
Abstract
Objective:
This study was planned to compare the efficacy of bolus regimens of tenecteplase (TNK) and 24 hours infusion of streptokinase (STK) in acute pulmonary embolism (APE) in a resource-poor setting.
Interventions:
In all, 25 patients received injection of TNK, and 75 patients received infusion of STK over 24 hours.
Results:
Pulmonary artery systolic pressure and right ventricular function were improved separately and significantly (P = .01) in both the study groups of patients from baseline at 24 hours or at seventh day and was comparable among the TNK and STK groups of patients. Mean duration of stay in intensive care unit was significantly less (2.2 ± 0.8 vs 3.2 ± 1.3 days; P = .04), and bleeding risk was also found to be nonsignificantly less in the TNK group.
Conclusion:
These results suggest that a 24-hour infusion regimen of STK is as effective as bolus TNK in the treatment of patients with APE in countries with limited resources.
Introduction
Pulmonary embolism (PE) is a common and potentially fatal disease that is still underdiagnosed in developing countries. Recent advancement of computed tomography pulmonary angiogram (CTPA) helped in the accurate diagnosis of PE and recent study described that it may overdiagnose PE. 1 Pulmonary embolism is the third most common acute cardiovascular disease after myocardial infarction and stroke. 2 Pulmonary embolism has an incidence in the general population approaching 1 to 6 of 1000. 2 Despite progress in the diagnosis and treatment of acute PE (APE), the mortality rate can reach up to 15% for high-risk patients. Although case fatality rates may vary widely, 2% of all cardiac arrests and 6.5% of cardiac arrests of extracardiac origin are due to APE. 3 Thrombolytic agents have been administered to patients with APE for almost 40 years. 4 In hemodynamically unstable patients, thrombolysis results in a significant reduction in death rates or symptomatic recurrence of PE. 5 Patients with low-risk PE have an unfavorable risk–benefit ratio with fibrinolysis. 6,7 The clinical benefit of thrombolytic treatment in hemodynamically stable patients with PE and right ventricular (RV) dysfunction (RVD) remains to be defined. Tenecteplase (TNK) is a triple-combination mutant variant derived from recombinant tissue-type plasminogen activator by the substitution of amino acids in 3 different locations of the original molecule. These changes lead to a longer plasma half-live, greater fibrin specificity, and greater resistance to plasminogen activator inhibitor 1. 8 It can therefore be administered as a single bolus dose over 5 to 10 seconds. The recommended dosing is from 30 to 50 mg based on patient’s weight. 9 –11 Tenecteplase is currently Food and Drug Administration (FDA) approved only for the thrombolytic therapy of acute myocardial infarction, not for the treatment of PE, 7 whereas both streptokinase (STK) and recombinant tissue plasminogen activator are currently FDA approved for the treatment of PE.
The present study was the first study to compare the fibrinolytic efficacy between TNK and STK to assess which of these 2 therapies can be administered in a resource-poor country.
Patients and Methods
Study Design
It was a prospective and comparative study. This study was conducted in a tertiary cardiac care institution in South India from November 2011 to May 2013.
Eligibility Criteria
Inclusion criteria: patients aged more than 18 years with APE (first symptoms 15 days or less before presentation) and confirmed by a positive findings in CTPA and echocardiography having RVD were included.
Exclusion Criteria
Patients with following criteria were excluded from the study: Symptoms started more than 15 days and/or without evidence of RVD. Administration of a thrombolytic agent in the previous 4 days or glycoprotein IIb/IIIa antagonists within the preceding 7 days. Vena cava filter insertion or pulmonary thrombectomy in the previous 4 days. Uncontrolled hypertension (systolic blood pressure [SBP] >180 mm Hg and/or diastolic blood pressure [BP] >110 mm Hg at presentation). Known hypersensitivity to STK, TNK, or heparin. Known coagulation disorder (including use of vitamin K antagonists and platelet count <100 000/mm3). Clinically relevant bleeding within the last 6 months or if they had a hemorrhagic diathesis, active peptic ulcer, arterial aneurysm or arterial/venous malformation, cancer at increased risk of bleeding, history of stroke, intracranial, or spinal surgery. Major surgery, biopsy, or trauma in the 2 months preceding the admission. Had prolonged cardiopulmonary resuscitation (>10 minutes) in the last 2 weeks. Severe hepatic or renal failure and subacute bacterial endocarditis.
Ethics
The study protocol was approved by the ethics committee of the respective authority of our institution. Written informed consent was obtained from all patients before inclusion in the study.
Methods
Written proformas will be filled up during inclusion of patients, which will contain epidemiological information (age, sex, occupation, and place), questionnaires for risk factor evaluation (smoking, drug history, malignancy, comorbid condition, and hypercoagulable state), information of clinical presentation (dyspnea, chest pain, syncope, cardiac arrest, etc), and clinical signs. Those patients had confirmed CTPA for APE and were treated per unit protocol with either TNK or STK. Most of our patients were from poor economic family, so mostly they were treated with STK. All the patients were prospectively studied; data were collected, compiled, and finally compared between STK and TNK treatment.
