
Abstract
Objective
To evaluate the association between alactic base excess (ABE) and mortality outcomes in patients with sepsis-associated disseminated intravascular coagulation (DIC) within intensive care unit (ICU).
Methods
Patients with sepsis-associated DIC were identified using Sepsis-3 criteria and the Japanese Association for Acute Medicine 2 DIC criteria. Multivariable Cox models and restricted cubic splines (RCS) were used to assess the relationship between ABE and 30-day and 90-day ICU mortality, with inflection points derived from a recursive algorithm. The predictive value of adding ABE to the Sequential Organ Failure Assessment (SOFA) score was further compared with SOFA alone.
Results
A total of 4839 patients with sepsis-associated DIC were included (median age 67.2 years; 59.8% male). Compared with Q3, multivariable Cox models showed higher 30-day mortality in Q1 (HR = 1.44, 95% CI 1.16-1.79), Q2 (HR = 1.26, 95% CI 1.01-1.57), and Q4 (HR = 1.45, 95% CI 1.15-1.81), with similar patterns for 90-day mortality (Q1: HR = 1.38, 95% CI 1.13-1.68; Q2: HR = 1.28, 95% CI 1.04-1.56; Q4: HR = 1.45, 95% CI 1.18-1.77). RCS analysis demonstrated a U-shaped association between ABE and mortality, with risk increasing at both low and high ABE levels. Adding ABE to SOFA significantly improved prediction for 30-day and 90-day mortality, with notable reclassification gains.
Conclusion
A clear U-shaped association was observed between ABE and 30-day/90-day ICU mortality in the patients with sepsis-associated DIC, suggesting that deviations from mid-range values may reflect early metabolic deterioration. However, the clinical implications require cautious interpretation and further validation in larger or prospective cohorts.
Keywords
Introduction
Sepsis is a systemic inflammatory response triggered by pathogens such as bacteria, viruses, and fungi, with high morbidity and mortality rates. It is one of the leading causes of intensive care unit (ICU) admissions worldwide, and the mortality rate further increases when multiple organ dysfunction is present. 1 DIC is a complex pathological condition involving widespread microvascular thrombosis and the consumption of coagulation factors. It is a common and severe complication of sepsis. 2 Sepsis patients with DIC have a higher prevalence of multiple organ dysfunction syndrome (32.0% vs 13.1%) and a higher mortality rate (24.8% vs 17.5%). 3 DIC arises from the dysregulation of the coagulation and fibrinolytic systems and is closely associated with systemic inflammation. Diffuse microthrombosis, along with widespread microvascular injury, leads to impaired tissue perfusion and oxygen delivery, which can also cause oxygen utilization dysfunction, ultimately resulting in metabolic acidosis. 4
In patients with sepsis-associated DIC, activation of the coagulation system not only leads to microthrombosis but may also affect metabolic processes. The consumption of coagulation factors and changes in blood flow can lead to the accumulation of acidic metabolites, exacerbating hyperlactatemia. 5 A study by Kobayashi et al suggested that DIC may play an important role in the mechanism of increased lactate production in critically ill patients. 6 Levraut et al prospectively studied 56 sepsis patients with normal or mildly elevated blood lactate levels, analyzing the relationship between lactate clearance and 28-day mortality. They found that the lactate clearance rate in survivors was significantly higher than that in non-survivors [(0.86 ± 0.32) versus (0.58 ± 0.18) L/(h·kg), P < 0.005]. 7 A study by Mark E. Mikkelsen and colleagues showed that moderate elevation of serum lactate levels (>4 mmol/L) is closely associated with mortality in sepsis patients. 8
However, hyperlactatemia cannot fully explain acid-base balance, as these patients often have concomitant acid-base imbalances, which should be identified and addressed. ABE refers to the sum of lactate and standard base excess (BE). 9 Patients with sepsis-associated DIC may experience both oxygen delivery and oxygen utilization dysfunction. Changes in ABE values (especially a decrease in ABE) usually indicate worsening metabolic acidosis and are associated with the severity of illness and mortality. This acidosis is closely related to the occurrence and progression of DIC. 10 Existing studies indicate that ABE is a risk factor for short-term mortality in patients with shock, 11 and is also closely associated with the prognosis of patients with myocardial infarction and heart failure. 12
ABE independently reflects the degree of metabolic acid-base imbalance and is closely related to various physiological states such as renal function, cardiovascular status, and oxygenation, providing guidance for early resuscitation and prognosis. 13 ABE is closely related to the clinical prognosis of sepsis patients. Although studies have explored the role of ABE in critically ill patients, there is limited research on its specific prognostic value in sepsis-associated DIC patients. Therefore, this study aims to fill this gap and provide new, more precise prognostic assessment tools for clinical use, which could improve the treatment outcomes and prognosis management of sepsis and DIC.
