
Abstract
Background
Thrombolysis remains a key treatment for mechanical left-sided valve thrombosis, but outcomes vary across agents and patient groups. We evaluated thrombolysis effectiveness and predictors of failure in a large single-center cohort.
Methods
We performed a retrospective cohort study of all patients with mechanical left heart valve thrombosis treated with thrombolysis at the Narayana Institute of Cardiac Sciences, Bangalore, from January 2013 to December 2023. Clinical, echocardiographic, and treatment data were obtained from the emergency registry and medical records. The primary outcome was successful thrombolysis, defined as complete restoration of valve function on echocardiography by hospital discharge without in-hospital complications. Logistic regression identified determinants of failure (p < 0.05 significant).
Results
We analyzed 190 patients (median age 43 years, IQR 36-52; 50% female). Bi-leaflet valves were present in 81.1%, and streptokinase was most frequently used (57.9%). Overall, 145 patients (76.3%) achieved successful thrombolysis, while 45 (23.7%) failed treatment. Major ischemic events occurred in 7.4%, hemorrhage in 1.6%, and 13 patients (6.8%) died. On multivariable analysis, failure was independently associated with female sex (aOR 2.59, 95% CI 1.13-5.92), double valve replacement (aOR 6.40, 95% CI 2.48-16.56), anemia (aOR 5.02, 95% CI 1.55-16.28), streptokinase use (aOR 3.05, 95% CI 1.11-8.33), and absence of fluoroscopy prior to therapy (aOR 3.77, 95% CI 1.59-8.95).
Conclusion
Thrombolysis achieved a 76.3% success rate, consistent with global reports. Tenecteplase showed greater success and fewer complications than streptokinase. Accounting for sex, valve type, anemia, and fluoroscopy may improve outcomes in mechanical valve thrombosis.
Introduction
The global use of prosthetic valves continues to rise, driven by degenerative valvular heart disease in aging populations of developed countries and the persistent burden of rheumatic disease in developing regions. Surgical replacement remains the gold standard for advanced valve disease, and mechanical prostheses are the preferred choice for young patients with unrepairable left-sided valves. 1 These valves are durable but highly thrombogenic, requiring lifelong anticoagulation and close follow-up.
Major complications of mechanical valves include thrombosis, pannus formation, endocarditis, structural deterioration, regurgitation, prosthesis–patient mismatch, heart failure, and both thromboembolic and hemorrhagic events, with thrombosis being the most frequent. 2 Mechanical valve thrombosis is defined as thrombus formation adjacent to or attached to the prosthesis, in the absence of infection, causing obstruction that impairs valve function or restricts blood flow. 3 It usually presents as an acute or subacute event, often triggered by inadequate anticoagulation with vitamin K antagonists. Reported annual rates range from 0.1% to 5.7%, with an incidence of 0.5%–6% per patient-year for mechanical mitral and aortic valves. 1 In developing countries, the incidence may reach as high as 10% per patient-year. 4
Management requires rapid clinical and imaging evaluation to assess thrombus burden. Intravenous heparin should be started promptly, followed by thrombolysis or surgery depending on clinical status. 5 Emergency surgery is recommended for patients in New York Heart Association class III–IV or with large thrombi (>0.8 cm2), while patients in class I–II or with smaller thrombi (<0.8 cm2) may initially receive heparin, with thrombolysis reserved for persistent obstruction.6,7 Thrombolytic drugs are classified into first-, second-, and third-generation agents. Streptokinase and urokinase are non–fibrin-specific first-generation drugs, while recombinant tissue plasminogen activator and newer fibrin-specific agents such as tenecteplase and reteplase represent second- and third-generation options. 8
While studies from other regions have reported variable outcomes with different agents, local data remain limited. The present study aimed to evaluate the outcomes of thrombolysis in patients with mechanical left-sided valve thrombosis and to identify factors influencing success across commonly used thrombolytic agents. These insights may help guide therapeutic choices in this high-risk population.
