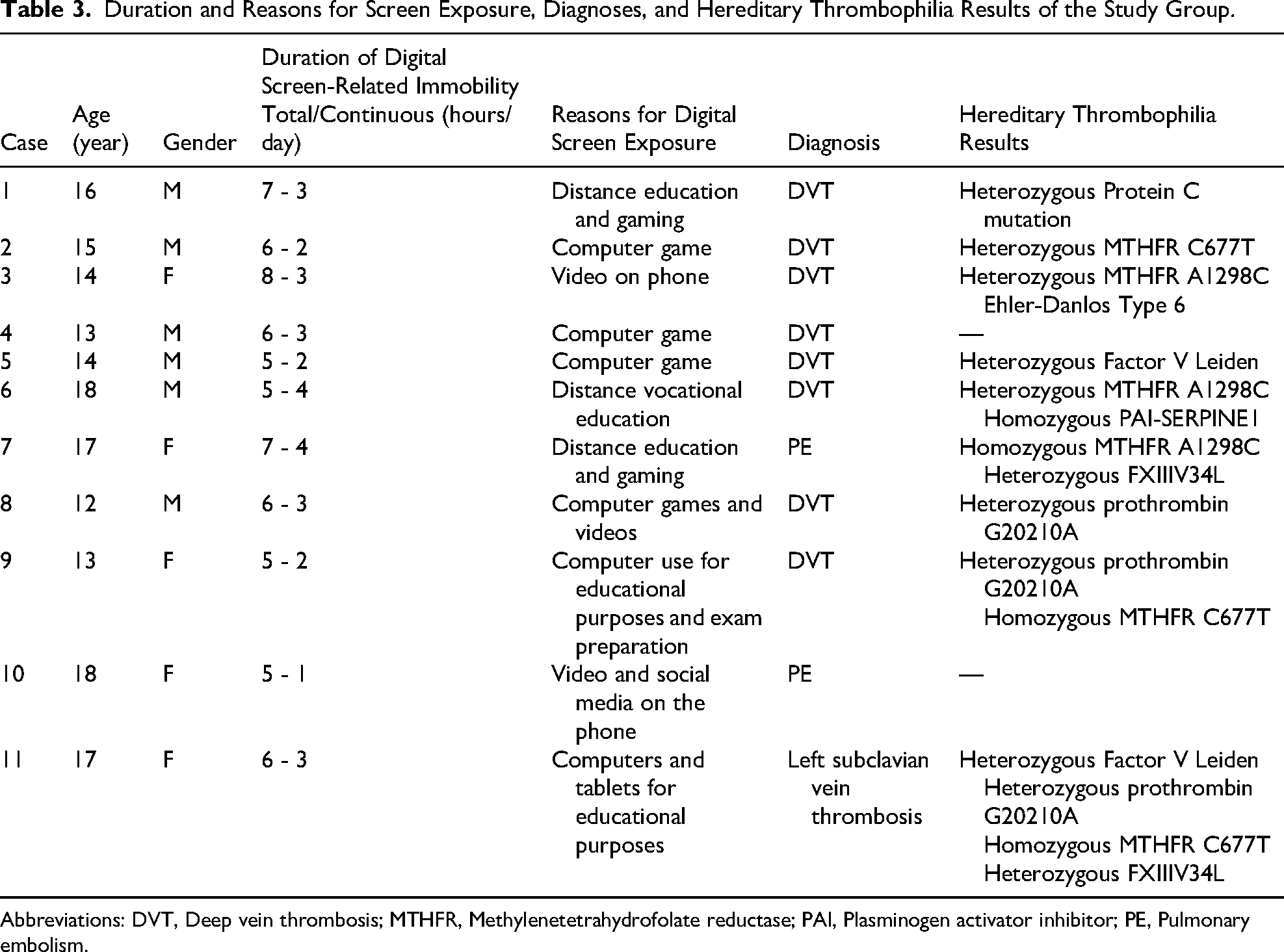
Abbreviations: DVT, Deep vein thrombosis; MTHFR, Methylenetetrahydrofolate reductase; PAI, Plasminogen activator inhibitor; PE, Pulmonary embolism.