Investigations
All patients will be investigated with the following tests: Chest x-ray. Electrocardiogram (ECG): For all patients, standard 12-lead ECG was recorded on admission with a paper speed of 25 mm/s. The first available ECG was used for analysis. The following ECG parameters were analyzed
12
: supraventricular or ventricular arrhythmia; QRS axis deviation, P-pulmonale, amplitude of P wave greater than 0.25 mV in at least 1 limb lead (II, III, and aVF), right bundle branch block (RBBB); McGinn-White sign (S1Q3T3 complex); negative T wave in leads III and aVF; negative T waves in leads V2 to V4; T segment depression in leads V4 to V6; ST-segment elevation in leads aVR, III, V1, and V2 to V4. Echocardiography: Baseline echocardiography was to be done within 24 hours from the diagnosis of PE. For the purpose of this study, RVD was defined as the right/left ventricle end-diastolic dimension ratio >1 in the apical 4-chamber view and/or >0.7 in parasternal long axis, both in the absence of RV hypertrophy (RVH). Echocardiography was scheduled to be repeated 24 hours and at discharge or 7 days after study treatment administration. The pulmonary artery systolic pressure (PASP) was calculated using tricuspid valve regurgitation jet and inferior vena cava dimension.
10
Computed tomography pulmonary angiogram. Complete hemogram, bleeding time, clotting time, prothrombin time, activated plasma thromboplastin time (aPTT), renal function test, and liver function test. Doppler venography/ultrasound abdomen if necessary.
Treatment of the Study Patients
Tenecteplase was given as an intravenous weight-adjusted bolus (given over 5 seconds) at a dose ranging from 30 to 50 mg, with a 5-mg step up for every 10 kg body weight from <60 to ≥90 kg. This regimen is currently recommended for the treatment of acute myocardial infarction. Bolus of TNK was scheduled to be given within 6 hours from baseline echocardiography. All patients received unfractionated heparin (UFH) infusion of 1000 IU/h after giving bolus of TNK. Heparin dose was adjusted in order to achieve and maintain the aPTT at 2.0 to 2.5 × control. Vitamin K antagonists (VKA) were started preferably on the same day of study treatment administration or as soon as possible. Heparin was continued until the international normalized ratio maintained in the therapeutic range (2.0-3.0) in 2 consecutive days (Figure 1).
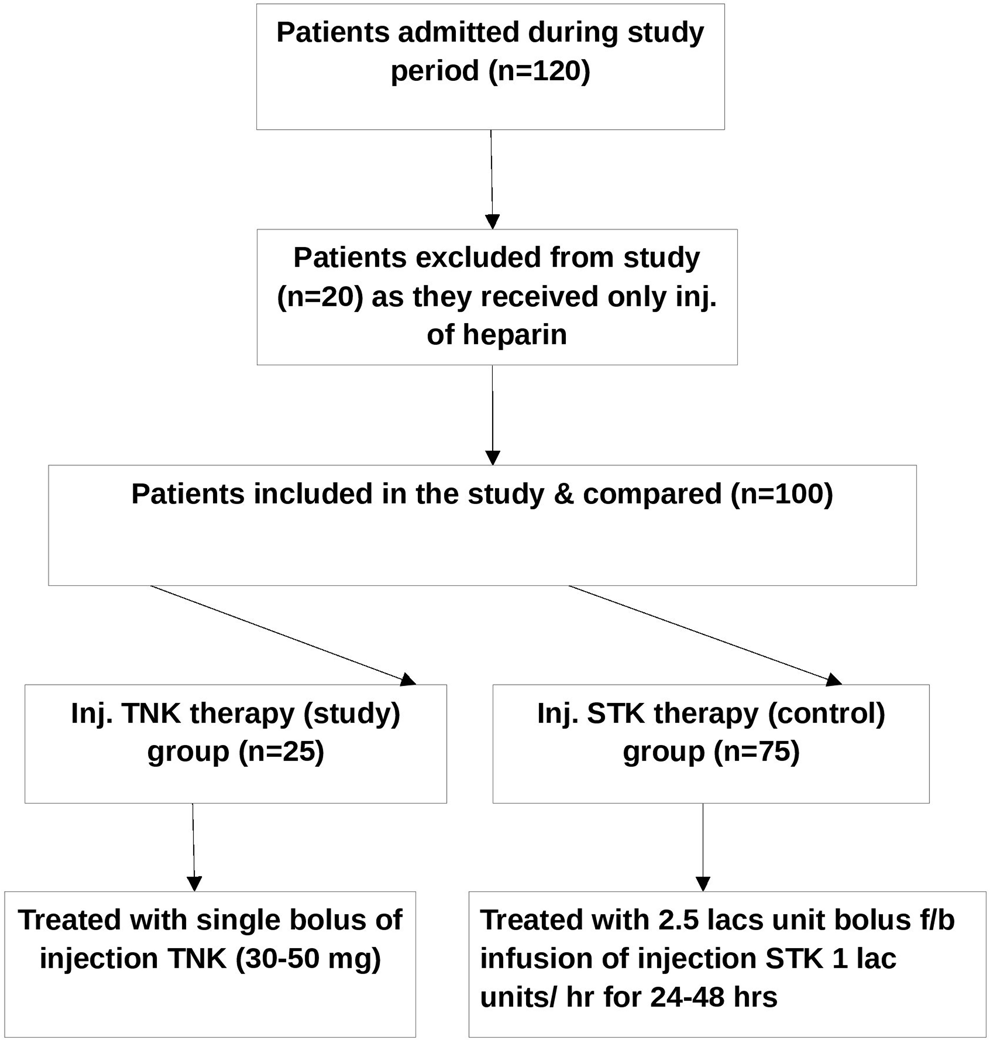
Flowchart of study patients.