Methods
Study Design and Setting
We conducted a retrospective cohort study at the Narayana Institute of Cardiac Sciences (NICS), Bangalore, India. The study period spanned from January 2013 to December 2023. All patients with confirmed mechanical left-sided valve thrombosis who underwent thrombolysis during this period were included. Patients were referred from surrounding hospitals and clinics or presented directly to the emergency department (ER), where they underwent initial evaluation, stabilization, and relevant investigations before admission.
Ethical Considerations
Ethical approval was obtained from the Narayana Hrudayalaya Ethics Committee (No. NHH/AEC-CL-2023-1077). The committee granted a waiver of informed consent due to the retrospective design. Patient confidentiality was ensured by assigning unique study identifiers unlinked to personal details. As no additional procedures were performed and only de-identified clinical records were used, no compensation was required.
Eligibility Criteria
We included patients with a diagnosis of mechanical left-sided valve thrombosis who received thrombolysis. Patients were excluded if they underwent primary surgical intervention, received escalation of vitamin K antagonists with intravenous unfractionated heparin instead of thrombolysis, or had incomplete clinical records.
Study Variables and Collection
The primary outcome was successful thrombolysis, defined as complete restoration of valve function during the index hospitalization, characterized by normalization of leaflet motion on echocardiography and normalization of mean transvalvular gradient for the affected valve, without in-hospital complications. Failure was defined as a mean gradient reduction of <50% from baseline, persistent leaflet restriction, or death from thrombolysis-related complications.
Secondary outcomes included in-hospital mortality, embolic stroke, and major bleeding. Major bleeding was defined as new-onset intracranial hemorrhage, as this event was reliably captured in the medical record and imaging reports. Other bleeding events (eg, gastrointestinal bleeding, access-site bleeding, hemoglobin drop, or transfusion requirement) could not be systematically adjudicated due to inconsistent documentation in retrospective records across the study period and were therefore not analyzed. Embolic stroke was defined as any new focal neurological deficit lasting ≥24 h, with brain imaging consistent with an ischemic origin.
Patients were identified from the NICS ER registry covering the 10-year study period. Clinical, laboratory, imaging, and outcome data were extracted from medical records using a standardized data collection form. Patients were followed until discharge from the hospital for assessment of outcomes.
Independent variables included sociodemographic data, clinical status, laboratory results, valve-related factors (position, type, size, duration since implantation, single vs double valve replacement, and anticoagulant used), and thrombolysis details (agent and dosing adequacy). Echocardiographic parameters included baseline and post-thrombolysis mean gradients and left ventricular ejection fraction (LVEF).
Blood pressure was classified as normal (systolic 100-140 mm Hg, diastolic 60-90 mm Hg) or abnormal if outside this range. Heart rate was considered normal between 60–100 beats per minute. Anemia was defined as hemoglobin <10 g/dL. International normalized ratio (INR) was categorized according to valve position: 2.0–3.0 for aortic valves and 2.5–3.5 for mitral valves. LVEF was categorized as reduced (<50%) or preserved (≥50%).
Thrombolytic Therapy and Dosing
The choice of thrombolytic agent was at the discretion of the treating physician. Streptokinase was administered as a continuous intravenous infusion regimen, while tenecteplase was given as a single intravenous bolus according to body weight. Dosing was considered adequate if streptokinase was administered as per the infusion protocol or if tenecteplase was weight-based. Any deviation was categorized as inadequate.
Statistical Analysis
Data were cleaned and analyzed using IBM SPSS Statistics, Version 26.0 (IBM Corp., Armonk, NY). Continuous variables were summarized as median with interquartile range (IQR), and categorical variables as frequencies and percentages. Group comparisons were performed using Pearson's chi-square or Fisher's exact test, as appropriate. Logistic regression was used to evaluate determinants of thrombolysis outcome. Variables with p < 0.10 on univariable analysis, as well as clinically relevant variables, were entered into multivariable models. Results are presented as odds ratios (OR) with 95% confidence intervals (CI). A two-tailed p < 0.05 was considered statistically significant.
Given the retrospective design, some variables were not uniformly documented in the medical record. Patients with incomplete clinical records were excluded from the analytic cohort at the eligibility stage. For analyses within the final cohort, we performed complete-case analysis for each comparison (denominators reflect available data). For multivariable logistic regression, observations with missing values in any included covariate were excluded by listwise deletion. No statistical imputation was performed.