Methods
Study Data
The data for this study were obtained from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. This database is a large clinical database established through a collaboration between the Massachusetts Institute of Technology (MIT) and the Beth Israel Deaconess Medical Center (BIDMC), primarily containing clinical data from patients in intensive care units. 14 One of authors, Yang Chen, has completed Human Subjects Research Training Certificate (Certificate No. 53753450) and completed several prior MIMIC- IV related work.15,16 The use of the data was approved by the Institutional Review Boards of MIT (2001-P-001699/14) and BIDMC (No.0403000206). The project adheres to the principles outlined in the Declaration of Helsinki.
Participants
The focus of this study is on patients with sepsis-associated DIC. Sepsis patients were identified according to the Sepsis-3 diagnostic criteria. 17 DIC patients were diagnosed using the modified version of Japanese Association for Acute Medicine (JAAM) 2 DIC criteria, JAAM-2 DIC criteria, with a score ≥3 indicating DIC. 18 The criteria includes the following parameters: (i) platelet count <80 × 109/L or a decrease of >50% within 24 h (3 points)/80 × 109/L ≤ platelet count <120 × 109/L or a decrease of 30%–50% within 24 h (1 point); (ii) fibrin degradation products ≥25 μg/mL (3 points)/10 ≤ fibrin degradation products <25 μg/mL (1 point); (iii) prothrombin time ratio ≥ 1.2 (1 point). The exclusion criteria were as follows: (i) patients without lactate and base excess values on the first day after admission; (ii) patients aged below 18 years; (iii) patients who underwent kidney transplantation; (iv) patients receiving renal replacement therapy; (v) patients with ICU stays shorter than 24 h; (vi) patients lacking records of intake and output on the first day after admission; (vii) patients with multiple hospital or ICU admissions; (viii) patients with incorrect death records or death occurring within the first 24 h; (ix) patients not meeting the JAAM-2 DIC diagnosis criteria.
Data Collection
We used Structured Query Language to extract basic data, including demographic characteristics including age, gender, race, height, and weight; vital signs including blood pressure, heart rate, respiratory rate, oxygen saturation, and fluid balance; ICU severity score: Sequential Organ Failure Assessment (SOFA) score; comorbidities including acute respiratory failure, sepsis-associated encephalopathy, septic shock, acute kidney injury (AKI), myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, hepatic disease, malignant cancer, and diabetes mellitus; laboratory tests including anion gap, bicarbonate, blood urea nitrogen (BUN), calcium, chloride, sodium, potassium, phosphorus, creatinine, estimated glomerular filtration rate (eGFR), partial pressure of carbon dioxide (PaCO2), potential of hydrogen (PH); ICU interventions including renal replacement therapy, and mechanical ventilation; medications including vasopressors, antibiotics, furosemide, and glucocorticosteroids. We extracted data from the first admission records and selected the first value within 24 h after admission for multiple measurements. The calculation formula is: ABE (mmol/L) = lactate (mmol/L) + BE (mmol/L). Both BE and lactate values were measured on the first day of ICU admission. Body mass index (kg/m2) = weight (kg)/height (m)2.
Study Outcomes
The primary endpoints of our study were: (1) 30-day ICU all-cause all-cause mortality, defined as death within 30 days after ICU admission; (2) 90-day ICU all-cause mortality, defined as death within 90 days after ICU admission. The secondary endpoints were: (1) ICU all-cause mortality, defined as death during the ICU stay; (2) hospital all-cause mortality, defined as death during the hospital stay; (3) length of ICU stay; (4) length of hospital stay. The secondary endpoints were only described.
