
Abstract
Background
Oxidized regenerated cellulose (ORC) is a topical hemostatic agent, but its efficacy and safety in arthroplasty remain inconclusive. This meta-analysis aimed to comprehensively assess its role in this procedure.
Methods
We systematically searched multiple databases up to July 30, 2025, for cohort studies and randomized controlled trials investigating the use of ORC in arthroplasty. Study quality was assessed using standard tools, and data were analyzed using Stata software.
Results
A total of 33 articles were retrieved. After removing 27 duplicates, six high-quality studies involving 684 participants were included in the analysis. The analysis revealed that ORC significantly reduced total blood loss (WMD = −102.50 mL, 95% CI: −201.75, −3.26, I2 = 69.9%) and hemoglobin drop (WMD = −3.99 g/L, 95% CI: −6.19, −1.79, I2 = 39.8%) compared with the control group. No significant differences were found in other secondary outcomes, such as intraoperative blood loss, risk of thrombosis, operative time, or wound complications.
Conclusion
ORC is an effective and safe hemostatic agent that reduces total blood loss and hemoglobin drop during arthroplasty. Future research should focus on determining the optimal timing of ORC and long-term functional outcomes.
Keywords
Introduction
Joint replacement surgery serves as an effective treatment for end-stage joint disease. It is a common procedure for individuals with severe osteoarthritis. This intervention significantly enhances patients’ quality of life. The volume of these procedures has seen a progressive increase.1,2 Nevertheless, perioperative hemorrhage remains a significant clinical challenge. Studies indicate that total blood loss for total hip arthroplasty (THA) patients can range from 1000 to 1500 mL. For total knee arthroplasty (TKA) patients, this loss spans 1000–1025 mL. Such significant bleeding may necessitate allogeneic blood transfusion.3–5 This carries risks of infection and immune reactions. It also escalates healthcare costs and can even lead to mortality. 6 Current hemostatic strategies encompass systemic antifibrinolytic agents (eg, tranexamic acid), electrocoagulation, mechanical compression, and topical hemostatic materials like gelatin sponge and collagen. While tranexamic acid effectively reduces blood loss, its application in patients with thrombosis risk is debated.7,8 Electrocautery can inflict thermal injury on adjacent tissues. 9 Conventional hemostatic materials demonstrate limited efficacy in moist environments. They also carry risks of slow absorption or residual presence.10,11
Oxidized regenerated cellulose (ORC) has many applications in surgery. Previous studies have demonstrated its use in specialties such as neurosurgery, thoracic and cardiovascular surgery, general surgery, and gynecology.12,13 ORC effectively controls bleeding, reduces postoperative complications, and promotes tissue repair. Several related articles have been published, indicating its broad application prospects. This highly malleable material can conform to irregular bone surfaces and infiltrate intertrabecular spaces. ORC is therefore particularly suitable for orthopedic surgery.14–16 Furthermore, ORC is fully absorbable, eliminating the need for secondary removal. This reduces the risk of foreign body reactions. 17 Research also suggests that ORC may possess intrinsic antimicrobial properties. These properties could aid in preventing surgical site infections. 18 Despite these advantages, the efficacy and safety of ORC in joint replacement surgery have not been comprehensively evaluated.
Consequently, we conducted this meta-analysis to evaluate the effectiveness and safety of ORC for hemostasis in joint replacement procedures.
Methods
This meta-analysis was conducted per the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement and was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) (CRD420251052012). 19
Literature Retrieval
The literature search strategy strictly adhered to the PRISMA guidelines. Combining subject headings and free-text terms, we conducted a comprehensive review of studies published up until July 30, 2025, across five databases: Cochrane, Embase, Scopus, PubMed, and Web of Science. The terms comprised various types of ‘Joint Replacement/Arthroplasty, Replacement’, or ‘Joint Prosthesis Implantation’, and ‘Oxidized Regenerated Cellulose’, along with its brand names (Surgicel). Notably, our retrieval imposed no language restrictions. We employed broad search terms to maximize retrieval specificity (Table S1).