Results
We identified 235 patients with mechanical left-sided valve thrombosis during the study period. After excluding five patients who did not undergo any intervention, 15 who underwent immediate surgery, 10 who were treated with intensified anticoagulation alone, and 10 with incomplete records, 190 patients formed the final study.
Baseline Characteristics
Table 1 summarizes patient characteristics. The median age was 43 years (IQR 36-52), with most patients between 31–40 years (33.7%) and 41–50 years (27.4%). The cohort had equal representation of men and women. The mitral valve was affected slightly more often than the aortic valve (51.1% vs 48.9%). Bi-leaflet prostheses predominated (81.1%), and most patients (82.6%) presented more than one year after valve replacement. Warfarin was the most frequently used anticoagulant (78.4%), and nearly three-quarters (73.7%) had an abnormal INR at admission.
Characteristics of Mechanical Valve Thrombosis Patient Who Underwent Thrombolysis (N = 190).

DBP: Diastolic blood pressure; INR: International normalized ratio; IQR: Interquartile range; LVEF: Left ventricular ejection fraction; SBP: Systolic blood pressure.
Thrombolytic Therapy and Outcomes
Among the 190 patients, 57.9% received streptokinase, 38.9% received tenecteplase, and only six received alternative agents such as reteplase, alteplase, or urokinase (Figure 1). Adequate dosing was achieved in 83.2% of cases, while 16.8% received inadequate dosing. Fluoroscopy was not performed before thrombolysis in 21.1% of patients. Forty-three patients presented with reduced left ventricular ejection fraction (LVEF <50%).
