
Abstract
Background
Microvascular reperfusion strongly influences prognosis after ST-elevation myocardial infarction (STEMI). While invasive indices are established, practical non-invasive biomarkers remain limited. This study evaluated whether coagulation markers correlate with myocardial blush grade (MBG)—an angiographic surrogate of tissue-level reperfusion—and could serve as non-invasive indicators of microvascular reperfusion.
Methods
In this single-center case-based study, 48 consecutive STEMI patients undergoing coronary angiography were enrolled. MBG was assessed by an experienced interventional cardiologist blinded to laboratory data. Blood was sampled after reperfusion for tissue plasminogen activator/plasminogen activator inhibitor-1 complex (tPA/PAI), prothrombin fragment 1 + 2 (F1 + 2), thrombin-antithrombin complex, and D-dimer. Associations between biomarkers and MBG (0-1 vs 2-3) were examined. Receiver operating characteristic (ROC) analysis determined cut-offs; multivariable models evaluated independence.
Results
Mean age was 61.2 ± 11.8 years; 87.5% were male. Comorbidities included hypertension (47.9%) and hyperlipidemia (33.3%). MBG distribution was: MBG 3 (33.3%), MBG 1 (25.0%), MBG 0 (22.9%), MBG 2 (18.8%). Patients with MBG 0–1 had significantly higher tPA/PAI and F1 + 2 than those with MBG 2–3 (p = .003 and p < .001, respectively). Admission troponin and CK-MB were also higher in MBG 0–1 (p = .049 and p = .026). ROC analysis showed tPA/PAI < 9.4 μg/dL predicted MBG 2–3 (AUC = 0.752; 95% CI 0.606-0.865; sensitivity 72.0%, specificity 69.57%), and F1 + 2 ≤ 14 580 pmol/L predicted MBG 2–3 (AUC = 0.973; 95% CI 0.880-0.999; p < .001). Lower admission troponin and CK-MB also predicted MBG 2–3. In multivariable analysis, no biomarker remained independently associated with MBG.
Conclusions
Lower post-reperfusion tPA/PAI and F1 + 2 levels are associated with higher MBG (better microvascular reperfusion) in STEMI. Although not independently predictive, these readily measurable markers—particularly tPA/PAI—may complement reperfusion assessment when direct angiographic evaluation is unavailable. Larger, multicenter studies with standardized sampling are warranted to validate cut-offs and clinical utility.
Introduction
Although primary percutaneous intervention (PCI), the gold standard for ST-elevation myocardial infarction (STEMI), is the primary treatment, many patients do not receive it due to economic, geographic, and patient-specific factors. 1 Fibrinolytic therapy or rescue PCI in cases where fibrinolytic therapy is contraindicated are potential beneficial strategies supported by numerous studies.2,3
Although the benefit of pharmacoinvasive therapy has been confirmed, indirect indicators such as pain reduction, electrocardiographic, and echocardiographic findings are still used as evidence of reperfusion in fibrinolytic therapy. 4 Even though reperfusion is a key endpoint for patient prognosis regarding early mortality, microvascular reperfusion, and thrombus burden are crucial for predicting mortality and left ventricular recovery. 5 In terms of either invasive or pharmacoinvasive therapy, the absence of a biomarker that can directly measure reperfusion is noteworthy.
The present study aimed to detect potential surrogate markers of thrombus burden, reperfusion, and microvascular reperfusion.