Eligibility Criteria
Eligible studies incorporated cohort studies and randomized controlled trials (RCTs) comparing the effect of ORC versus placebo in individuals undergoing joint replacement surgery. Inclusion criteria were: (i) Study population consisted of individuals undergoing joint replacement surgery; (ii) Intervention involved the use of ORC as a hemostatic agent; (iii) Primary outcomes were total blood loss and hemoglobin (Hb) decrease. Secondary outcomes included operative duration, intraoperative blood loss, occult blood loss, and postoperative complications. (iv) Study design was either a cohort study or an RCT. Exclusion criteria were: (i) Duplicate studies, systematic reviews, and meta-analyses; (ii) Literature reviews, case reports, non-English publications, animal experiments, letters to the editor, and narrative reviews; (iii) Studies with inaccessible full texts, inability to extract data, or non-compliance with data inclusion criteria.
Literature Screening and Information Collection
Two independent authors, Chenglong Xiao and Huang Liyin, screened articles using Zotero per the eligibility criteria. They reviewed the titles and abstracts to determine study eligibility. Any conflicts were resolved by Chai Sheng. Two review authors independently collected information from the eligible studies. This data included the first author, publication year, study type, sample size, surgical type, hemostatic agent type, and follow-up duration.
Total blood loss among study outcomes was calculated via the Gross method, encompassing changes in blood volume before and after surgery. The specific equation was: Total blood loss = Preoperative blood volume × (Preoperative hematocrit – Postoperative hematocrit) / Preoperative hematocrit.
Quality Evaluation
The quality of eligible articles was evaluated by two authors independently employing the National Institutes of Health (NIH) quality assessment tools. Discrepancies were resolved through discussion with a third author. Domains within the risk of bias (ROB) tool included assessment of randomization adequacy, allocation concealment, blinding of study participants and personnel, blinding of outcome assessment, management of incomplete outcome data, selective reporting, and identification of any other potential biases. The tool contained 14 evaluation items. Each item was judged as ‘Yes’ or ‘No’ based on the rigor of study design and implementation. All reviewers classified studies based on their ROB according to established criteria: studies scoring 0–5 were categorized as having high ROB (Poor), scores of 6–10 were considered to have fair ROB (Fair), and scores of 11–14 were deemed to have low ROB (Good).
Statistical Analysis
Data analysis was performed using Stata version 15.1 and the “metan” command. Continuous outcomes were expressed as a standardized mean difference (SMD) or a mean difference (MD), along with their respective 95% confidence intervals (CIs). For dichotomous data, the risk ratio (RR) and its 95% CI were computed based on the event counts and total sample sizes. Heterogeneity was evaluated utilizing the I2 statistic and the Q test. A random-effects model (REM) was employed for analysis when I2 > 50% and P < .05; otherwise, a fixed-effects model (FEM) was adopted. Sensitivity analyses were conducted to evaluate the robustness of the findings. Publication bias was evaluated using funnel plots and Egger's test when more than 10 studies were included. If significant bias was detected, the trim-and-fill method was applied to adjust its potential influence.
Results
Baseline Characteristics of Included Studies
Database retrieval yielded 33 articles. After removing 27 duplicates and conducting a thorough full-text review, the final meta-analysis comprised six studies (Figure 1).20–25

Basic flowchart.
