
Abstract
Keywords
Introduction
Heparin-induced thrombocytopenia (HIT) is a severe immune-mediated complication caused by heparin drugs during anticoagulant therapy. It is characterized by the formation of antibodies against the complex of heparin and platelet factor 4 (PF4).1,2 Such immune complexes further initiate coagulation. The clinical signs and symptoms include a significant decline in the platelet count (thrombocytopenia), thrombosis, and ulcerating skin lesions. These all lead to financial and health burdens.1,3 Anti-PF4/heparin antibodies have been uncommonly detected in healthy individuals with an incidence of only 0.3% to 0.5%.4,5 Most HIT cases usually occur after heparin exposure—especially unfractionated heparin (UFH)—either prophylactically or therapeutically. 6
Patients undergoing total hip arthroplasty (THA) and total knee arthroplasty (TKA) are recommended to receive routine chemical thromboprophylaxis7,8 to prevent severe complications. These include deep vein thrombosis (DVT) and pulmonary embolism (PE). Although the incidence of thrombotic complications after THA or TKA has decreased substantially, the use of heparin carries a risk of potentially resulting to HIT. Therefore, HIT after THA or TKA has become increasingly common and has led to a higher risk of hemorrhage and thrombosis. 9
Currently, there is no large-scale study on HIT in post-THA and post-TKA patients. Hence, the aim of this study was to investigate the incidence and risk factors of HIT in patients after TKA or THA using the National Inpatient Sample (NIS) database. To the best of our knowledge, this is the first study based on a large sample size that focuses on HIT after THA or TKA.
Material and Methods
This retrospective cohort study was conducted using the NIS database. This database has been recognized as the largest national database in the United States since 1998. 6 We investigated patients who underwent either THA or TKA in the United States from 2005 to 2014. The patients were identified according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 CM) procedure codes 81.51 and 81.54. For each procedure, the identified patients were divided into two groups, according to the presence of postoperative HIT (ICD-9 code 289.84). Those who were diagnosed with thrombocytopenia unrelated to heparin exposure were excluded. Studies on the baseline characteristics, hospital conditions, and risk factors of HIT were performed.
A chi-square test was used to evaluate the categorical variables which included grouped age and gender. A rank-sum test was used to assess the continuous variables including age, Charlson Comorbidity Index (CCI), Elixhauser Comorbidity Index (ECI), length of hospital stay (LOS), and total medical cost. CCI aggregated the prognostic burden of comorbid diseases. This index was used as an indicator to predict 1-year mortality. The ECI was applied to identify elevated mortality or hospital readmission risks. In addition, a logistic regression analysis was conducted to analyze the potential predictors of HIT. The odds ratios (OR) and 95% confidence intervals (CI) were calculated. The level of statistical significance was defined as P < .05. 6 All analyses were performed using the SPSS version 23 software (IBM; Armonk, New York).