Treatment of Control Patient
Streptokinase was given as 250 000 units of intravenous bolus followed by 100 000 units/h infusion maximum up to 24 to 48 hours according to the reduction in PASP and was decided by consultants of treating unit. Unfractionated heparin and VKA were also given similar to the study group (Figure 1).
Outcomes
In this study, the outcome was to determine the improvement in RVD and/or reduction in PASP observed in echocardiography performed 24 hours after treatment, given as used in previous study. 10
Treatment Complication
This was as follows: (1) composite of death from any cause or hemodynamic collapse within 7 days of treatment, (2) hemodynamic collapse is defined as at least 1 of the following: (i) the need for cardiopulmonary resuscitation; (ii) SBP <90 mm Hg for at least 15 minutes, or drop of SBP by at least 40 mm Hg for at least 15 minutes, with signs of end-organ hypoperfusion (cold extremities or urinary output <30 mL/h or mental confusion); (iii) the need for catecholamines (except for dopamine at a rate of <5 μg/kg/min) to maintain adequate organ perfusion and a SBP of >90 mm Hg, (3) clinical deterioration requiring escalation of treatment within 7 days or before discharge (whichever came first), (4) ischemic or hemorrhagic stroke within 7 days, (5) bleeding (ie, mild, moderate, or severe) within 7 days, and (6) any serious adverse events within 7 days. Mild bleeding defined as a bleeding not requiring blood transfusion. Moderate bleeding is defined as a bleeding episode requiring blood transfusions but one that is not considered life-threatening and does not lead to hemodynamic compromise requiring emergency fluid replacement, inotropic support, or interventional/surgical treatment. Severe bleeding is defined as an episode that leads to hemodynamic compromise requiring emergency intervention (as administration of fluids and/or blood products, inotropic support, or surgical treatment) or is life-threatening or fatal. 13
Statistics
All the data were compiled at the end of the study, and the sample was analyzed with chi-square test. The P value of <.05 will be considered as statistically significant.
Results
A total 120 consecutive patients with APE were admitted within the study period. Among them 20 patients were excluded as they did not have either echocardiographic evidence of RVD or received only injection heparin. Finally 100 patients were included in this study. Those patients who had both CTPA proved APE and echocardiographic evidence of RVD were treated with thrombolytic therapy after considering contraindication. They had received either TNK or STK per their financial affordability. In all, 25 patients, who received TNK, were considered as study group and the rest 65 patients, who received STK, were considered as control group. As it was the first study of this kind, the study sample was calculated based on similar type of previous study on APE. 14 The data were collected and analyzed, and conclusion was made.
The mean age of the patients in TNK group (37 ± 12.6 years, with the range of 28-65 years) was lesser than the patients in STK group (39 ± 13 years, with the range of 20-76 years), although the result was not significant (NS). Both the groups have more number of male patients than female. Of our study populations, 56% were below 40 years of age.
Deep vein thrombosis (DVT) was the most common risk factor and comorbid condition associated with PE in our patients with 46% of prevalence, which was followed by smoking (35%) and dyslipidemia/obesity (23%). Of the study patients, 33% have no apparent risk factors for APE. Two patients in STK group were incidentally diagnosed as having human immunodeficiency virus infection. In all, 2 patients in the TNK group had lower limb fracture, and 9 patients in STK group have other risk factors like seizure disorder on anti epileptics, lower limb fracture, hypothyroidism, rheumatic heart disease, and alcoholism.