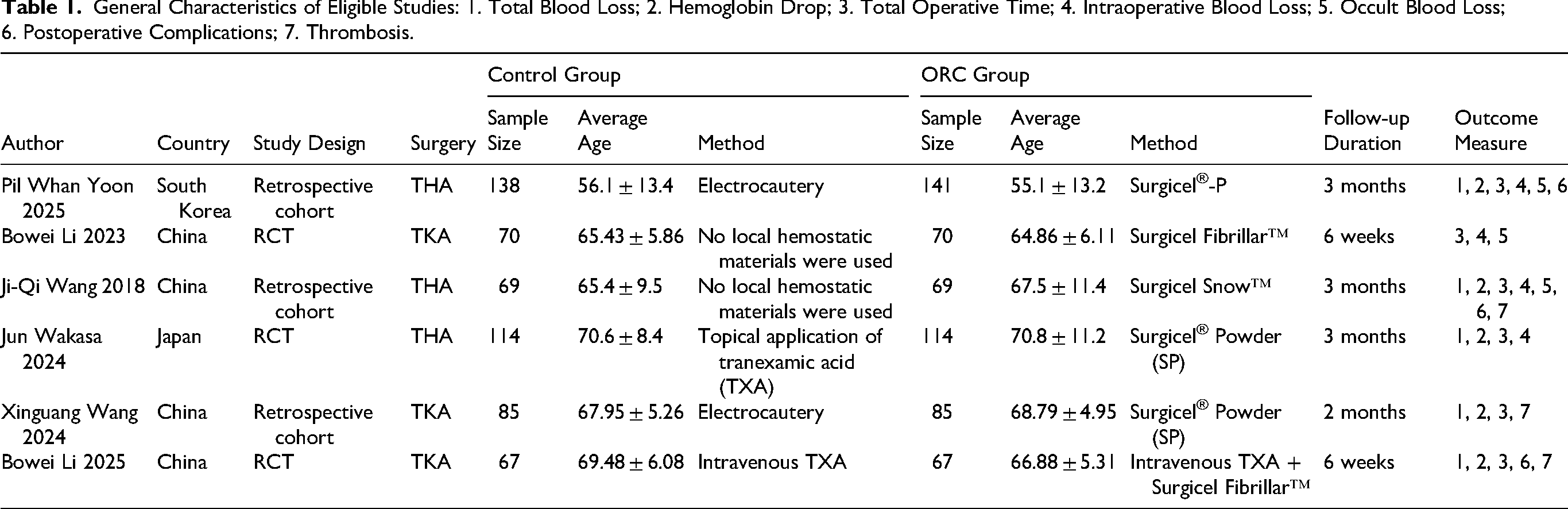
The eligible studies encompassed 684 subjects from China, Japan, and South Korea. Among these, three studies involved THA, with 462 subjects. Three studies focused on TKA, involving 222 subjects. Due to overlapping study populations and timeframes in two publications by Bowei Li et al, data from the more recent article were prioritized. Follow-up durations among the included studies were as follows: Bowei Li et al (six weeks), Xinguang Wang et al (two months), and Pil Whan Yoon et al, Ji-Qi Wang et al, and Jun Wakasa et al (all three months postoperatively) (Table 1).
General Characteristics of Eligible Studies: 1. Total Blood Loss; 2. Hemoglobin Drop; 3. Total Operative Time; 4. Intraoperative Blood Loss; 5. Occult Blood Loss; 6. Postoperative Complications; 7. Thrombosis.
Quality Evaluation
The quality of the eligible studies was generally high, with three studies employing a retrospective design and three being RCTs. The score range was 9–12. The retrospective studies demonstrated high quality, though specific deductions were primarily concentrated in the following areas. Firstly, the three retrospective studies did not provide adequate justification for sample size, power descriptions, or estimates of variance and effect, which might influence the interpretability of the findings. Secondly, outcome assessors in these studies were unblinded to exposure status, introducing potential assessment bias. Furthermore, the intervention (intraoperative ORC use) was inherently a single-event dichotomous variable, making blinded outcome assessment logically implausible. Consequently, Question 8 was not met. Additionally, some studies failed to adequately measure key potential confounding variables and did not employ appropriate statistical methods to adjust for them, which could affect the accuracy of the relationship between the exposure and the outcome. Given that this was a surgical study, outcome assessors needed to be aware of the subject's specific condition; thus, blinding was not implemented. Lastly, due to inherent design limitations, retrospective studies cannot be prospectively planned. Consequently, control over the aforementioned aspects was challenging, failing to meet the standards achievable by RCTs. The three RCTs could not fulfill blinding for subjects, surgical providers, or outcome assessors due to the nature of surgical research; surgeons needed to be aware of subject conditions, and subjects needed to be aware of their primary physician. These represented inherent limitations for such studies (Table S2A, Table S2B).