Statistical Analysis
In this study, the proportion of missing values for included covariates did not exceed 25% (Supplementary Table S1). Therefore, we used the “miceforest” package in Python to perform multiple imputation by chained equations to handle the missing data. Normality of variable was assessed using the Shapiro-Wilk test. Continuous variables included in this analysis were non-normal distributions, expressed as median and interquartile range (IQR), and intergroup comparisons were performed using the Kruskal-Wallis test. Categorical variables were presented as frequencies and percentages, and intergroup comparisons were made using the Chi-square or Fisher exact test. ABE was divided into four groups based on its quartiles, and baseline characteristics were compared across these four groups. We used multivariable Cox proportional hazards models and restricted cubic spline (RCS) analyses to assess the associations between ABE with 30-day and 90-day ICU all-cause mortality, with calculating hazard ratios (HR) and 95% confidence intervals (CI). Potential models with different combinations of confounders were adjusted for in the analysis. Model I: unadjusted; Model II: adjusted for age, sex, BMI, and race; Model III: adjusted for age, sex, BMI, race, and comorbidities; Model IV: adjusted for age, sex, BMI, race, vital signs, comorbidities, and treatment measures. Additionally, if a non-linear relationship was identified, a recursive algorithm was used to determine the optimal inflection point. 19 Following this, a two-piece Cox proportional hazards model was fitted on each side of the cut-off point to assess the distinct hazard ratios. Furthermore, stratified subgroup analyses were performed based on age (≥ 65 years vs <65 years), sex (male vs female), BMI (≥30 vs <30), and AKI (AKI stage 0/I vs AKI stage II/III). Then, to compare the prognostic performance of ABE with conventional acid–base markers, we evaluated the discrimination of ABE, BE, and lactate for 30-day and 90-day ICU mortality. For each marker, receiver operating characteristic (ROC) curves were generated and the area under the curve (AUC) with 95% confidence interval (CI) was calculated. Pairwise comparisons of AUCs between ABE, BE, and lactate were conducted using the DeLong test. Finally, to assess the performance of ABE combined with current ICU severity score in predicting mortality outcomes, we compared the ABE combined with SOFA to the SOFA score. We calculated the AUCs with 95% CIs and statistically compared between two models using the DeLong test. In addition, we further quantified the incremental prognostic value of incorporating ABE into SOFA score using the Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) indicators.
A two-tailed p < 0.05 was considered statistically significant. All analyses were applied utilising SPSS Statistics (version 27, USA), and Python (version 3.11.1, USA) and R (version 4.3.2, Austria).
Results
Baseline Characteristics
This study involved 3333 patients (the flowchart is shown in Figure 1), with median (IQR) 68.1 (57.4-78.1) years and 55.8% males. ABE was divided into four groups based on its quartiles: Q1: ABE ≤ −2.0 mmol/L, Q2: −2.0 < ABE ≤ 1.0 mmol/L, Q3: 1.0 < ABE ≤ 3.0 mmol/L, Q4: ABE > 3.0 mmol/L. Baseline characteristics varied meaningfully across ABE quartiles. Several comorbidities, such as acute respiratory failure, sepsis shock, chronic pulmonary disease, hepatic disease, and malignancy, were unevenly distributed among the groups. Laboratory profiles also differed, with eGFR showing a clear stepwise increase from Q1 to Q4, alongside significant variations in PH, PaCO2, creatinine, BUN, and electrolytes. Full details of these differences are provided in Table 1.

Flowchart of this study. DIC, disseminated intravascular coagulation; ICU, intensive care unit; JAAM2-DIC, Japanese Association for Acute Medicine 2 Disseminated Intravascular Coagulation; MIMIC-IV, Medical Information Mart for Intensive Care IV.
Baseline Characteristics among Patients with Sepsis-Induced Disseminated Intravascular Coagulation.

Q1: ABE ≤ −2.0 mmol/L, Q2: −2.0 < ABE ≤ 1.0 mmol/L, Q3: 1.0 < ABE ≤ 3.0 mmol/L, Q4: ABE > 3.0 mmol/L.
Abbreviations: AKI, acute kidney injury; BMI, body mass index; BUN, blood urea nitrogen; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; PaCO2, partial pressure of carbon dioxide; PH, potential of hydrogen; SAE, sepsis associated encephalopathy; SBP, systolic blood pressure; SOFA, sequential organ failure assessment.
Study Outcomes Across ABE Quartiles
Figure 2 shows the distribution of our study outcomes of interest across the ABE quartiles. The incidence of all four outcomes in the first quartile group was significantly higher than in the other three groups: 30-day ICU all-cause mortality: Q1 (36.70%) > Q2 (24.70%) > Q4 (23.76%) > Q3 (14.82%), 90-day ICU all-cause mortality: Q1 (34.87%) > Q2 (25.52%) > Q4 (24.14%) > Q3 (15.47%). For other outcomes, there were similar trends.