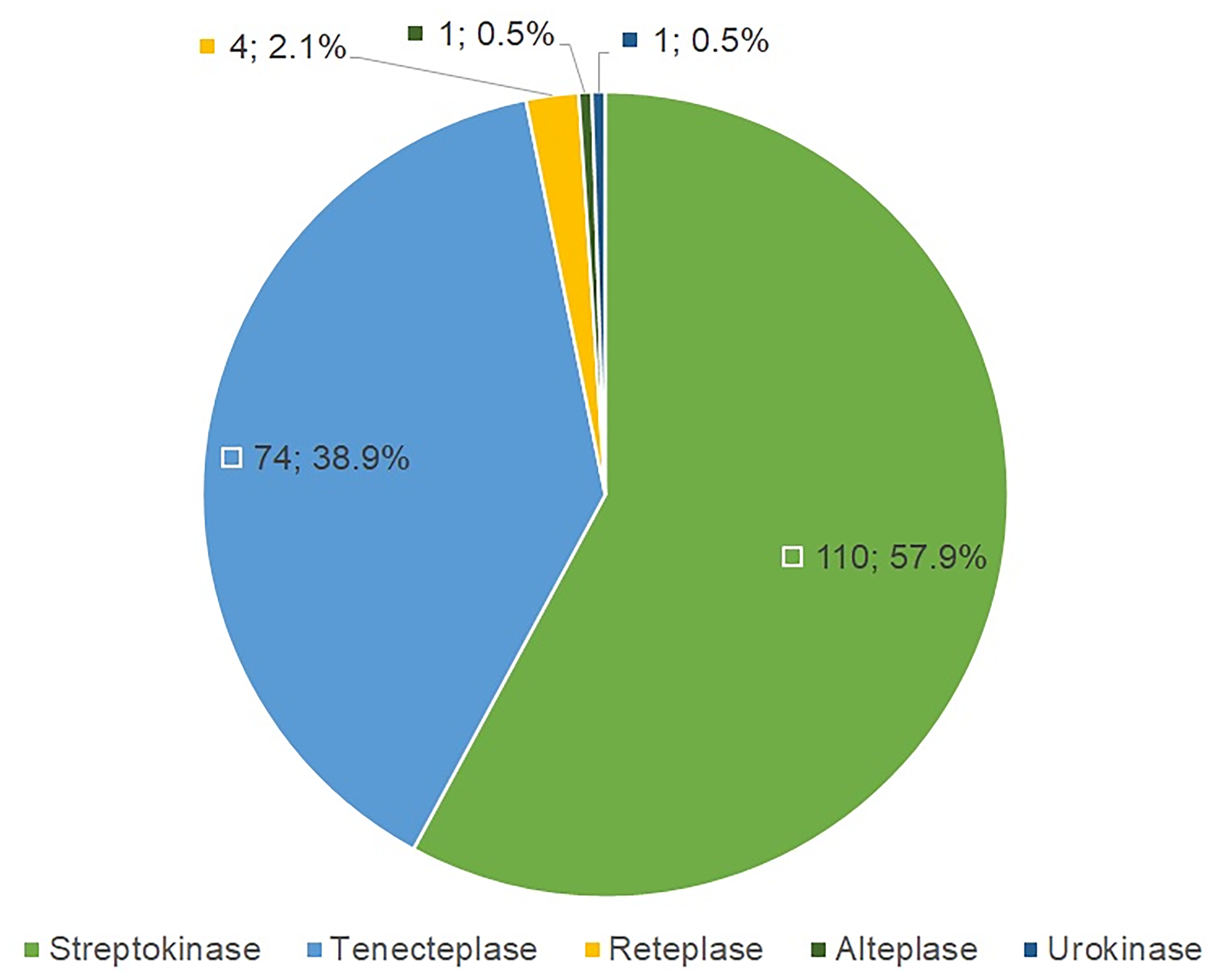
Distribution of thrombolytic agents used for mechanical left-sided prosthetic valve thrombosis (n = 190).
Overall, 145 patients (76.3%) achieved successful thrombolysis, while 45 (23.7%) experienced failure. Major ischemic events occurred in 7.4% of patients, whereas major hemorrhagic events were uncommon (1.6%). Despite thrombolysis, in-hospital mortality remained significant at 6.8% (13 patients), reflecting the severity of this condition. Survivors with failed thrombolysis proceeded to second thrombolysis, surgery during the same admission or a later admission, or sought further care elsewhere.
Comparison of Thrombolytic Agents
Outcomes differed between agents (Table 2). Tenecteplase tended to be used in older patients (27% were aged 51-60 years), whereas streptokinase was more frequently used in younger patients (36.4% aged 31-40 years). Patients with mitral valve thrombosis were more often treated with streptokinase (57.3%), while those with aortic valve thrombosis more often received tenecteplase (58.1%). Inadequate dosing occurred more frequently with tenecteplase (28.4%) than with streptokinase (10.0%). Despite this, tenecteplase was associated with higher success (82.4% vs 70.9%) and fewer complications. In-hospital mortality was also lower with tenecteplase (2.7%) than with streptokinase (10.0%).
Comparing Thrombolytic Agents among Patients with Mechanical Valve Thrombosis (N = 190).