Primary percutaneous coronary intervention (PCI) is the preferred reperfusion strategy in patients with ST-elevation myocardial infarction (STEMI) and has been shown to reduce mortality and improve clinical outcomes.1,2 Nevertheless, despite successful restoration of epicardial coronary flow, a substantial proportion of patients experience inadequate myocardial tissue reperfusion due to microvascular obstruction, distal embolization, or persistent thrombotic burden. Impaired microvascular reperfusion is a major determinant of infarct size, left ventricular remodeling, and long-term prognosis. 3
Reperfusion assessment has traditionally relied on angiographic, electrocardiographic, and imaging-based parameters. Angiographic indices such as Thrombolysis in Myocardial Infarction (TIMI) flow grade and myocardial blush grade (MBG) directly reflect epicardial and tissue-level perfusion, respectively, but they are invasive, operator-dependent, and not universally available, particularly in patients treated with fibrinolytic therapy or in non-interventional centers.3,4 Electrocardiographic markers, including ST-segment resolution, and early echocardiographic findings provide indirect information regarding reperfusion but have limited sensitivity and specificity for evaluating microvascular perfusion. 2 Consequently, there remains a need for practical, non-invasive biomarkers that can reflect myocardial reperfusion at the microvascular level.
Cardiac troponins are the most widely used biomarkers in acute myocardial infarction and have been proposed as indirect indicators of reperfusion based on their release kinetics.5,6 However, troponin levels primarily reflect myocardial necrosis rather than tissue-level perfusion and may be influenced by a variety of non-coronary conditions, including renal dysfunction, heart failure, and systemic inflammatory states. 7 These limitations have prompted interest in alternative biomarkers that more directly reflect thrombotic activity and fibrinolysis during acute coronary occlusion and reperfusion.
Coagulation and fibrinolytic pathways play a central role in coronary thrombus formation and resolution in STEMI. Prothrombin fragment 1 + 2 (F1 + 2) reflects in vivo thrombin generation and hypercoagulability. 8 The thrombin–antithrombin (TAT) complex indicates activation of the coagulation cascade and has been associated with thrombotic conditions in both arterial and venous systems.9,10 Beta-thromboglobulin is released during platelet activation and serves as a marker of platelet involvement in coronary thrombosis. 11 The fibrinolytic system is primarily regulated by tissue plasminogen activator (tPA) and its main inhibitor, plasminogen activator inhibitor-1 (PAI-1). The circulating tPA/PAI-1 complex reflects the balance between fibrinolysis and its inhibition and has been linked to impaired fibrinolytic activity and adverse cardiovascular outcomes.12–14 Elevated levels may indicate ineffective thrombus resolution and persistent microvascular obstruction despite epicardial reperfusion. D-dimer reflects fibrin degradation and ongoing thrombus turnover but lacks specificity in the acute coronary setting due to its elevation in inflammatory and other prothrombotic conditions.15
Despite the biological relevance of these biomarkers, their relationship with direct angiographic indicators of microvascular reperfusion, particularly myocardial blush grade, remains unclear. Establishing such an association may help determine whether readily measurable coagulation-related biomarkers can serve as non-invasive surrogates of tissue-level reperfusion.
Therefore, this study aimed to investigate the association between selected coagulation and fibrinolytic biomarkers (tPA/PAI-1 complex, prothrombin fragment 1 + 2, thrombin–antithrombin complex, beta-thromboglobulin, and D-dimer) and myocardial blush grade in patients with STEMI. We hypothesized that biomarkers reflecting impaired fibrinolysis and increased thrombin generation would be associated with lower MBG, indicating suboptimal microvascular reperfusion.
Materials and Methods
Study Population
The study was approved by the local ethics committee at Baskent University, and written informed consent was obtained from each participant (KA14/308). A total of 48 STEMI patients who were admitted to the Baskent University Emergency Department between April 2014 and June 2016 was included. All patients underwent percutaneous coronary interventions, which were performed by an experienced invasive cardiologist. Blood samples were collected after reperfusion. Patients who refused to participate in the study, declined to undergo coronary angiography, or were not scheduled for coronary angiography, as well as those with over 120 min in door-to-balloon time, were excluded. Additionally, patients with severe hematological, hepatic, renal, or infectious diseases with inherently elevated (≥2.0) international normalized ratio (INR), low thrombocyte count (< 50.000/mm3), other severe bleeding diatheses, or signs and symptoms of disseminated intravascular coagulation (DIC) were excluded. Patients on oral anticoagulants such as coumarin derivatives or novel oral anticoagulants, including dabigatran, apixaban, rivaroxaban, or edoxaban, were also excluded. Although ethical approval was obtained in October 2013, patient recruitment was extended due to the acute nature of STEMI, strict exclusion criteria, and a considerable proportion of eligible patients declining participation.