Results
A total of 593 045 patients undergoing THA and 1228 707 patients undergoing TKA were identified (Figure 1). The annual incidence of HIT from 2005 to 2014 is shown in Figure 2. The baseline characteristics and hospital conditions are presented in Table 1. The predictors for postoperative HIT are summarized in Table 2.

Flow diagram of the study population. Abbreviations: NIS, national inpatient sample; ICD-9 CM, International Classification of Diseases, Ninth Revision, Clinical Modification; HIT, heparin-induced thrombocytopenia.
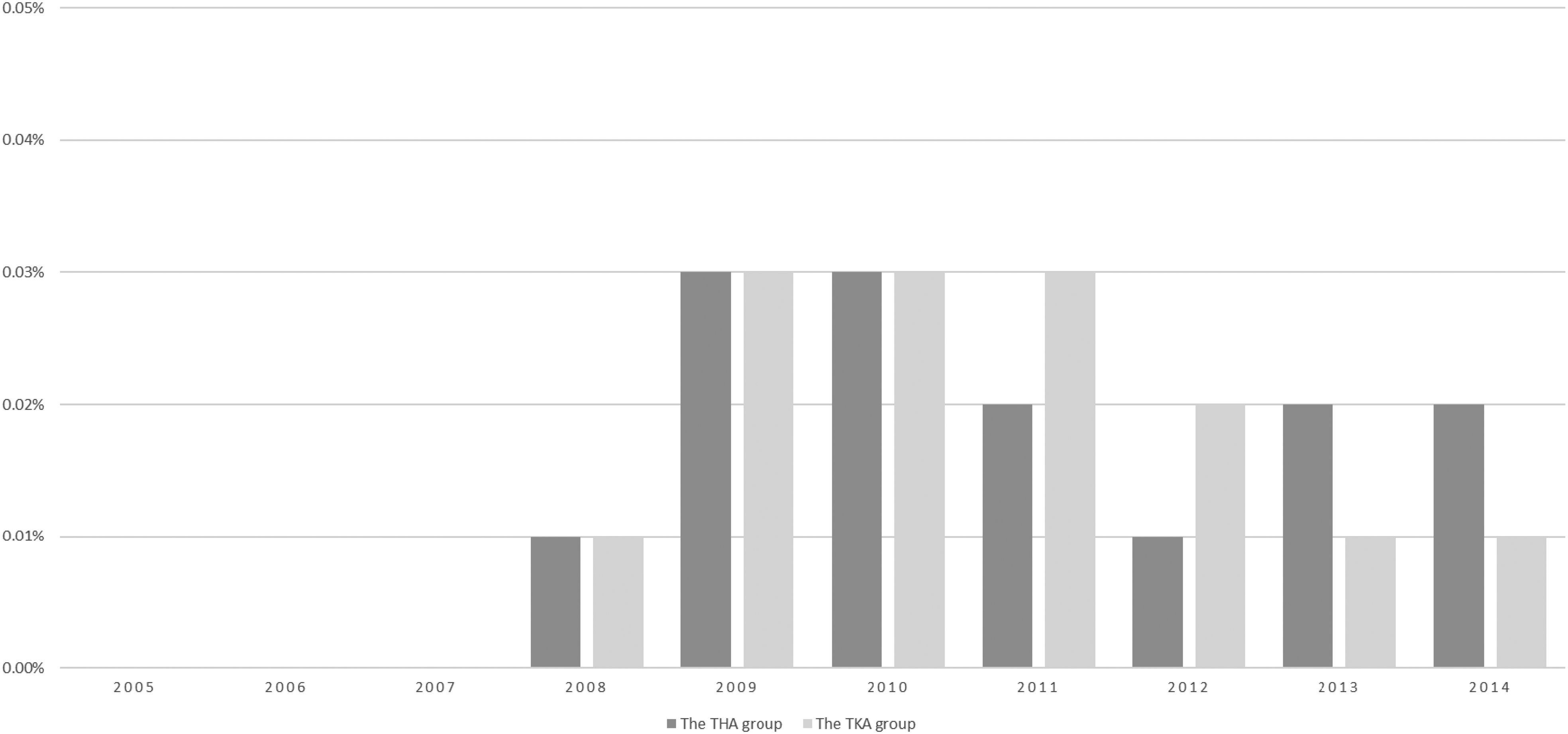
Incidence of HIT in patients undergoing THA and TKA from 2005 to 2014. Abbreviations: HIT, heparin-induced thrombocytopenia; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Baseline and Hospital-Level Characteristics of Patients Undergoing Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA).

Charlson Comorbidity Index.
Elixhauser Comorbidity Index.
The length of hospital stays. The impact of HIT on mortality was evaluated by the Fisher's exact test.
Predictors of HIT in Patients Undergoing Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA).

Odds Ratios.
95% Confidence Intervals.
Acquired Immune Deficiency Syndrome.
Rheumatoid arthritis or collagen vascular diseases.
Weight loss. Weight loss is not strictly defined per ICD-9 coding criteria; rather, it is determined by the discretion of the health care provider.
HIT After THA
The inpatient mortality was significantly higher in patients with HIT after THA (2.17% vs 0.16%, P = .091). Patients in the HIT group had significantly higher CCI and ECI scores, longer hospital stays, and more burdensome medical costs (P < 0.0001).
Racial minorities (OR = 2.60, 95% CI 1.02-6.63, P = .0452), AIDS (OR = 5.86, 95% CI 1.27-27.12, P = .0236), pulmonary circulation disorders (OR = 4.14, 95% CI 1.83-9.40, P = .0007), psychoses (OR = 2.63, 95% CI 1.08-6.40, P = .0326), and hypertension (OR = 2.57, 95% CI 1.47-4.50, P = .0010) were identified as independent risk factors of postoperative HIT. The protective factors were large-scale hospitals (OR = 0.46, 95% CI 0.27-0.80, P = .0059) and teaching hospitals (OR = 0.58, 95% CI 0.36-0.91, P = .0182).
HIT After TKA
The median ages (71 vs 67 years, P < .0001) and the proportions of patients over 70 years (51.74% vs 35.45%, P < .0001) in the HIT group were significantly higher. Races other than Caucasians earned higher percentages in the HIT group as well (P = .0335). The proportion of females in the HIT group was significantly lower (51.16% vs 62.87%, P = .0019). Although not statistically significant, HIT was demonstrated to result in a higher death rate after TKA (0.58% vs 0.07%; P = .1178). Additionally, the HIT group presented significantly higher CCI and ECI scores, longer hospital stays, and more burdensome medical costs (P < .0001).
Patients from other minor racial ethnicities (OR = 2.33; 95% CI 1.12-4.83; P = .0228), pulmonary circulation disorders (OR = 4.38; 95% CI 2.50-7.65; P < .0001), and weight loss (OR = 2.75; 95% CI 1.08-6.99; P = .0332) were identified as risk factors for HIT. The protective factors were teaching hospitals (OR = 0.68; 95% CI 0.48-0.96; P = .0280).