Mean duration of symptoms at presentation was also less in TNK group (4 ± 2 days, with the range of 2-5 days) than in the STK group (6 ± 4.4 days, with the range of 1-15) of patients, although this result was statistically insignificant. Most common symptom at presentation was dyspnea as 95% of our patients had dyspnea at presentation followed by chest pain (39%) and syncope (9%). At presentation, 9 patients in the STK group had other symptoms like cough, hemoptysis, and easy fatigability. Most common clinical sign was tachycardia and tachypnea in about 89% of the patients. Hypotension was seen in 57% of the patients, and rest had normal BP. Mean saturation of oxygen (Sp
Among the blood investigations,
Among the ECG features suggestive of APE, sinus tachycardia was common with prevalence of 89% followed by S1Q3T3 pattern (65%), RBBB pattern (63%), “T” wave inversion in the mid-precordial lead (56%), and right axis deviation/RVH with strain pattern was seen in 23% of patients.
Echocardiographic features of RVD were seen in all patients. Pulmonary artery systolic pressure at baseline was also comparable between the study groups. Six patients in STK group had visible clot in right atrium, RV, or PA. But all the baseline characteristics had similar distribution in both the groups without any statistical significant differences (Table 1).
Baseline Demographic, Clinical, Investigational, and Echocardiographic Profile in TNK and STK Groups.
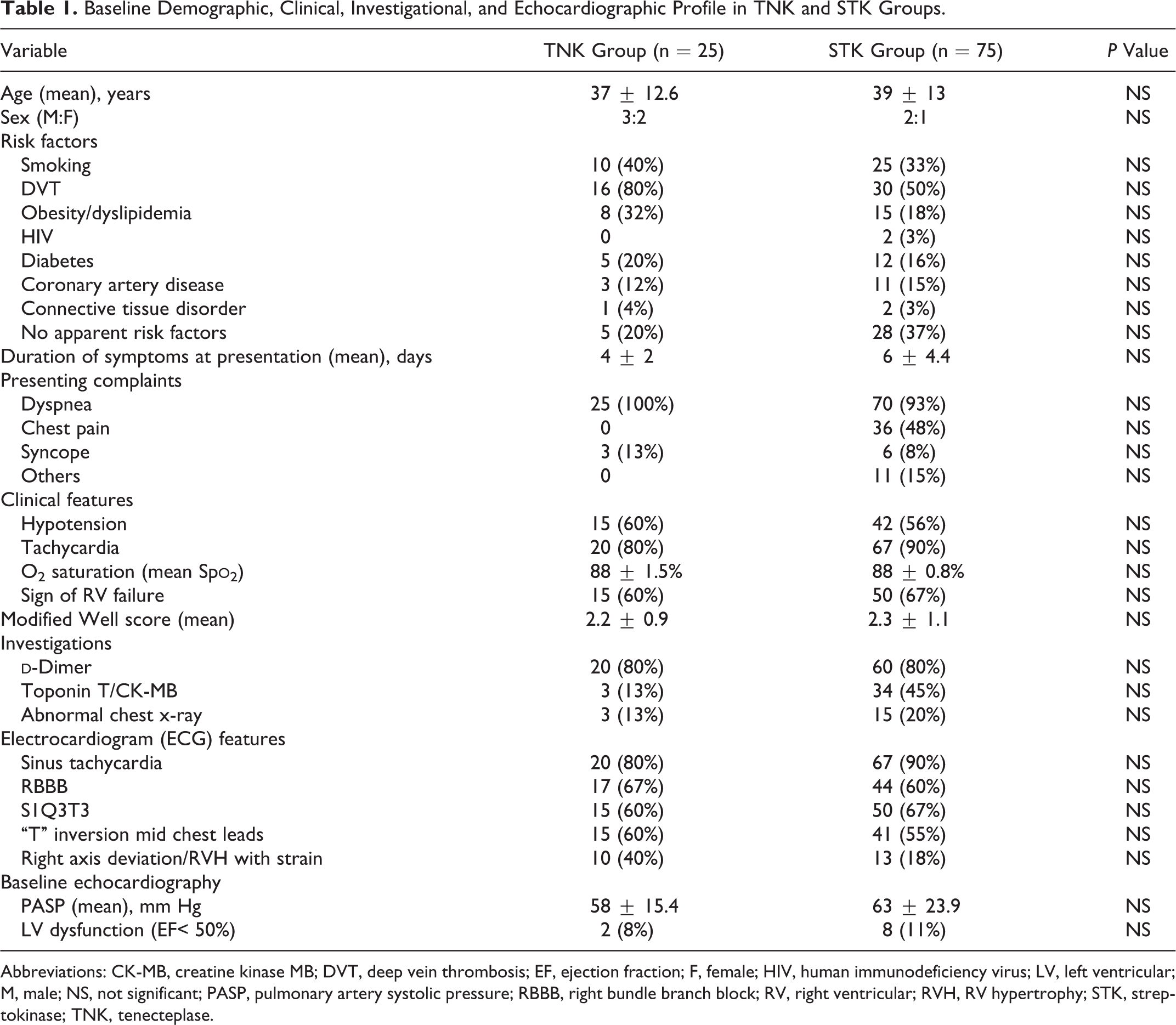
Abbreviations: CK-MB, creatine kinase MB; DVT, deep vein thrombosis; EF, ejection fraction; F, female; HIV, human immunodeficiency virus; LV, left ventricular; M, male; NS, not significant; PASP, pulmonary artery systolic pressure; RBBB, right bundle branch block; RV, right ventricular; RVH, RV hypertrophy; STK, streptokinase; TNK, tenecteplase.