Coronary Angiographic Evaluation
All patients underwent coronary angiography performed by experienced cardiologists, and all angiographic examinations were carried out using a Siemens ARTIS ZEE (Serial no: 137236). All patients received guideline-directed antithrombotic therapy, including dual antiplatelet treatment and intravenous unfractionated heparin during primary PCI, according to current STEMI management guidelines. Each patient first underwent a comprehensive coronary angiography with all standard positions and a 30 frames-per-second sequence. The myocardial blush grade (Table 1: Definition of MBG grades) was evaluated from the database by an interventional cardiologist with 10 years of experience who was blinded to the results of other study tests.
Definition of MBG Grades.

Blood Sampling and Biomarker Assays
All blood samples were collected from the femoral artery after successful reperfusion. Blood samples were allowed to clot at room temperature for 20 min prior to centrifugation. Following centrifugation at 4000 rpm, serum samples were stored at −80 °C until biochemical analysis. Hemolyzed samples were excluded from the analysis.
The following commercially available enzyme-linked immunosorbent assay (ELISA) kits were used for biomarker measurements: Human Beta-Thromboglobulin ELISA kit, Human Prothrombin Fragment 1 + 2 ELISA kit, Human Thrombin–Antithrombin Complex ELISA kit, Human PAI-1/tPA Complex ELISA kit, and Quantia D-dimer ELISA kit.
Beta-thromboglobulin is a protein stored in platelet alpha granules and released during platelet activation, serving as an indicator of platelet activation. Prothrombin fragment 1 + 2 is generated during the cleavage of prothrombin by activated factor X and reflects in vivo thrombin generation and a prothrombotic state. The thrombin–antithrombin complex is formed when thrombin binds to antithrombin and represents activation of the coagulation cascade.
The tPA/PAI-1 complex is formed by the binding of tissue plasminogen activator (tPA) and plasminogen activator inhibitor type-1 (PAI-1) and reflects the balance between fibrinolysis and its inhibition. D-dimer is produced during plasmin-mediated degradation of cross-linked fibrin and indicates active thrombus formation and fibrinolysis.
All patients were grouped by myocardial blush grade, a marker of reperfusion, and biomarker levels were evaluated independently within each group. Patients were categorized as follows:
Group 1: MBG 0–1 Group 2: MBG 2–3
Statistical Analysis
Descriptive statistics were presented as mean ± standard deviation or median with minimum–maximum values for continuous variables, depending on data distribution. Categorical variables were expressed as numbers and percentages.
Normality of continuous variables was assessed using the Kolmogorov–Smirnov, Shapiro–Wilk, and Anderson–Darling tests. For comparisons between two independent groups, the Independent Samples t-test was applied for normally distributed variables, while the Mann–Whitney U test was used for non-normally distributed variables. For comparisons involving more than two independent groups, the Kruskal–Wallis test was used for non-normally distributed variables, followed by the Dwass–Steel–Critchlow–Fligner test for multiple comparisons.
Differences between categorical variables were evaluated using Pearson's Chi-square test or Fisher's exact test for 2 × 2 tables. For larger contingency tables (RxC), the Fisher–Freeman–Halton test was applied.
Receiver operating characteristic (ROC) curve analysis was performed using the DeLong method, and optimal cut-off values were determined using the Youden index. Area under the curve (AUC) values with corresponding 95% confidence intervals (CI) were calculated. ROC analyses were conducted using MedCalc Statistical Software Trial version (MedCalc Software bvba, Ostend, Belgium; 2015).