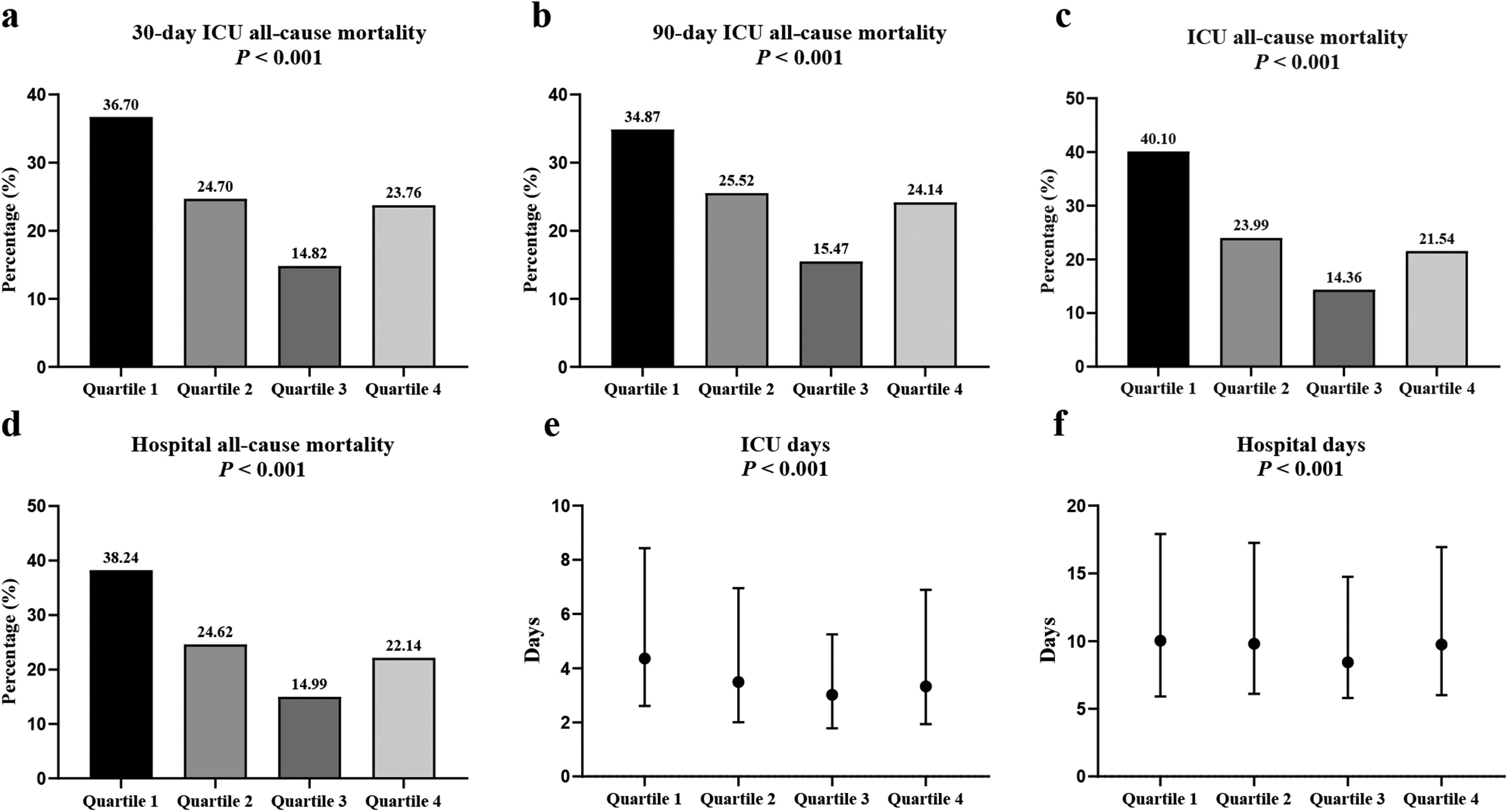
Distribution of study outcomes across alactic base excess quartile groups. Q1: ABE ≤ −2.0 mmol/L, Q2: −2.0 < ABE ≤ 1.0 mmol/L, Q3: 1.0 < ABE ≤ 3.0 mmol/L, Q4: ABE >3.0 mmol/L. ICU, intensive care unit.
Relationships of ABE with 30-Day and 90-Day ICU All-Cause Mortality
Kaplan-Meier survival curves (Figure 3) demonstrate significantly different survival probabilities across ABE quartiles, with Q1 showing markedly lower survival rates. The Log-rank test indicates a significant difference in survival distributions (both P < 0.0001).