We had taken variables like decrease in mean heart rate, improvement in mean Sp
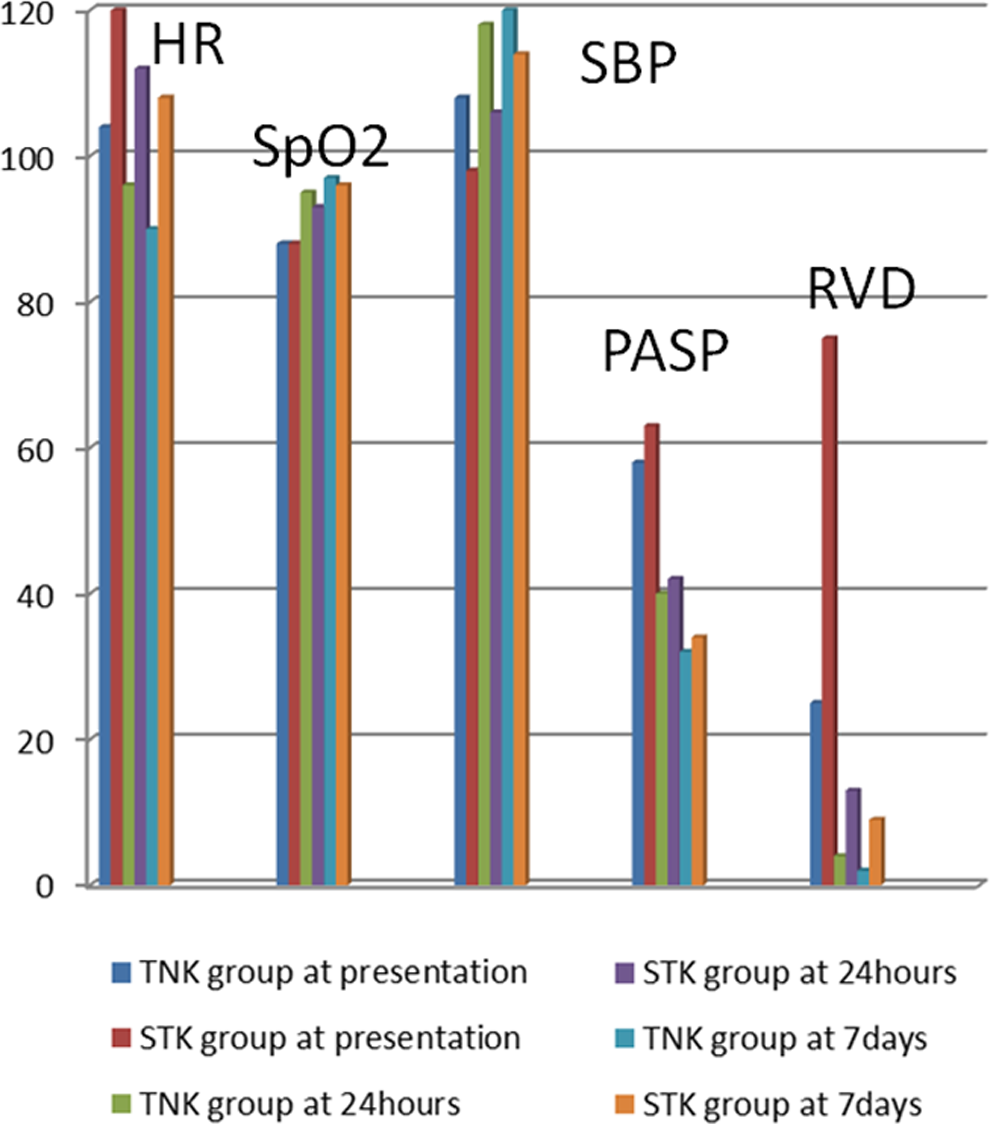
Parameters for assessment for clinical course after therapy.
Clinical Course After Therapy (Figure 2).