Discussion
THA and TKA are the most frequently performed joint replacement surgeries. The annual demands for primary THA and TKA are estimated to reach 174% and 673% by the year 2030, respectively. 10 Patients undergoing total joint arthroplasty (TJA) have a high risk of developing thrombotic complications due to reduced blood flow, thrombophilia, and damage to the venous linings.11–14 Thus, after TJA, patients are recommended to routinely receive prophylactic anticoagulation. 13 However, HIT—one of the most dangerous pro-thrombotic disorders—may occur during anti-thrombotic prophylaxis.1,9,15 HIT patients have a higher risk of developing paradoxical thrombotic syndrome.16–18 Hence, it is critical to understand the incidence and risk factors of HIT.
Despite the performance of TJA soaring from 2005 to 2014, the incidence of HIT after TJA has remained at 0.01% to 0.03%. This is consistent with the results reported by Craik. 7 In 2008, the American Academy of Orthopedic Surgeons (AAOS) released a guideline recommending thromboprophylaxis after TJA. 11 Thereafter, chemoprophylaxis has been done more routinely.7,9,19 Although it has not been commonly diagnosed, HIT has been recognized as one of the thromboembolic complications of patients after TJA, which might result in many postoperative adverse effects. Interestingly, compared with the incidence of postoperative HIT to other procedures, Dhakal et al 20 reported that the risk of HIT after TJA was lower. A possible explanation might be the application of low molecular weight heparin (LMWH) rather than UFH. Thus, routine laboratory monitoring was not recommended for HIT after TJA.7,19,21 However, according to our study, the cases of inpatient mortalities in post-THA patients were 13.75 times higher (2.2% vs 0.16%) and 8.3 times higher than in post-TKA patients (0.58% vs 0.07%), respectively. It is critical to identify the HIT risk factors and keep in mind that HIT may take place during LMWH exposure.
There have been controversial conclusions about the risk factors of HIT. In contrast to our results, Warkentin et al 22 and Chaudhry et al 23 found the female gender as a risk factor to HIT. This may be due to the different immune responses after various surgeries, 23 or the different thromboprophylactic therapies employed. 22 The racial differences 24 and polymorphism variabilities 25 have also been reported by other researchers. For example, non-Caucasians had higher thrombotic risks of HIT development after undergoing any procedure on their current admission. 24 Furthermore, in our results, large hospitals and teaching hospitals were detected as protective factors after THA. This finding may be attributed to the fact that surgeons in large hospitals and teaching hospitals are more experienced and professional in the perioperative management of HIT. However, the relationship between these factors and the occurrence of HIT may be related rather than causal, and it is worthy of further study.
The study of preoperative comorbidities may be valuable in preventing HIT. For THA, AIDS, hypertension, psychoses, and pulmonary circulation disorders increased the risk of postoperative HIT. In TKA patients, pulmonary circulation disorders and weight loss were identified as risk factors. To date, there is no established mechanism able to explain the above findings. One possible explanation is the formation of nonspecific and dysregulated antibodies triggered by pathological processes. 26 Specially, in the case of psychoses, the combined use of heparin and psychotropic medications may result in adverse hematologic effects. 27
The application of novel anticoagulants may provide a good opportunity of decreasing HIT. Argatroban and lepirudin, both direct thrombin inhibitors, have been estimated to have comparative efficacy and safety in the management of HIT. 28 Danaparoid has been found to have less influence on platelets compared with other anticoagulants because it inhibits factor Xa selectively. 29 However, given the low incidence of HIT after TJA, LMWH is still able to be used as the chemoprophylaxis after TJA in patients without a history of HIT.11,13,14
This study had several limitations. First, as a retrospective study utilizing the NIS database, coding and data-entry errors may have existed and led to an erroneous estimation of the HIT. The misdiagnosis or missed diagnosis of HIT, as well as the delayed onset in some HIT cases might also result in statistical deviation since the NIS database could only record complications during hospitalization. Second, the limited elements and absence of follow-up in the NIS database made it impossible to analyze the long-term HIT outcomes. For instance, heparin and other anticoagulants such as warfarin sodium are classified under the same code (964.2) in the ICD-9 code. Therefore, it is impossible to distinguish patients receiving heparin treatment from other anticoagulants treatment, which may lead to different risks of HIT. Finally, the different risk factors of HIT after THA and TKA were identified without established mechanisms. Bias in the medical records, utilization of tourniquet in the TKA, and the different seroconversion rates of anti-PF4/heparin antibodies between the two procedures 30 might have contributed to the difference in the results. Further prospective, evidence-based studies are needed to determine the exact causalities between comorbidities and HIT.
Conclusions
According to our study based on large sample size, the incidence of HIT in patients undergoing THA and TKA is relatively low. However, HIT significantly increases inpatient mortality. Thus, considerable attention and further investigations regarding HIT are warranted. Orthopedic surgeons should remain vigilant to the occurrence of HIT during postoperative anticoagulant therapy. They should also be aware of the risk factors of HIT to further improve patient outcomes.
Footnotes
Authors’ Contributions
Y. H. C., J. W., Z. J. S., and Y. Z. performed this study, analyzed and interpreted data; J. W., Y. Z., and Y. H. C. designed the study; Q. F. Y. and Y. C. X. carried out data collection; and Y. H. C. and Y. Z. wrote the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.