Kaplan-Meier survival curves across alactic base excess quartile groups for 30-day (a) and 90-day (b) ICU all-cause mortality. Q1: ABE ≤ −2.0 mmol/L, Q2: −2.0 < ABE ≤ 1.0 mmol/L, Q3: 1.0 < ABE ≤ 3.0 mmol/L, Q4: ABE >3.0 mmol/L. ICU, intensive care unit.
Table 2 presents the crude and multivariable Cox models, demonstrating the associations across sequential adjustment levels for potential confounders. The results of multivariable Cox proportional hazards models indicated that compared to Q3 of ABE (due to the lowest mortality rate among quartiles), Q1, Q2, and Q4 were associated with higher risks of 30-day ICU all-cause mortality (Q3 as reference; Q1: HR = 1.44, 95% CI 1.16-1.79; Q2: HR = 1.26, 95% CI 1.01-1.57; Q4: HR = 1.45, 95% CI 1.15-1.81) and 90-day ICU all-cause mortality (Q3 as reference; Q1: HR = 1.38, 95% CI 1.13-1.68; Q2: HR = 1.28, 95% CI 1.04-1.56; Q4: HR = 1.45, 95% CI 1.18-1.77).
Associations Between ABE with 30-Day and 90-Day ICU All-Cause Mortality.

Q1: ABE ≤ −2.0 mmol/L, Q2: −2.0 < ABE ≤ 1.0 mmol/L, Q3: 1.0 < ABE ≤ 3.0 mmol/L, Q4: ABE > 3.0 mmol/L.
Model I: unadjusted;
Model II: adjusted for age, sex, body mass index and race;
Model III: based on Model II further adjusted for acute respiratory failure, sepsis associated encephalopathy, sepsis shock, acute kidney injury, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, hepatic disease, malignant cancer, diabetes mellitus;
Model IV: based on Model III further adjusted for heart rate, systolic blood pressure, diastolic blood pressure, blood oxygen saturation, respiratory rate, glucose, input, output, Sequential Organ Failure Assessment, mechanical ventilation, vasopressor, antibiotics, furosemide, glucocorticosteroid.
*P for trend <0.001 for each model corresponding to this outcome.
Abbreviations: ABE, alactic base excess; CI, confidence interval; HR, hazard ratio; ICU: intensive care unit.
RCS Analysis and Inflection Points of ABE for 30-Day and 90-Day ICU all-Cause Mortality
Figure 4 demonstrates the RCS results of nonlinear relationships between ABE and risk of 30-day and 90-day ICU all-cause mortality in patients with sepsis-associated DIC (P overall <0.001, P non-linear <0.001 for both). The curves were overall U-shaped, indicating that either high or low ABE values were associated with higher mortality risk, with nadirs of ABE between 2 and 3 mmol/L. We then applied recursive algorithm to identify the ABE inflection points, measured in the ICU at 2.5 mmol/L for 30-day all-cause mortality and 2.4 mmol/L for 90-day all-cause mortality.

Restricted cubic spline analysis of the associations between alactic base excess with 30-day (a) and 90-day (b) ICU all-cause mortality. CI, confidence interval; HR, hazard ratio; ICU, intensive care unit.
Table 3 shows that using two-segment Cox proportional hazards models on either side of the identified inflection points, we observed a significant inverse association between ABE and mortality outcomes below the inflection points (30-day mortality: HR = 0.95, 95% CI 0.93-0.97; 90-day mortality: HR = 0.96, 95% CI 0.94-0.98). In contrast, ABE values exceeding these thresholds were associated with a significantly increased risk of 30-day and 90-day all-cause mortality (30-day: HR = 1.10, 95% CI 1.06-1.14; 90-day: HR = 1.08, 95% CI 1.04-1.12).
Inflection Point Analysis of ABE on 30-Day and 90-Day ICU All-Cause Mortality.

Abbreviations: ABE, alactic base excess; CI, confidence interval; ICU, intensive care unit.
Subgroup Analysis
We performed a risk stratification analysis of 30-day and 90-day all-cause mortality in sepsis-associated DIC patients based on age, sex, BMI, and AKI (Figure 5). Subgroup analyses demonstrated no significant interactions between ABE quartiles and any examined factors for either 30-day or 90-day all-cause mortality. The direction of associations remained consistent across all subgroups.