Examination of the patients’ presenting complaints revealed that those diagnosed with deep vein thrombosis had pain, swelling, and redness in their legs; those diagnosed with pulmonary embolism had chest pain, cough, and shortness of breath; and the patient diagnosed with left subclavian vein thrombosis had swelling and pain in their left arm. In addition to blood tests, Doppler ultrasound and Thoracic Computed Tomography Angiography imaging methods were used to confirm the diagnoses. All patients received low molecular weight heparin therapy (2-6 months). The patient with protein C deficiency was started on prophylactic oral anticoagulant therapy after low molecular weight heparin therapy. Thrombectomy was performed in one patient (diagnosed DVT) who was resistant to treatment. The 11 patients we included in the study were informed about avoiding prolonged immobilization and leg and foot exercises. These patients are currently being monitored, and their thrombosis has not recurred.
Discussion
In the literature, prolonged screen exposure in children has been associated with numerous adverse psychological (depression, anxiety, attention deficit/hyperactivity disorder, behavioural problems), physical (obesity, metabolic syndrome, posture disorders, sleep disorders, chronic neck and back pain, language skill deficiencies) and social (social isolation, decreased communication and empathy skills) effects of prolonged screen exposure in children. 7 However, awareness and scientific publications regarding the increased risk of thrombosis, a potential and serious complication of a sedentary lifestyle associated with this type of exposure, are quite limited.
Thrombosis resulting from prolonged immobilization associated with use of digital device (gaming-screen addiction or educational-occupational requirements) is currently referred to as e-thrombosis.2,6 Although the prevalence of prolonged seated immobility (especially orthopedic surgery, long trip, bedridden illness…) is estimated to be between 16% and 34% of all VTE episodes, 8 it is not known how many of these are use of digital device-related. Although the prevalence of e-thrombosis is not yet known, it has been reported that the annual incidence of thromboembolism has increased in adolescents with intense contact with technology in recent years.2,9 Studies on technology addiction and an increase in thrombosis cases with the COVID-19 pandemic support these predictions.2-4 Most of these patients are adolescents who were monitored during the pandemic and have digital screen addiction. Their parents have also confirmed that these habits continue.
It is known that hereditary and acquired risk factors play a role in the development of thrombosis. In the pathogenesis, slowing of blood flow (stasis), hypercoagulability (disruption of hemostasis balance), and endothelial damage, called Virchow's triad, play a central role.1,2,8,9 In immobilization, although stasis is prominent among these three, endothelial damage and coagulability have also been shown to increase.1,9,10 Studies have drawn attention to an increase in fibrinogen and hemoglobin concentration (hemoconcentration) and up to a 4-fold decrease in popliteal vein flow during prolonged uninterrupted sitting. 1 Prolonged sitting position increases oxidative stress and impairs endothelial function. 11
Prolonged immobility was first described as a significant risk factor for thrombosis by Simpson in 1941 after he noted the development of pulmonary embolism in people in shelters during the London air raids in World War II. 12 In a study conducted by Homans in 1954, he reported that prolonged immobilization during car and airplane travel could trigger venous thromboembolism. 13 Today, e-thrombosis triggered by use of digital device-dependent immobility has been on the agenda since Beasley's definition in 2003. 6 In a cross-sectional study conducted by West et al in 97 patients with a diagnosis of VTE and 106 healthy control groups, it was reported that those who were sedentary for long periods while sitting at a computer had a 1.8-fold higher risk for VTE, and each 1-h period of sedentary sitting increased the cumulative risk of VTE by 10%. 14 In a cohort study comparing two groups of subjects with sedentary and dynamic jobs, a 28% higher risk of PE development was found in sedentary workers. 15 Digital device addiction increases in adolescence, which is one of the periods when the frequency of thrombosis peaks in children.16,17 Kohorts et al defined the triad consisting of obesity, sedentary lifestyle, and video games as a thrombophilia cocktail and reported 4 cases of use of digital device-dependent immobilization and thrombosis in adolescents. 