Primary Outcomes
Total Blood Loss
Five articles involving 614 subjects were encompassed. Analysis indicated that ORC significantly reduced total intraoperative blood loss. Heterogeneity testing revealed substantial heterogeneity among studies (I2 = 75.3%), thus an REM was applied. The pooled results demonstrated that ORC offered a significant advantage in reducing total blood loss compared to the control group (weighted mean difference (WMD [95% CI]): −102.50 [−201.75, −3.26]), with the difference being statistically significant (Figure 2). Sensitivity analysis, conducted by sequentially excluding individual studies, suggested that the findings were robust (Figure S1). Further subgroup analyses revealed that the intervention effect of ORC on total blood loss was more pronounced in the TKA group (−158.60 [−259.54, −57.66], I2 = 0.0%) across different surgical procedures. However, it did not reach statistical significance in the THA group (−69.90 [−219.46, 79.66], I2 = 86.7%) (Figure S2). In the subgroup analysis by measurement time, a significant effect was observed on postoperative day 3 (−191.22 [−259.26, −123.19], I2 = 0%), whereas the effect within the perioperative period did not reach statistical significance (−41.39 [−158.93, 76.16], I2 = 63.5%) (Figure S3).

Total blood loss.
Hb Drop
Five articles involving 614 participants were included to analyze the effect of ORC compared to placebo on postoperative Hb drop. Heterogeneity testing revealed moderate heterogeneity among the studies (I2 = 53.1%), thus an REM was employed. Pooled results indicated that ORC was superior to the control group in reducing Hb drop (−3.99 [−6.19, −1.79]), with statistical significance (Figure 3). Sensitivity analysis, performed by sequentially omitting individual studies, suggested the study conclusions were robust and reliable (Figure S4). Further subgroup analyses demonstrated that the intervention effect of ORC on Hb drop was more pronounced in the TKA group (−4.60 [−8.06, −1.14], I2 = 0.0%) across different surgical procedures. In the THA group, it also achieved statistical significance but with high heterogeneity (−3.44 [−6.81, −0.07], I2 = 75.5%) (Figure S5). For measurement time, a significant effect was observed on postoperative day 3 (−5.11 [−7.53, −2.69], I2 = 0%), while the effect within the perioperative period was not statistically significant (−2.85 [−7.37, 1.66], I2 = 74.0%) (Figure S6).
