
Abstract
We present a 15-week pregnant woman who developed mechanical mitral valve thrombosis on a fixed dose of enoxaparin therapy 60 mg twice daily. No reductions were observed in the thrombus size or mean mitral gradient on transesophageal echocardiography (TEE) with 1 week of unfractioned heparin therapy. As the thrombus on TEE imaging was hypermobile and fragile, in addition to a higher dose of enoxaparin (80 mg twice daily), trofiban infusion 0.20 µg/kg per minute was administered for another 1 week. The thrombus on the valve was reduced in size, mobility and fragility of the thrombus diminished, and mean valve gradient decreased on TEE. As complete thrombus resolution was not observed and limitation of valve mobility continued, tissue plasminogen activator (tPA) was given to the patient. A complete thrombus resolution was observed on this therapy. The patient is presented for being the first case in literature whose valvular thrombus reduced with trofiban therapy.
Introduction
Pregnant women with a mechanical prosthetic valve have a hypercoagulable condition, and this condition significantly increases the thromboembolic risk. 1 Thromboembolic complication rate in patients using warfarin throughout pregnancy is 3.9%, and in pregnant women using unfractioned heparin (UH) during the first trimester continuing with warfarin is 9.2%. Maternal mortality rates with these regimens were reported to be 1.8% and 4.2%, respectively. 2 Necessity for optimal anticoagulant therapy should be considered as well as the adverse effects of anticoagulation on fetus. The guidelines recommend warfarin to be used until 36 gestational weeks except between weeks 6 and 12. Warfarin therapy 5 mg or less daily minimizes valvular thrombosis risk without fetal malformation risk. Although warfarin protects the mother from thromboembolic complications, it may cause embryopathy, prematurity, and abortion. With UH use, there is no embryopathy risk, whereas maternal thromboembolic complications can be seen more frequently. 3 Low-molecular weight heparins (LMWHs) have no embryopathy risk as they do not cross the placenta. Stable nonpregnancy coagulation is provided more easily with LMWH compared to UH. 4 For pregnant women who develop mitral valve thrombosis, there are options of fibrinolytic therapy, surgical treatment, and anticoagulant therapy according to the patient’s hemodynamic status. Glycoprotein IIb/IIIa antagonists serve as very strong inhibitors of platelet function by blocking the last stage of platelet aggregation. 5 For the first time in literature, trofiban from this group was used in a pregnant woman with prosthetic valvular thrombosis and provided a decrease in the mobility, fragility, and the size of the thrombus. Thereafter, a complete thrombus resolution was achieved by administrating tissue plasminogen activator (tPA) infusion.
Case Report
In a 29-year-old, 80-kg woman with a metallic mitral prosthetic valve implanted in 1997, warfarin was stopped when her pregnancy was identified, and a fixed dose of enoxaparin 60 mg twice daily was started. This was her first pregnancy. At week 11 of her gestation, she was hospitalized by the neurology clinic for sudden loss of strength on her left arm. The patient was admitted to our clinic at the 15th gestational week with a complaint of an increase in dyspnea after regression of her neurological symptoms. A severe gradient increase was detected on mitral valve on the transthoracic echocardiography (TTE) carried out on the patient for the prediagnosis of prosthetic valvular thrombosis. On transesophageal echocardiography (TEE), a mobile and highly fragile thrombus was seen on one of the leaflets of the mitral valve, which limited the mobility (Figure 1 ). Mean mitral valve gradient was 33 mm Hg, and a grade 3 echocontrast at left atrium and severe tricuspid regurgitation were detected. The patient was started on UH and acetylsalicylic acid 100 mg under close activated partial thromboplastin time (aPTT) monitoring. No clinical improvement was observed in the patient who was monitored for 1 week at 2 to 3 times the normal aPTT levels. As there was no reduction in the thrombus size, and no decrease in mean mitral valve gradient on serial TEE imaging, UH was replaced with enoxaparin 80 mg twice daily, and in addition, trofiban 0.20 µg/kg per minute infusion was started. On TEE imaging performed 24 hours later, it was observed that the thrombus was reduced in size by 50%, its fragility and mobility diminished, and mean mitral valve gradient decreased to 12 mm Hg (Figure 2 ). Clinical findings of the patient improved. On TEE performed following 1 week of trofiban infusion, there was no further regression in the thrombus, high mean valvular gradient remained, and limitation of valvular mobility continued because of an organized thrombus on 1 leaflet. The patient was informed about the risks of surgical procedure and thrombolytic therapy. As the patient refused surgical treatment, a 4-hour infusion of tPA 25 mg was administered for 3 times. Consequent TEE showed that the thrombus completely disappeared (Figure 3 ). No maternal or fetal complications occurred. Warfarin was then started, and international normalized ratio (INR) was adjusted to >2.5. The patient was discharged on acetylsalicylic acid 100 mg and warfarin therapy. At her control visits, valvular gradient on TTE was found to be normal and her pregnancy was going on in a healthy manner.

Thrombus completely limiting 1 of the leaflets of the mitral valve, which limited the mobility. LA indicates left atrium.