All other statistical analyses and graphical representations were performed using Jamovi (Version 1.6.13.0; Jamovi Project, 2020) and JASP (Version 0.14.1.0). A two-sided p value < .05 was considered statistically significant.
An a priori power analysis was conducted using an exact two-tailed test for correlation (H0: ρ = 0), with a significance level of α = 0.05 and a desired power of 80%. Assuming a moderate expected effect size (ρ = .40), the required sample size was calculated as 48 patients. This estimation was considered appropriate given the exploratory nature of the study.
Results
A total of 48 patients undergoing coronary angiography in the acute phase of STEMI were included in the study. The mean age was 61.2 ± 11.8 years, and the majority of patients were male (87.5%). A positive family history was present in 27 patients (57.4%). Hypertension and hyperlipidemia were the most common comorbidities, observed in 47.9% and 33.3% of patients, respectively. Acetylsalicylic acid was the most frequently used medication (32.6%), followed by ACE/ARB therapy (28.3%), beta-blockers (19.6%), and statins (15.2%).
The distribution of myocardial blush grades was as follows: MBG 3 in 33.3%, MBG 1 in 25.0%, MBG 0 in 22.9%, and MBG 2 in 18.8% of patients. Baseline demographic and clinical characteristics are summarized in Table 2. Laboratory parameters of the overall study population are presented in Table 3. Troponin and creatine kinase–MB levels were significantly higher on the first day than at admission (both p < .001).
Baseline Demographic and Clinical Characteristics of the Overall Study Group (n = 48).

† : mean ± standard deviation, ‡: n (%). BMI: body mass index, CABG: coronary artery bypass grafting, AMI: acute myocardial infarction, COPD: chronic obstructive pulmonary disease, ACE: angiotensin-converting enzyme inhibitor, ARB: angiotensin receptor blockers, TIMI: thrombolysis in myocardial infarction, MBG: myocardial blush grade. BMI: body mass index,
Laboratory Parameters of the Study Group.
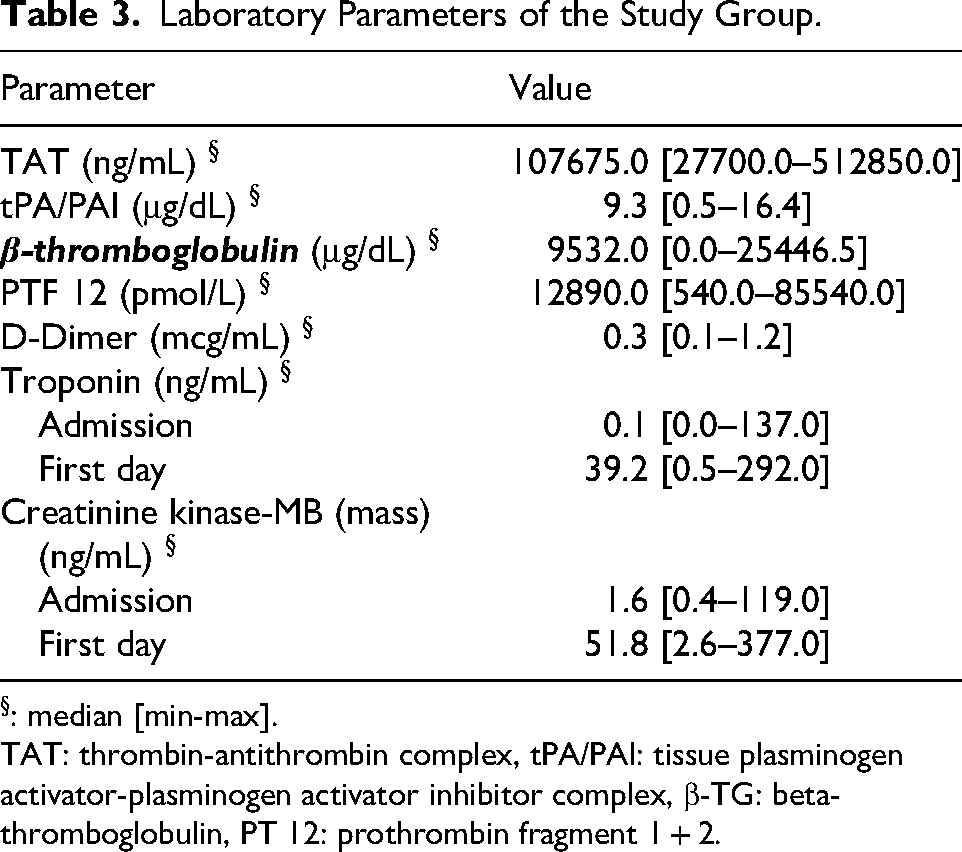
: median [min-max].