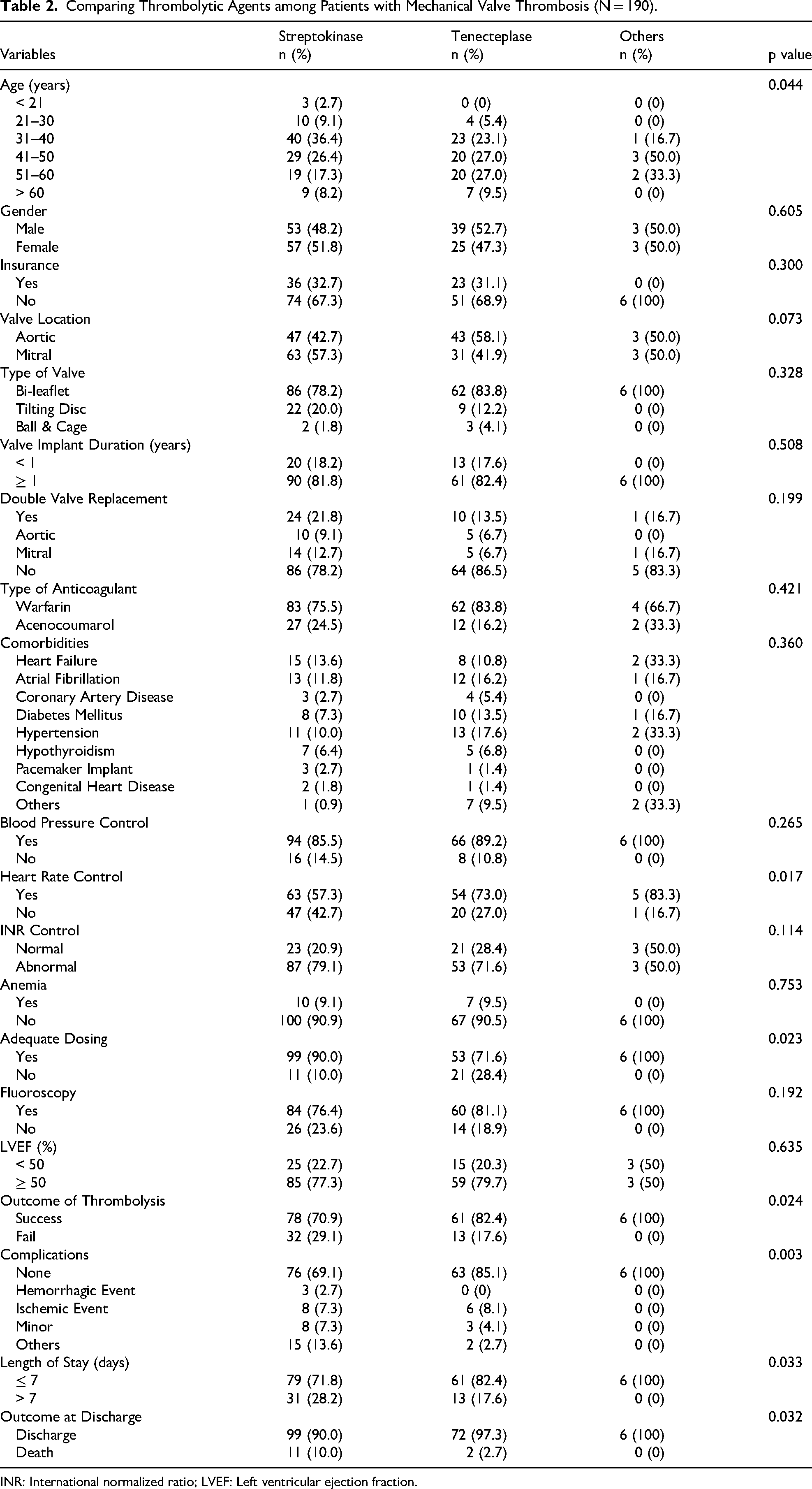
INR: International normalized ratio; LVEF: Left ventricular ejection fraction.
Determinants of Thrombolysis Failure
On univariable analysis (Table 3), failure was more likely among women (cOR 2.46; 95% CI 1.22-4.96; p = 0.011), patients with double valve replacement (cOR 4.28; 95% CI 1.97-9.34; p < 0.001), those with anemia (cOR 4.28; 95% CI 1.54-11.88; p = 0.003), and those who did not undergo fluoroscopy before thrombolysis (cOR 3.22; 95% CI 1.52-6.84; p = 0.002).
Factors Associated with the Outcome of Thrombolysis Among Patients with Mechanical Valve Hrombosis (N = 190).

aOR: Adjusted odds ratio; cOR: Crude odds ratio; INR: International normalized ratio; LVEF: Left ventricular ejection fraction
After adjustment, independent predictors of failure included female sex (aOR 2.59; 95% CI 1.13-5.92; p = 0.024), double valve replacement (aOR 6.40; 95% CI 2.48-16.56; p < 0.001), anemia (aOR 5.02; 95% CI 1.55-16.28; p = 0.007), use of streptokinase (aOR 3.05; 95% CI 1.11-8.33; p = 0.030), and lack of fluoroscopy before thrombolysis (aOR 3.77; 95% CI 1.59-8.95; p = 0.003).