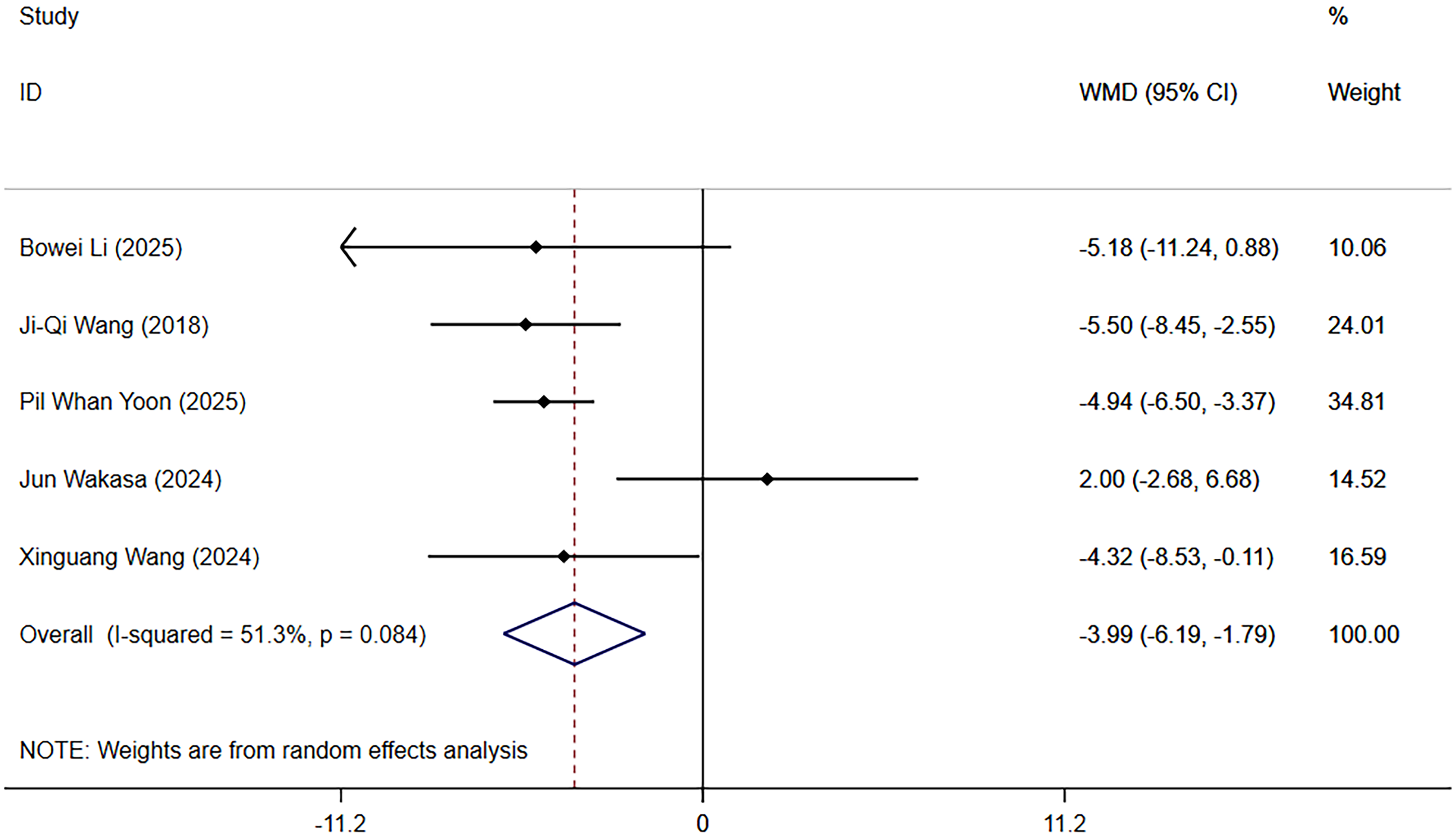
Hb reduction.
Secondary Outcomes
Total Operative Time
Five articles involving 614 subjects were incorporated to analyze the effect of ORC on operative duration relative to placebo. Heterogeneity testing indicated no heterogeneity (P = .532, I2 = 0.0%) among the study data. Analysis using an REM revealed no significant difference in operative duration between the ORC group and the control group (−1.94 [−4.08, 0.20]) (Figure S7). Sensitivity analysis, conducted by sequentially excluding individual studies, suggested that the findings were robust (Figure S8).
Intraoperative Blood Loss
Four investigations comprising 532 participants evaluated the effect of ORC versus placebo on intraoperative blood loss. Heterogeneity testing revealed extreme variability across studies (P = .000, I2 = 86.7 %). In a random-effects synthesis, the WMD was −27.37 (95 % CI: −55.84, 1.11), indicating no significant advantage of ORC over control (Figure S9). Sequentially omitting each study did not alter this conclusion, underscoring the robustness of the result (Figure S10).
Occult Blood Loss
Three studies including 418 subjects assessed the impact of ORC versus placebo on occult blood loss. Heterogeneity was high (P = .011, I2 = 77.9 %). Random-effects analysis showed significant benefits of ORC over control for occult blood loss (−104.27 [−206.53, −2.02]) (Figure S11). Sensitivity checks, removing one study at a time, confirmed the stability of this finding (Figure S12).
Wound Complications
Three studies with 415 participants examined the effect of ORC versus placebo on wound complications. No heterogeneity appeared (P = .668, I2 = 0.0 %). The random-effects odds ratio (OR) comparing ORC to control was 0.75 (95 % CI: 0.32, 1.75), revealing a statistically significant difference (Figure S13). Sequentially excluding individual studies preserved this outcome, demonstrating its durability (Figure S14).
Thrombosis
Three investigations comprising 221 subjects evaluated the influence of ORC versus placebo on muscular calf vein thrombosis (MCVT). Homogeneity was consistent (P = .405, I2 = 0.0 %). Random-effects synthesis yielded an OR of 1.06 (95 % CI: 0.68, 1.68), showing no significant disparity between groups (Figure S15). Omitting each study one after another left this result unchanged, confirming its stability (Figure S16).