TAT: thrombin-antithrombin complex, tPA/PAI: tissue plasminogen activator-plasminogen activator inhibitor complex, β-TG: beta- thromboglobulin, PT 12: prothrombin fragment 1 + 2.
When patients were grouped according to myocardial blush grade (MBG 0-1 vs MBG 2-3), no significant differences were observed in baseline demographic or clinical characteristics (Table 4). Patients with MBG 0–1 had significantly higher levels of tPA/PAI and prothrombin fragment 1–2 compared with those with MBG 2–3 (p = .003 and p < .001, respectively) (Table 5). Admission troponin and creatine kinase–MB levels were also significantly higher in the MBG 0–1 group (p = .049 and p = .026), whereas other laboratory parameters did not differ significantly between groups.
Comparison of the Baseline Demographic and Clinical Characteristics Between the Patients who Were Grouped Based on the MBGs.

: mean ± standard deviation, ‡: n (%).
BMI: body mass index, CABG: coronary artery bypass grafting, AMI: acute myocardail infarction, COPD: chronic obstructive pulmonary disease, ACE: angiotensin converting enzyme inhibitor, ARB: angiotensin receptor blockers, TIMI: thrombolysis in myocardial infarction, MBG: myocardial blush grade.
*. Pearson Chi-Square, Fisher's Exact or Fisher Freeman Halton tests
**. Independent Samples T-Test
Comparison of the Laboratory Parameters Between the Patients who Were Grouped Based on Myocardial Blush Grade.

: median [min-max].
TAT: thrombin-antithrombin complex, tPA/PAI: tissue plasminogen activator plasminogen activator inhibitor complex, β-TG: beta- thromboglobulin, PT 12: prothrombin fragment 1 + 2.
*. Mann-Whitney U test
Clinical details of the post-PCI period, Table 6, and echocardiographic findings are summarized in Table 7.
Clinical Details of the post-PCI Period.

Post-Treatment Echocardiographic Outcomes in the Overall Study Group (n = 48).

: mean ± standard deviation, ‡: n (%), §: median [min-max].
EF: ejection fraction, EDV: end-diastolic volume, ED: end-diastolic
CCB: calcium channel blockers
In ROC analysis, tPA/PAI < 9.4 μg/dL and prothrombin fragment 1–2 ≤ 14,580 pmol/L were significantly associated with MBG 2–3 (Table 8, Figure 1). A tPA/PAI value below 9.4 μg/dL showed a sensitivity of 72.0% and a specificity of 69.6% for identifying MBG 2–3 (AUC = 0.752, 95% CI 0.606-0.865; p = .001). Prothrombin fragment 1–2 demonstrated excellent discriminatory ability (AUC = 0.973, 95% CI 0.880-0.999; p < .001). Lower admission troponin and creatine kinase–MB levels were also associated with MBG 2–3. Other laboratory parameters were not significantly associated with MBG status. Using ROC-derived cut-off values, tPA/PAI ≤ 9.4 μg/dL demonstrated a positive predictive value of 69.2% and a negative predictive value of 68.2% for identifying MBG 2–3, whereas prothrombin fragment 1 + 2 ≤ 14,580 pmol/L showed a PPV of 89.3% and an NPV of 100%.