Agent-Specific Predictors
When analyzed separately, predictors of failure differed by thrombolytic agent. Among patients receiving streptokinase (Table 4), failure was more likely in women (aOR 3.08; 95% CI 1.60-8.96; p = 0.039), those with double valve replacement (aOR 6.37; 95% CI 1.82-22.30; p = 0.004), and those who did not undergo fluoroscopy before thrombolysis (aOR 5.00; 95% CI 1.59-15.75; p = 0.006).
Factors Associated with the Outcome of Streptokinase Among Patients with Mechanical Valve Thrombosis (N = 110).

aOR: Adjusted odds ratio; cOR: Crude odds ratio; INR: International normalized ratio; LVEF: Left ventricular ejection fraction.
Among patients treated with tenecteplase (Table 5), double valve replacement (aOR 6.25; 95% CI 1.20-32.38; p = 0.029) and anemia (aOR 6.70; 95% CI 1.05-42.96; p = 0.045) emerged as significant predictors of failure.
Factors Associated with the Outcome of Tenecteplase Among Patients with Mechanical Valve Thrombosis (N = 74).
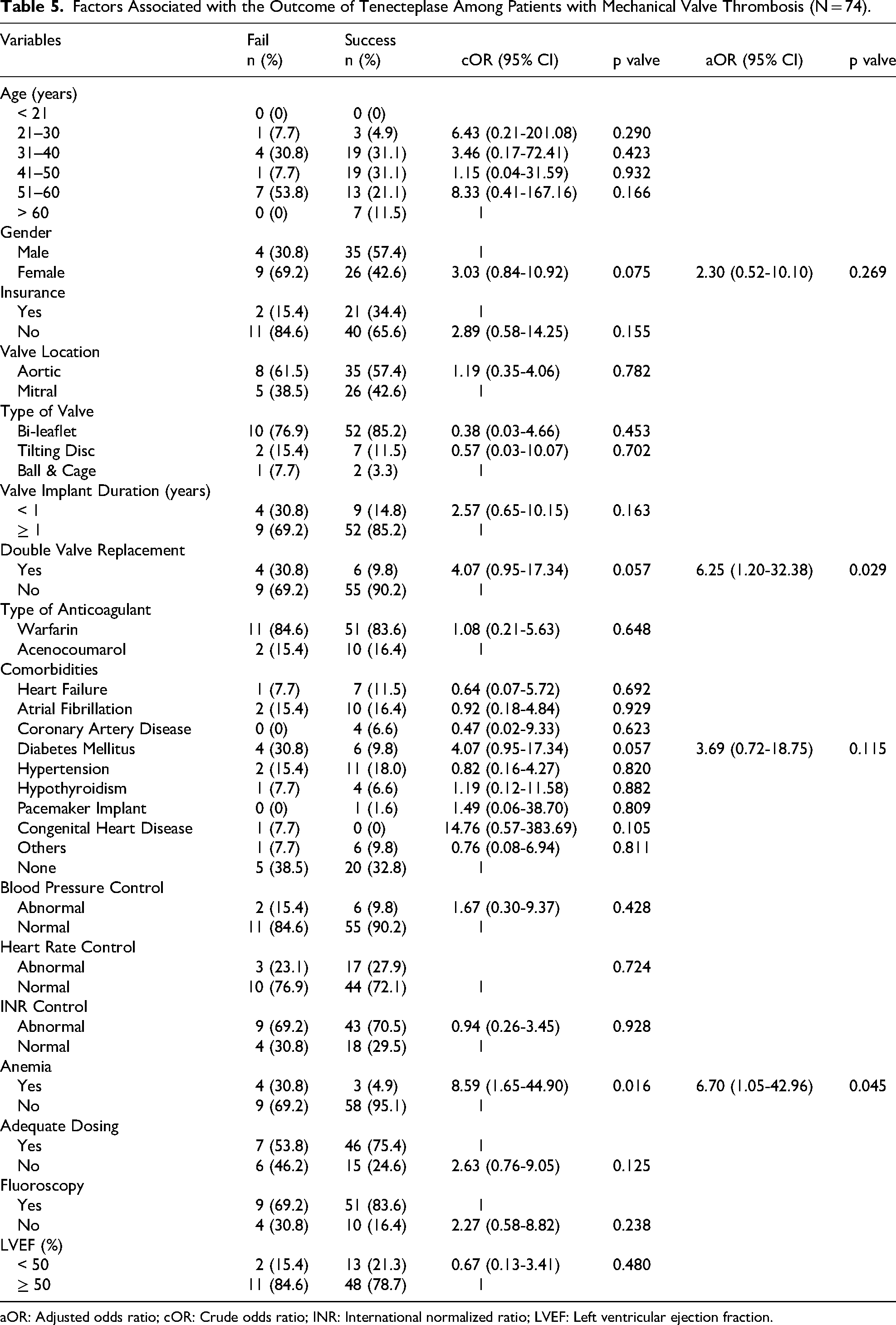
aOR: Adjusted odds ratio; cOR: Crude odds ratio; INR: International normalized ratio; LVEF: Left ventricular ejection fraction.