Discussion
This meta-analysis comprehensively appraised the hemostatic efficacy and safety of ORC in joint arthroplasty. A systematic query of electronic databases was conducted, and evidence integration from six studies encompassing 684 subjects confirmed that ORC application in arthroplasty significantly reduced total blood loss and Hb decline, without increasing intraoperative blood loss, occult blood loss, or the risk of MCVT. It also exerted no negative impact on operative duration or wound complications, thereby substantiating its clinical safety profile.
The statistically significant differences observed in the primary outcomes have important clinical implications. First, in terms of blood loss reduction, the total perioperative blood loss in TKA typically reaches approximately 1000 mL, whereas the blood loss in THA is generally higher. Therefore, even a reduction of 100–200 mL could be significant for high-risk patients. Previous research suggests that, for every 200–300 mL reduction in perioperative blood loss, the need for an allogeneic red blood cell transfusion decreases by about 10%. 5 Second, regarding Hb decline, the postoperative Hb level is a key physiological indicator that influences a patient's early mobility, fatigue, and rehabilitation speed. The present study found that the ORC group experienced a smaller Hb drop. The magnitude of this reduction also holds significant clinical value. For patients with Hb levels at the lower limit of normal, this protective effect may prevent their postoperative Hb levels from falling into a range indicative of severe anemia. This could significantly lower the risk of developing anemia-related symptoms and establish a more favorable physiological foundation for early postoperative rehabilitation exercises. It may also indirectly reduce the time required to achieve functional recovery goals.26,27 Among the secondary outcomes, however, the effects of ORC on intraoperative blood loss, operative time, and wound complications did not reach statistical significance. The result for hidden blood loss was borderline, suggesting a potential, yet uncertain, clinical effect that requires validation through larger-scale studies.
Furthermore, moderate to substantial heterogeneity was observed across studies regarding the outcomes of total blood loss, Hb decline, intraoperative bleeding, and hidden blood loss. Inconsistencies in surgical sites and observation time points are likely primary sources of this heterogeneity. These methodological and clinical variations introduce uncertainty into the pooled effect estimates. Two subgroup analyses were performed by surgical sites and observation periods to address these heterogeneities. These analyses revealed that the efficacy of ORC exhibited significant anatomical site-dependency and time-effect characteristics. ORC demonstrated superior effectiveness in TKA compared to THA. The increased blood loss observed in the THA group within the study by Wakasa et al 22 may be attributed to the complex hip anatomy (rich deep vasculature), the ball-and-socket joint structure hindering uniform powder coverage of bleeding points, or a deeper surgical field. The time-measurement subgroup indicated pronounced efficacy on postoperative day 3. The study by Li et al 24 suggests this may be related to the mechanism of action of ORC powder. The present analysis incorporated both RCTs and retrospective cohort studies. Disparities in bias control and confounding adjustment inherent to these distinct study designs may further contribute to heterogeneity. Variability in the commercial ORC formulations used across trials—including differences in physical form, absorption rate, and mode of action—could also influence the consistency of hemostatic outcomes. Additionally, most of the included studies originated from China, Japan, and South Korea, where differences in healthcare systems, surgical protocols, and perioperative care standards are additional potential sources of heterogeneity.