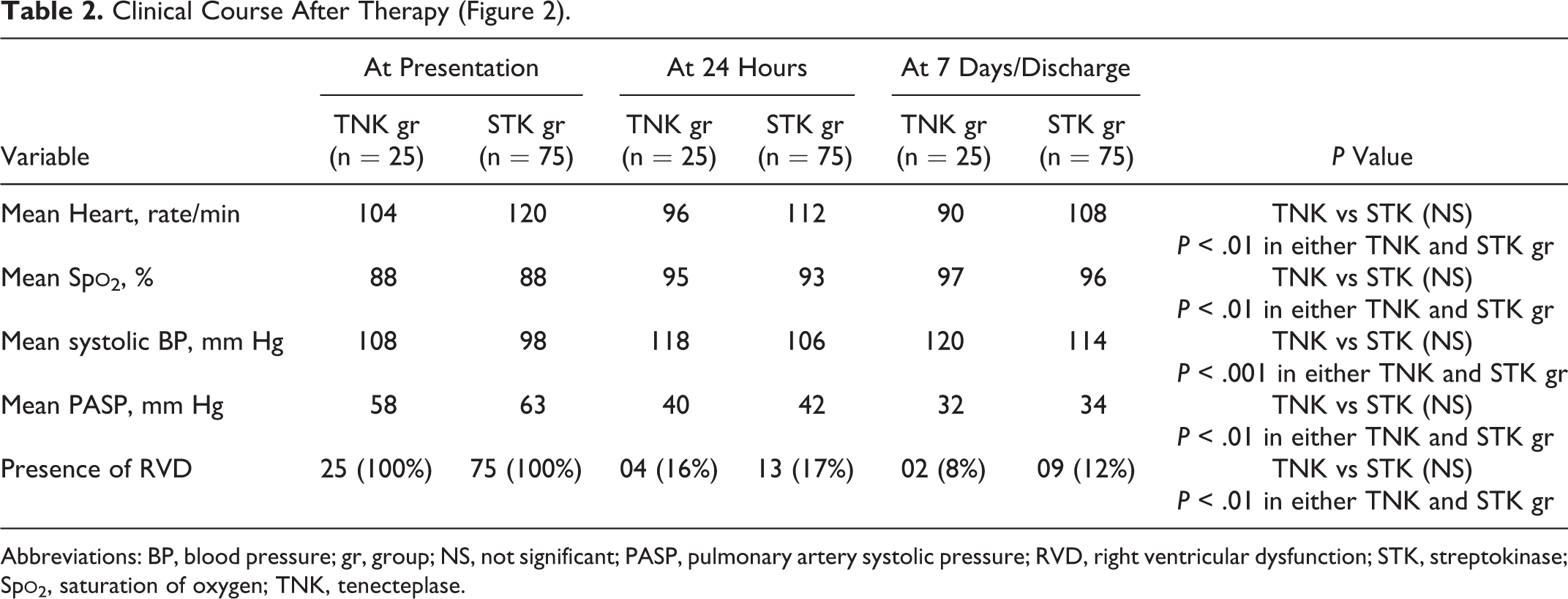
Abbreviations: BP, blood pressure; gr, group; NS, not significant; PASP, pulmonary artery systolic pressure; RVD, right ventricular dysfunction; STK, streptokinase; Sp
When we compare the effect of thrombolysis on PASP in patients with RVD and normal BP (hemodynamically stable) and patients with RVD and hypotension (hemodynamically unstable), we found that both the group of patients had significant improvement in RVD or decreased in PASP from the baseline. So, thrombolysis was helpful in reducing PASP in patients with hemodynamically stable as well as those who are hemodynamically unstable (Table 3; Figure 3). As in our study, complications rates are very less, so we could not find any significant differences in the adverse event between those who were hemodynamically unstable and those who were stable hemodynamically after APE.
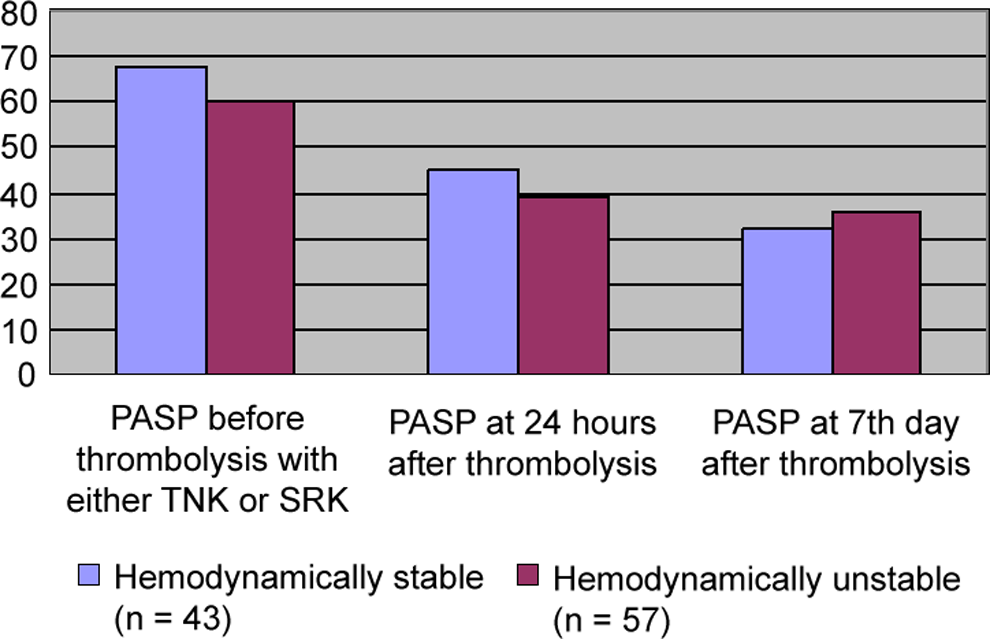
Effect of thrombolysis on pulmonary artery systolic pressure (PASP) in hemodynamically stable patients compared with hemodynamically unstable patients.