Discussion
In this retrospective cohort of 190 patients with mechanical left-sided valve thrombosis, we observed a 76.3% success rate with thrombolysis, with 23.7% experiencing failure. Complications were not uncommon: thromboembolism occurred in 7.4%, major hemorrhage in 1.6%, and in-hospital mortality in 6.8%. These results align with prior reports, where success rates ranged between 58%–90%, thromboembolic events between 1.7–17.6%, and major bleeding between 1.7%–12%. 9 Data from India also fall within similar ranges, with success rates of 59%–100% (average 78.1%) and mortality rates of 1.9–9.5% (average 5.4%). 9 Thus, our findings reflect the broader national and global experience with thrombolysis in this high-risk population.
Reported cerebrovascular complication rates after thrombolysis for mechanical valve thrombosis vary widely between centers and may appear higher in routine practice depending on patient mix (eg, higher NYHA class, larger thrombus burden, atrial fibrillation), surveillance intensity, and the thrombolytic regimen used. Prior studies suggest that low-dose slow or ultraslow alteplase infusion protocols guided by serial echocardiography can reduce embolic and bleeding complications compared with accelerated regimens, although real-world implementation and selection criteria differ across institutions.10,11
Mortality in our cohort (6.8%) was lower than the 12.5% mortality reported in a 2022 meta-analysis 12 and slightly below the 9% reported in an earlier 2013 meta-analysis. 13 Both meta-analyses highlighted increased risks of bleeding, systemic embolism, and recurrence following thrombolysis. A study from Australia reported an even higher in-hospital mortality of 16%, 14 possibly reflecting limited cardiothoracic surgical support. Our comparatively lower mortality underscores the potential benefit of having immediate surgical backup and specialized cardiac care available.
When outcomes were stratified by agent, tenecteplase achieved a higher success rate than streptokinase (82.4% vs 70.9%) and was associated with fewer complications and lower in-hospital mortality (2.7% vs 10%). These findings are consistent with other Indian studies that reported superior efficacy of tenecteplase, with success rates ranging from 75%–90% compared to 44–77.5% for streptokinase.15,16 The higher fibrin specificity and resistance to plasminogen activator inhibitor-1 (PAI-1) may explain the more favorable profile of tenecteplase. 17 Nevertheless, variability between centers emphasizes that outcomes remain context-dependent, influenced by patient selection, dosing practices, and supportive care.
We also identified independent predictors of thrombolysis failure. Female sex was strongly associated with poorer outcomes. While prior studies on valve thrombosis have not consistently examined sex differences, evidence from stroke thrombolysis supports a biological explanation. Women often exhibit higher PAI-1 levels, a recognized mediator of thrombolysis resistance. 18 Estrogen may modify this effect, as it lowers PAI-1 levels; however, declining estrogen levels with age could reduce the effectiveness of thrombolysis in older women.19,20 In our study, more women undergoing thrombolysis were older than 50 years, supporting this biological mechanism. These findings highlight the need to consider sex-specific factors when evaluating thrombolysis outcomes.