The receiver operating characteristic curve based on the prediction of MBGs of 2 and 3. (AUC: area under the curve).
ROC Analysis of the Laboratory Parameters in Predicting MBGs of 2 and 3.

: median [min-max].
TAT: thrombin-antithrombin complex, tPA/PAI: tissue plasminogen activator plasminogen activator inhibitor complex, β-TG: beta- thromboglobulin, PTF 12: prothrombin fragment 1 + 2.
In multivariable logistic regression analysis including tPA/PAI, prothrombin fragment 1–2, admission troponin, and creatine kinase–MB, none of the biomarkers remained independently associated with myocardial blush grade.
Discussion
It has long been sought to identify biochemical or electrocardiographic surrogate markers of angiographic myocardial reperfusion in STEMI. Although some of them provide valuable data, they are either insensitive (e.g, ST resolution, echocardiographic LVEF estimation), invasive (TIMI TG, MBG), time-consuming (TIMI TG, MBG), or expensive (TIMI TG, MBG). Besides, although TIMI TG and MBG can be readily assessed from invasive coronary angiogram in early presenters who are eligible for primary percutaneous intervention, patients who present too late, those who pose contraindications for coronary angiography (active bleeding or bleeding diathesis, acute aortic dissection, too many comorbidities or critical condition), or those who present to non-intervening centers, cannot benefit angiographic myocardial reperfusion assessment and heavily depend on electrocardiographic, echocardiographic, or clinical judgment. Thus, at least for patients who cannot undergo coronary angiography and intervention for any reason, biochemical markers, apart from electrocardiographic ones (ST resolution, emergence of idioventricular rhythm, among others), may, in theory, guide physicians regarding how myocardial perfusion is achieved during reperfusion, particularly with fibrinolytic therapy.
Previously, some biomarkers have been used to assess myocardial reperfusion. 16 The most traditional ones are troponins. Since they are highly sensitive to myocardial injury, any increase or decrease in them can indicate myocardial injury and possible reperfusion. 5 Therefore, it has been widely accepted that an early-than-expected peak of troponins is a reliable sign of the opening of the infarct-related artery and myocardial reperfusion, especially in the era of coronary intervention. 15 However, troponins can also be elevated in many non-coronary conditions such as renal failure, pulmonary embolism, heart failure, and tachyarrhythmias. 6 Therefore, more specific markers, perhaps rheological ones, are needed to confirm thrombus resolution, the absence of distal no-reflow, and myocardial reperfusion. This study provides an important basis for coagulation markers by linking their levels to definitive markers of myocardial reperfusion, namely MBG.
There are several coagulation markers in clinical use. Human beta-thromboglobulin is a protein stored in alpha-granules of platelets and released in large amounts upon platelet activation. Its levels serve as an indicator of platelet activation. 17 Human prothrombin fragment 1 + 2 is an amino-terminal activation product with a molecular weight of 35.5 kDa, produced by the cleavage of prothrombin by activated factor X7. A byproduct of this reaction is thrombin; therefore, human prothrombin fragment 1 + 2 indicates circulating thrombin and a tendency toward thrombosis. The thrombin-antithrombin complex is formed when thrombin binds to antithrombin and reflects the activation of the clotting pathway. 10 Previous studies have shown this parameter to be a sensitive marker for venous thromboembolism in the lower limbs.18,19 The t-PA-PAI-1 complex is formed by tissue plasminogen activator (t-PA) and plasminogen activator inhibitor type-1 (PAI-1). Plasmin is the main enzyme responsible for fibrinolysis in blood, and its formation is mainly regulated by t-PA, which promotes plasmin formation from plasminogen, leading to fibrinolysis, and by its counterpart, PAI-1, a serine protease produced by thrombocytes and endothelium, which blocks the conversion of plasminogen to plasmin. 13 The plasma level of the t-PA/PAI-1 complex reflects the concentrations of these two proteins, serving as an indicator of the thrombosis-fibrinolysis cycle. DD is formed when plasmin cleaves fibrin, indicating active thrombotic and fibrinolytic processes, such as in venous thromboembolism, cancer, inflammation, and post-surgical states. It is commonly used in clinical practice to rule out deep venous thrombosis and pulmonary thromboembolism.