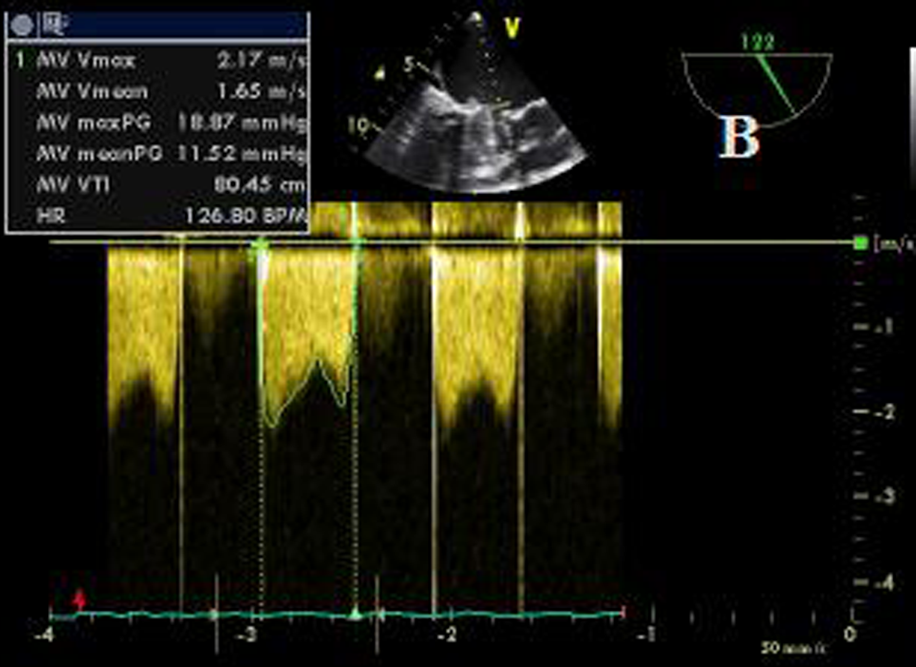
Mitral valve gradient after trofiban therapy.
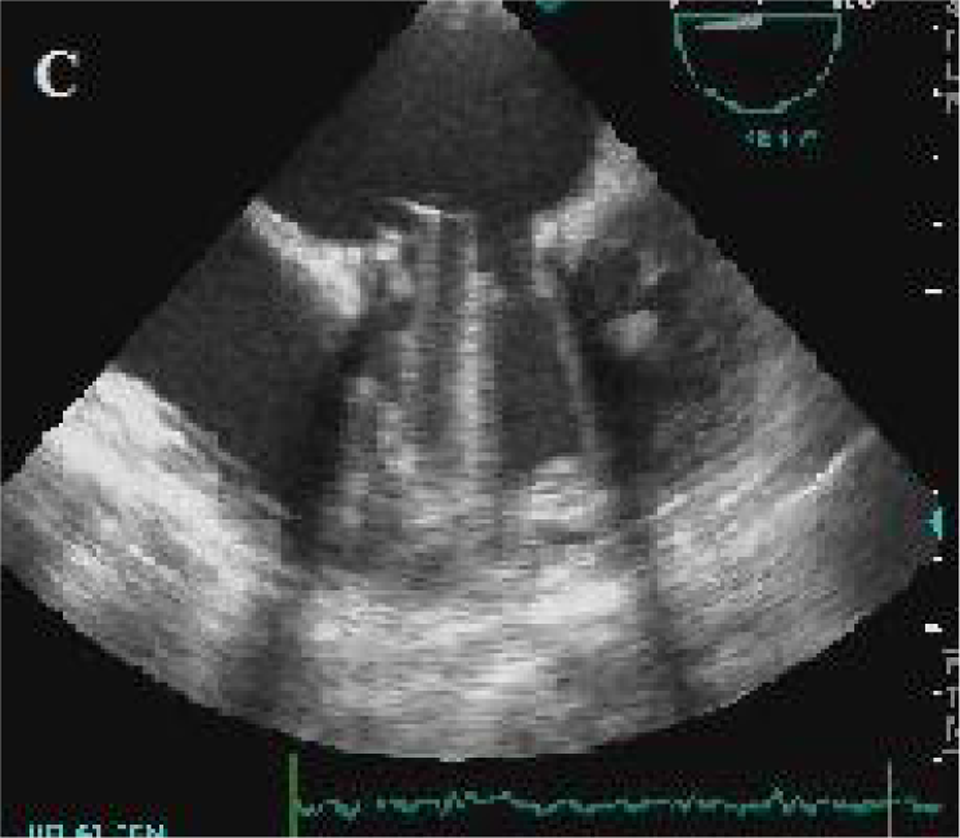
Complete resolution of the thrombus after tPA. tPA indicates tissue plasminogen activator.