Double valve replacement was another significant predictor of failure. Prosthetic valves subject circulating platelets to abnormal shear stress, leading to platelet activation and release of mediators such as platelet factor 4. Patients with double valve replacement exhibit higher platelet activation markers than those with single valves. 21 Our findings suggest that this pro-thrombotic state may reduce the efficacy of thrombolysis and contribute to poorer outcomes.
We also found that absence of fluoroscopy prior to thrombolysis increased the risk of failure. Without fluoroscopy, some patients may have been misdiagnosed with thrombosis based solely on elevated gradients on echocardiography when pannus formation or mechanical dysfunction could have been the true cause. Thrombolysis in such cases would be ineffective. This underscores the importance of fluoroscopy in confirming prosthetic valve obstruction before initiating thrombolytic therapy.
Anemia also emerged as a strong predictor of failure, particularly in patients receiving tenecteplase. Anemia reflects both systemic illness and impaired oxygen delivery, which may amplify the hemodynamic burden of valve obstruction and blunt recovery even after lysis. It also often coexists with nutritional deficiencies, inflammation, or chronic comorbidities that may impair fibrinolysis. Identifying and correcting anemia may therefore improve the success of thrombolysis.
Strengths and Limitations
This study has several strengths. It represents one of the largest single-center series of thrombolysis for mechanical left-sided valve thrombosis in India, spanning a 10-year period with detailed echocardiographic and clinical data. We directly compared outcomes between streptokinase and tenecteplase, adding to the limited regional evidence on agent-specific differences. Furthermore, our analysis identified clinically relevant predictors of failure, including sex, double valve replacement, anemia, and lack of fluoroscopy, which may help guide decision-making in similar settings.
However, important limitations must be acknowledged. First, this was a retrospective single-center study, introducing inherent selection bias and limiting generalizability. We did not include a surgical comparator group, nor did we capture recurrence rates, as many patients may have sought follow-up elsewhere. Information on anticoagulation compliance and follow-up was incomplete, although these are known to influence thrombosis risk. Thrombus size was not analyzed due to inconsistent documentation, despite its established role in prognosis. Major bleeding was defined only as intracranial hemorrhage, as other bleeding parameters (hemoglobin drop, transfusion) were unavailable, which may have underestimated complication rates. Dosing practices also varied, particularly with tenecteplase, and while we classified adequacy, heterogeneity may have influenced outcomes. Finally, some patients were excluded for incomplete data, which may have introduced bias.
Conclusion
In this 10-year single-center experience, thrombolysis achieved a success rate of 76.3%, a figure consistent with global and Indian data. Importantly, outcomes were not uniform across agents. Tenecteplase was associated with higher odds of success and fewer complications than streptokinase, even though dosing was less often adequate. These findings suggest that tenecteplase may be the preferred fibrinolytic agent for mechanical left-sided valve thrombosis when thrombolysis is chosen.
Our study also identified key predictors of failure: female sex, double valve replacement, anemia, and the absence of fluoroscopy prior to therapy. These factors highlight the importance of individualized patient assessment. Incorporating fluoroscopy into diagnostic work-up, correcting anemia when feasible, and recognizing the heightened risk in women and double valve recipients may improve outcomes.
Based on these findings, clinicians should prioritize tenecteplase where available, ensure confirmatory imaging before lysis, and adopt risk-stratified decision-making in patients with mechanical left-sided valve thrombosis. Future prospective studies, ideally with standardized dosing and inclusion of thrombus burden, are warranted to validate these observations and further refine treatment strategies.
Footnotes
Acknowledgements
We thank the staff of Narayana Hrudayalaya for their co-operation during this study period.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Narayana Hrudayalaya Ethics Committee (No. NHH/AEC-CL-2023-1077). The committee granted a waiver of informed consent due to the retrospective design. The study was conducted according to the guidelines of the Declaration of Helsinki.
Author Contributions
Abid M. Sadiq – Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – Original draft.
Nithin P.R. – Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – Review & editing.
Pradeep Kumar Karkal – Methodology, Project administration, Supervision, Validation, Visualization, Writing – Review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
Anonymized dataset available on request from corresponding author.