Compared to conventional hemostatic methods, ORC offers advantages in moldability and flexibility. Its powder form enables penetration into trabecular bone spaces, the medullary cavity, pin tracks, screw holes, and fracture line gaps—areas often inaccessible to traditional agents like bone wax or gelatin sponges. It can also be delivered to deep surgical sites via minimally invasive instruments, potentially reducing the need for wider incisions.5,14,17,28,29 While gelatin sponges require several minutes of pressure and depend on the patient's intrinsic coagulation, ORC gelates within seconds upon blood contact, creating a micro-environment conducive to clotting and enabling rapid hemostasis.7,14,17 In contrast to methods like bone wax, which can persist as permanent foreign bodies and potentially impede bone union, ORC powder is fully absorbable, exerts minimal impact on bone healing, and avoids secondary trauma or surgery.10,11,30,31 Employing electrocautery for hemostasis in arthroscopic surgery can elevate the temperature of saline within the joint cavity; temperatures exceeding 43 °C may damage intra- and peri-articular tissues. Utilizing ORC powder does not induce such temperature increases.9,32 The acidic environment formed by ORC powder may inhibit the growth of certain microorganisms, conferring inherent antimicrobial properties compared to other hemostatic options and potentially reducing postoperative infection risk.18,33,34 Regarding operability, ORC powder can be sprayed directly onto the wound surface, requiring no specialized training and allowing quicker adoption by novices. The included studies indicated no significant difference in operative duration between procedures utilizing ORC and conventional techniques. 29 Pil et al 20 confirmed the applicability of ORC powder in the posterior approach for THA, addressing a gap left by previous research focused on the anterior approach and demonstrating the potential for expanded application.16,35 Although ORC use increases single-surgery material costs, the reduction in blood loss and complications shortens hospital stays, ultimately generating overall cost savings for both hospitals and patients. 36 Its application does not necessitate refrigeration or complex equipment, making it suitable for implementation in primary hospitals performing joint arthroplasty. 28 For complex bleeding scenarios or when seeking additional benefits beyond mere hemostasis (eg, adhesion prevention, healing promotion), standalone ORC application may have limitations. Therefore, exploring combination strategies integrating ORC with other hemostatic or adjunctive materials represents a highly promising direction for enhancing its clinical value and broadening its application scope. ORC powder also possesses inherent limitations. It is suitable only for low-to-moderate intensity bleeding and requires a relatively dry wound surface. If the site is flooded with blood, the powder can be washed away or excessively diluted, drastically diminishing its hemostatic effect.14,37,38 Its use is contraindicated in enclosed bony cavities or for direct contact with exposed nerves, as the acidic degradation products and mechanical compression may cause irreversible damage to neural tissue.39,40 In some patients, postoperative ORC residue may complicate radiographic interpretation, becoming a subject of differential diagnosis for abscess or fluid collection.41,42
This meta-analysis has several limitations. The relatively small number of eligible studies (n = 6) may affect the precision of the findings. The inconsistent observation periods across studies potentially introduce bias, necessitating future research with standardized measurement timepoints to minimize variability arising from perioperative assessment schedules. While both types of study designs included in the analysis were recognized as high quality, retrospective studies have inherent limitations regarding exposure assessment, confounding control, and blinding implementation. Therefore, combining these two distinct study designs may introduce certain bias. Although subgroup and sensitivity analyses were used to address this variability, future assessments should prioritize evidence synthesis based on large-scale, multicenter RCTs. Notably, long-term data are lacking; functional outcomes at ≥5 years postoperatively are absent, leaving the long-term efficacy of ORC unverified. Further investigations with extended follow-up are required.
Conclusion
In summary, this meta-analysis demonstrated the efficacy and safety of ORC for hemostasis in joint arthroplasty. ORC application significantly reduced total blood loss and Hb decline without increasing intraoperative blood loss, occult blood loss, or the risk of MCVT. Furthermore, it had no adverse effects on operative duration or wound complications. However, due to the small number of eligible studies and sample size, further RCTs are warranted to validate these findings.
Supplemental Material
sj-docx-1-cat-10.1177_10760296261420230 - Supplemental material for Effectiveness and Safety of Oxidized Regenerated Cellulose for Hemostasis in Joint Arthroplasty: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cat-10.1177_10760296261420230 for Effectiveness and Safety of Oxidized Regenerated Cellulose for Hemostasis in Joint Arthroplasty: A Systematic Review and Meta-Analysis by Chenglong Xiao, Huang Liyin and Chai Sheng in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Abbreviations
Acknowledgments
Not applicable.
Ethics Approval and Informed Consent Statements
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
All authors contributed to the study conception and design. Writing - original draft preparation: [Chenglong Xiao]; Writing - review and editing: [Huang Liyin]; Supervision: [Chai Sheng], and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing does not apply to this article as no datasets were generated or analysed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.