In the present study, we showed that lower levels of the tPA/PAI complex and PTF 1-2 were significantly linked to higher myocardial blush grades (MBG 2 and 3), indicating better microvascular reperfusion. Conversely, patients with MBG 0 had notably higher levels of these markers, suggesting impaired microvascular perfusion. Although other coagulation markers such as D-dimer, thrombin-antithrombin complex (TAT), and β-thromboglobulin were assessed, only the tPA/PAI complex consistently correlated with MBG. However, none of the biomarkers were independently predictive in multivariate analysis. These results support the idea that specific thrombotic markers, especially the tPA/PAI complex, can provide insights into the quality of myocardial reperfusion at the microvascular level in STEMI patients. Because fibrinolysis plays a key role in thrombus resolution, elevated levels of the tPA/PAI complex may indicate impaired fibrinolytic activity and poorer reperfusion. Measuring this complex could help guide treatment decisions, especially when direct angiographic assessment of perfusion is not possible. Our findings are consistent with previous research suggesting that the tPA/PAI complex is a marker of impaired fibrinolysis and adverse cardiovascular outcomes, as shown in the SHEEP trial 14 and related studies. 20 Although antithrombotic therapies administered during primary PCI may influence circulating coagulation markers, all patients were treated according to a standardized guideline-directed protocol, thereby minimizing potential differential effects between study groups.
Limitations
This study has several limitations that should be acknowledged. First, it is a single-center study with a relatively small sample size, which may limit the generalizability of the findings to broader populations or different clinical settings. Second, the analysis focused primarily on angiographic and electrocardiographic indicators of reperfusion and did not include clinical outcomes or a comprehensive evaluation of the relationship between angiographic findings and echocardiographic measures of left ventricular volume and function. Consequently, it remains uncertain whether the observed associations between coagulation markers, thrombus burden, and myocardial blush grade translate into meaningful clinical outcomes or improvements in left ventricular remodeling. In addition, echocardiographic parameters were evaluated descriptively, as the study was not powered to detect meaningful differences between myocardial blush grade subgroups with respect to left ventricular function. Predictive values should be interpreted with caution, given the limited sample size and the prevalence-dependent nature of PPV and NPV.
Conclusion
Some coagulation markers, particularly the tPA/PAI-1 complex, may provide complementary information for assessing coronary thrombus burden and myocardial reperfusion in patients presenting with STEMI. Although these markers were not independently predictive, their association with angiographic indices of microvascular reperfusion suggests a potential role as adjunctive, non-invasive indicators. Larger, multicenter studies with standardized sampling and clinical follow-up are warranted to determine whether these biomarkers translate into meaningful clinical outcomes, including the development of heart failure or changes in echocardiographic parameters such as left ventricular ejection fraction and chamber dimensions.
Footnotes
Ethical Considerations
This study was approved by the Başkent University Institutional Review Board (approval No. KA14/308; date 08 October 2013) and conducted in accordance with the Declaration of Helsinki.
Consent to Participate
Written informed consent to participate was obtained from all participants prior to inclusion in the study.
Consent for Publication
Not applicable. This manuscript does not contain any individual person's data (including images or videos) that would require specific consent for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
De-identified data underlying the findings of this study are available from the corresponding author upon reasonable request and subject to institutional/ethical approvals.
Code Availability
Not applicable. No custom code was used.