Discussion
Increased mitral prosthetic valvular thrombosis during pregnancy is linked to increased plasma levels of fibrinogen, factor VII, factor VIII, factor X, and plasminogen activator inhibitor. In addition, an increase in platelet adhesion facilitates the situation. Also, uterine compression on inferior vena cava at supine position and activated protein C resistance during pregnancy result in slow venous blood flow in the legs, leading to hypercoagulability. 6 Although oral anticoagulants are the most effective medications in preventing prosthetic valvular thrombosis, they have the highest fetal damage risk. Low-molecular weight heparins have less fetal damage risk and provide adequate anti-Xa levels, but they provide less effective anticoagulation. Unfractioned heparin is only recommended during hospitalization, although it provides effective anticoagulation and has no fetal damage risk. 2 Abilgaard and colleagues reported in their study that thromboembolic complication risk was 7.1% with the use of LMWH throughout the pregnancy, 3.6% in the group that used LMWH only at the first trimester and continued with warfarin during the last 2 trimesters, and 2.4% in the group that used warfarin during whole pregnancy. 7 As warfarin has a high teratogenicity and abortion risk at the first trimester, it is recommended for very high–risk pregnant women with thromboembolic complication risk. Low-molecular weight heparin is the first-line option for anticoagulation at this period. In a review that evaluated 81 pregnant women with prosthetic valves, 9 of 30 pregnant women receiving a fixed dose of LMWH developed thromboembolic complications, whereas only 1 of 51 pregnant women using LMWH adjusted according to the anti-Xa level developed thromboembolic complication. 8 With the recommended dose, peak anti-Xa level measured 4 hours after the last dose should be 0.7 to 1.2 U/mL. If basal level is at subtherapeutic level after achieving the therapeutic peak level, the dose should be administered 3 times daily. 4 In another study with dalteparin and enoxaparin, the therapy was started with dalteparin 100 U/kg and enoxaparin 1 mg/kg, and the doses were titrated so that the target anti-Xa level would be 1.0 to 1.2 IU/mL. In only 1 of 12 pregnant women, nonfatal prosthetic valvular thrombosis was observed because of subtherapeutic anti-Xa level, and 3 had major hemorrhage. On average, 54.4% increase was observed in the prenatal dose compared to the initial dose. 9 In our patient, a fixed dose of enoxaparin, a lower dose for her body weight, was started and the dose was not adjusted according to anti-Xa level. We related mechanical valvular thrombosis in this patient to failure of the dose to provide adequate anticoagulation. When mechanical valvular thrombosis develops in pregnancy, risk of cardiac surgery for the mother is similar to that of nonpregnant women. However, fetal mortality risk associated with cardiopulmonary bypass is 20% to 30%. 10,11 As our patient’s clinical condition did not deteriorate and as this was her first pregnancy, surgical treatment was not intended, considering fetal-loss rate. When surgical treatment is mandatory in the patient, fetal mortality is reported to be low at mild hypothermia, high perfusion pressure, and in a short cardiopulmonary bypass period. As uterine contractions during surgery is a predictor of fetal mortality, continuously monitoring uterine contractions along with fetal heart rate is definitely recommended during surgery. 12,13 Although there is very limited data, it was shown that fibrinolytic therapy could be successfully used without any negative effect on the fetus. 14 Compared to surgery, fibrinolysis should be considered as a safer approach for many pregnant patients. When fibrinolytic therapy is administered, TTE is recommended to observe thrombus resolution once every 3 hours. Transesophageal echocardiography should be performed 24 hours later, and if necessary, should be repeated at 48 and 72 hours. 15 Weight-adjusted LMWH was given and trofiban was added to our patient who had had no clinical improvement and no thrombus resolution on TEE with UH therapy. Because mobility and fragility of the thrombus were excessive, we aimed to decrease the complication rate of subsequent therapies by even partially reducing the condition with trofiban. As vaginal hemorrhage and presence of pregnancy are relative contraindications, we did not administer fibrinolytic therapy at that stage. An improvement was observed in the clinical findings of the patient. Transesophageal echocardiographic image at 24 hours showed that mobility and fragility of the thrombus diminished, the thrombus resolved by 50%, and mean valvular gradient decreased. On TEE performed 1 week after trofiban infusion, it was seen that the thrombus was localized on 1 leaflet and remained in an organized form, and there was no more reduction in the mean valvular gradient. In literature, some small-sized trials reported similar success rates with abciximab, a platelet glycoprotein IIb/IIIa inhibitor. 16 As no complete resolution was observed and mobility limitation at the valve remained with trofiban, the patient was informed about the risks of surgical and thrombolytic treatments. Tissue plasminogen activator was given to the patient who refused surgical treatment. In literature, success rate with weight-adjusted bolus tPA is 85% to 93%. In addition to general complications of fibrinolysis, there is the risk of uterine hematoma for pregnant women. 17 –19 In our patient, we observed a complete resolution without any complication after tPA.
After addition of trofiban to LMWH, the thrombus remained localized on 1 leaflet. Moreover, the thrombus reduced 50% in size, and mean mitral valve gradient was significantly decreased. Such reduction shown in the patient with severe obstructive prosthetic valvular thrombus may be an alternative to fibrinolytic therapy in nonobstructive prosthetic valvular thrombi or in conditions that are obstructive but the thrombus load is lower. However, data on dose and length of use are yet inadequate. Case reports and clinical trials that will be carried out in the future will determine clinical practice of this therapy, which puts lives of both mother and fetus at lower risk compared to surgical or fibrinolytic therapy.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.