Effect of Thrombolysis on PASP in Patients With RV Dysfunction and Normal Blood Pressure (Hemodynamically Stable) and Patients With RV Dysfunction and Hypotension (Hemodynamically Unstable; Figure 3).

Abbreviations: PASP, pulmonary artery systolic pressure; RV, right ventricular; STK, streptokinase; TNK, tenecteplase.
In all, 2 (4%) patients in TNK group died after therapy, whereas 6 (8%) patients died in the STK group (P = NS). All of them had severe RVD, and 1 of them had sudden cardiac death during hospital stay. Hemodynamic deterioration was seen after therapy in 24% of the patients. Minor bleeding was seen in 16% of our study patients. About 11% of patients had other complication like renal dysfunction. But there were no statistically significant differences seen among the 2 groups of patients. One patient in the STK group had stroke due to intracranial bleeding, and another patient had major upper gastrointestinal bleeding. Mean duration of stay in intensive care unit (ICU) was less in the TNK group (2.2 ± 0.8 days) than in the STK group (3.2 ± 1.3 days), and this result was statistically (P = .04) significant (Table 4).
Complication After Therapy, Duration of Intensive Care Unit Stay, and Cost of Treatment in Study Groups.
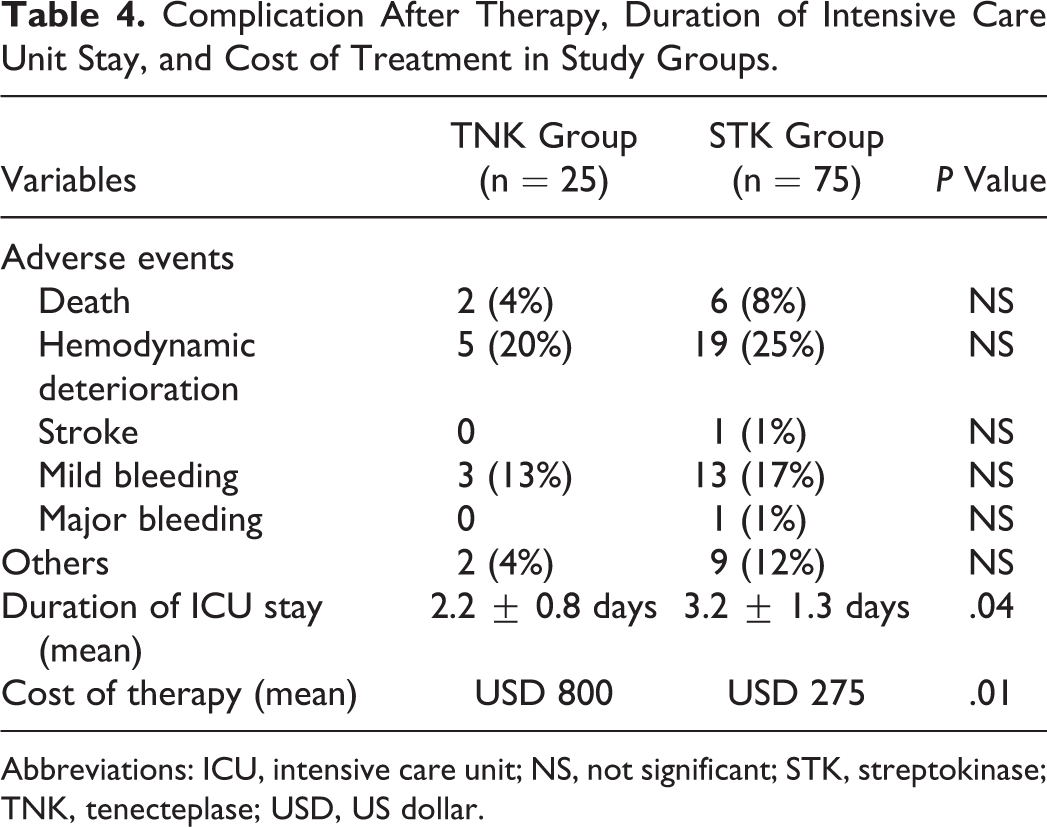
Abbreviations: ICU, intensive care unit; NS, not significant; STK, streptokinase; TNK, tenecteplase; USD, US dollar.