18 Similarly, cases including adolescents who developed VTE as a result of technology-dependent long-term immobility have been reported in the literature.1,3,14,15,18-25 In our study, we found that our patients who developed thrombosis in the adolescent age group spent an average of 6 ± 1 h of sedentary time in front of computers, tablets, and phones for work, play, and education, with an average of 2.7 ± 0.9 h of uninterrupted sitting. Individuals with a genetic predisposition, in particular, face a higher risk of developing thrombosis, with the addition of acquired risks. Siniarski et al evaluated 493 patients aged 18–65 years with a history of VTE in their study investigating the relationship between thrombophilia and sitting inactivity and VTE, and found that 115 patients (24.5%) spent 8–12 h of sitting inactivity. In the analysis performed in patients with unprovoked VTE in the study, they revealed that Factor V Leiden (OR 4.05, 95% CI 2.12-7.76), prothrombin G20210A variant (OR 3.84, 95% CI 1.47-10.05) and computer use (OR 2.84, 95% CI 1.43-5.63) were independent predictors of thrombosis due to prolonged immobility. It has been reported that computer-related immobility associated with computer use can be considered an independent prothrombotic risk factor and, while not effective in the development of thrombosis on its own, can increase the risk of developing venous thromboembolism when combined with existing hereditary factors. 8 To our knowledge, our study is one of the few series focusing specifically on e-thrombosis in the adolescent population since the term e-thrombosis was first introduced. No other acquired risk factors other than inactivity were identified in our eleven patients who had prolonged sitting (1-4 h continuous). Mutations were detected in the genetic thrombosis panel in nine patients. Protein C deficiency, prothrombin G20210A and Factor V Leiden mutations are the leading causes of inherited thrombophilia. In addition, polymorphisms of the methylene tetrahydrofolate reductase (MTHFR) gene are common in the general population and there are publications supporting the association of these variants with increased prothrombotic risk. 26 One of our patients had a homozygous polymorphism of methylene tetrahydrofolate reductase (MTHFR) C677T, and the other had a homozygous polymorphism of MTHFR A1298C. Homocysteine levels in these patients were within the normal range. In these cases, the MTHFR gene mutation may not be the sole etiological factor, but rather contribute to cumulative risk when combined with other risk factors. With this study, we suggest that prolonged immobility may increase the cumulative risk of thrombosis, especially in adolescents with genetic risk factors.
It is predicted that digital exposure and addiction will increase in the coming years,1-5 and preventive measures should be taken against e-thrombosis as a potential risk factor that may develop alongside this. Correct sitting position, ergonomic desk-chair use (Figure 2a), avoiding crossed leg position and bending the knees while sitting (Figure 2b), increasing venous return by moving the feet (Figure 2c); taking a break every hour, limiting the time the screen is on; providing awareness trainings and evaluating pharmacologic prophylaxis options especially for individuals with genetic risk factors may be among the measures.1,2,14,16,18-20,23,25,27

(a) ergonomic working environment (b) avoid bending the knees (c) exercise with foot movements.
The limitations of our study include the limited number of patients included due to age group, the risk of recall bias, and the absence of a control group.
Conclusion
In this study, venous thromboembolism was detected in various regions in a group of adolescents exposed to an average of more than 6 h of digital screen time and approximately 3 h of uninterrupted sitting time per day. The most common diagnosis was deep vein thrombosis in the lower extremities. Genetic thrombophilia mutations, including Factor V Leiden, Prothrombin G20210A, and Protein C deficiency, were present in 9 of the 11 patients. These findings support the notion that prolonged immobility associated with digital device use may be a triggering factor for thrombosis, particularly in adolescents with underlying genetic predisposition.
Footnotes
Abbreviations
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. This study was approved by the Kırıkkale University Clinical Research Ethics Committee on 18.12.2024 with decision number 2024.12.05.
Consent to Participate
Written informed consent was obtained from the parents.
Consent to Publish
The authors confirm that human research participants gave informed consent for publication of the data. Approval is appropriate.
Authors’ Contributions
All authors contributed to the study conception and design. All authors read and approved the final manuscript. Study conception and design: Şule Toprak, Meryem Albayrak. Data Collection: Şule Toprak, Meryem Albayrak. Analysis and interpretation of results: Şule Toprak, Meryem Albayrak. Draft manuscript preparation: Şule Toprak, Meryem Albayrak. Critical revision: Şule Toprak, Meryem Albayrak.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.