Discussion
Thrombolysis is now the current standard of therapy in patients with APE who presented with hypotension and RVD. 15 So far, TNK is not approved by US FDA for the management of APE. 15 There is no study in the literature where TNK has been compared with STK for the management of both massive and submassive APE, especially in the resource poor countries. The first use of STK in APE was reported in 1964, 16 whereas first report of using TNK in APE was in 2002. 11 This is the first clinical study to compare the safety and efficacy of TNK and STK in patients with APE.
This study showed that APE has a prevalence of 56% those aged below 40 years. This observation was different from previous studies. 9 Deep vein thrombosis was the most common risk factor and comorbid condition in our patients with 46% of prevalence which was similar to the previous studies and was followed by smoking (35%) and dyslipidemia/obesity (23%). 17 It was also unusual in our study that about one-third (33%) of our patients with APE has no apparent risk factors though we could not have thrombotic workup in all these patients due to their poor socioeconomic profile. Clinical profile of our patients was similar to previous studies. 14 Of our patients, 33% were hemodynamically stable with normal BP (SBP >90 mm Hg). As all of our study patients had echocardiographic features of RVD, all of them had received thrombolytic therapy. The ECG findings were also similar to previous study on APE except that our study had more number of patients with the presence of typical S1Q3T3 pattern. 12
Thrombolytic efficacy that was determined by reduction in RVD or PASP as our primary outcome was significantly reduced at 24 hours and at seventh day after treatment from the baseline in both the TNK and the STK group separately (P < .01), but within these 2 groups, there was no significant variation seen in both the reduction of PASP and the resolution of RVD. Along with PASP, there was statistically significant reduction in mean heart rate, improvement in mean Sp
Although we did not find any statistically significant differences in the outcome or adverse effects among the 2 groups of patients and between patients with normotension and hypotension PE, there was insignificantly more trend of excess bleeding in the STK group. Previous study showed up to 20% of bleeding complication after thrombolytic therapy, and incidence of major bleeding was more in alteplase group than in the STK group. 13 In comparison, our study showed less incidence of bleeding (17%) and most of them had minor bleeding only. The reason behind this may be the lesser mean age of our study patients. Mean duration of stay in ICU was less in the TNK group than in the STK group, and this result was statistically significant (P = .04).
Limitation of Study
First, as it was a comparative study, chances of selection bias are more. Second, the study group contains only 25 patients as it was a single-center-based study over a period of 1.5 years, and most of our study patients were from poor economic status so they could not afford TNK therapy. Although the sample size was adequate per the calculation made like in previous study, 13 but due to nonrandomization, the observation of this study should not be generalized and there is a definite need of further double-blinded randomized study with larger sample size. Third, we did not use 2 hours use of STK to compare with bolus of TNK, 13 and fourth, we had used fibrinolytic therapy even in the normotensive APE those who have echocardiographic evidence of RVD, which is so far not indicated as per guidelines. 7 Finally, although this study has about one-third of patients without any risk factor for APE, due to poor financial condition, thrombotic workup was not possible.
Conclusion
Although this was a comparative study with small sample size, it was a first study of this kind and the results from this study must have definite impact on the treatment of both massive and submassive APE in the resource-poor developing country like India. Both TNK and STK can be given to patients with both normotensive and hemodynamically unstable APE with equal efficacy. But in the affordable patient who have more associated risk factors like DVT and presented early after the onset of symptoms, TNK can be prescribed due to its rapidity in the improvement of symptoms and less need of ICU staying and less bleeding risk. Mean age of our study patients was below 40 years, which could be the reason behind the less adverse events in this study, so these results should not be generalized, especially in elderly population. Further, double blinding the study with adequate sample size is needed to compare TNK and STK in the treatment of APE.
1. What is already known?
Thrombolytic therapy is effective in patients with hemodynamically unstable acute pulmonary embolism. Streptokinase is a recommended thrombolytic therapy for it.
2. What is new in this study?
Streptokinase has similar efficacy like tenecteplase. Tenecteplase is costlier but has little less bleeding risk than streptokinase. Thrombolytic therapy has role in patients with normotension having acute pulmonary embolism.
Footnotes
Authors’ Note
Soumya Patra and C. M. Nagesh planned the study. Soumya Patra designed the protocol, collected, and analyzed the data, reviewed the literatures, and drafted the article. Babu Reddy, B. C. Srinivas, Navin Agrawal, and C. N. Manjunath were involved in the management of the patients. Madhav Hegde was involved in doing computed tomography scan of all patients. All authors approved the final version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.