Subgroup analysis of the association between alactic base excess with 30-day and 90-day ICU all-cause mortality. Cox proportional hazard model was adjusted for age, sex, body mass index and race, acute respiratory failure, sepsis associated encephalopathy, sepsis shock, acute kidney injury, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, hepatic disease, malignant cancer, diabetes mellitus, heart rate, systolic blood pressure, diastolic blood pressure, blood oxygen saturation, respiratory rate, glucose, input, output, Sequential Organ Failure Assessment, anionic gap, bicarbonate, blood urea nitrogen, calcium, chloride, sodium, potassium, phosphorus, creatinine, estimated glomerular filtration rate, partial pressure of carbon dioxide, potential of hydrogen, renal replacement therapy, mechanical ventilation, vasopressor, antibiotics, furosemide, glucocorticosteroid. Q1: ABE ≤ −2.0 mmol/L, Q2: −2.0 < ABE ≤ 1.0 mmol/L, Q3: 1.0 < ABE ≤ 3.0 mmol/L, Q4: ABE > 3.0 mmol/L. AKI, acute kidney injury; BMI, body mass index; CI, confidence interval; HR, hazard ratio; ICU, intensive care unit.
Predictive Performance of ABE, BE, and Lactate for 30-Day and 90-Day ICU All-Cause Mortality
Across both 30-day and 90-day ICU all-cause mortality (Supplementary Figure S1), ABE consistently demonstrated the best discriminative performance. For 30-day mortality, ABE achieved an AUC of 0.580 (95% CI: 0.563-0.597), exceeding BE (0.522, 95% CI: 0.505-0.539) and lactate (0.535, 95% CI: 0.518-0.552). Similar patterns were observed for 90-day mortality, where ABE again outperformed BE (0.530, 95% CI: 0.513-0.547) and lactate (0.520, 95% CI: 0.503-0.537), with an AUC of 0.573 (95% CI: 0.556-0.590). DeLong tests confirmed that ABE was significantly superior to both BE and lactate at each time point (all P < 0.05).
Predictive Performance of ABE Combined with SOFA for 30-Day and 90-Day ICU All-Cause Mortality
Combining ABE into the SOFA score significantly improved the predictive performance of 30-day and 90-day all-cause mortality in patients with sepsis-associated DIC (Table 4 and Figure 6). Specifically, the AUC of ABE combined with SOFA was significantly higher than that of SOFA alone (30-day ICU all-cause mortality: ABE + SOFA vs SOFA: 0.631 vs 0.610, DeLong test P = 0.008; 90-day ICU all-cause mortality, ABE + SOFA vs SOFA was 0.621 vs 0.602, DeLong test P = 0.006). In addition, significant improvements in risk reclassification were achieved by ABE combined with SOFA (30-day ICU all-cause mortality: NRI of 29.10%, IDI of 1.30%; 90-day ICU all-cause mortality: NRI of 27.31%, IDI of 1.10%).

Comparison of predictive performance between ABE combined with SOFA and SOFA alone for 30-day (a) and 90-day (b) ICU all-cause mortality. ABE, alactic base excess; SOFA, Sequential Organ Failure Assessment.
Comparison of Predictive Performance of Models Incorporating ABE and SOFA for 30-Day/90-Day All-Cause Mortality in Sepsis Patients.

Abbreviations: ABE, alactic base excess; AUC, area under curve; CI, confidence interval; ICU, intensive care unit; IDI, Integrated Discrimination Improvement; NRI, Net Reclassification Improvement; SOFA, Sequential Organ Failure Assessment.
Discussion
Our study is the first to suggest that ABE is associated with the risk of 30-day and 90-day ICU all-cause all-cause mortality in sepsis-associated DIC patients, with a U-shaped relationship. There were significant differences in baseline characteristics among the four ABE quartiles, with quartiles Q1, Q2, and Q4 all associated with increased 30-day and 90-day ICU all-cause all-cause mortality. In addition, the ABE inflection points determined by the recursive algorithm were 2.5 mmol/L (30-day ICU all-cause all-cause mortality) and 2.4 mmol/L (90-day ICU all-cause all-cause mortality), respectively. Moreover, incorporating ABE into the SOFA score enhanced performance in predicting death. These findings highlight the potential of ABE as an important biomarker for risk stratification and suggest its utility in enhancing clinical decision-making in sepsis-associated DIC patients.
Sepsis-associated DIC is often accompanied by severe metabolic acidosis. In the process of DIC, microthrombi form in the microvasculature, leading to tissue hypoxia and inadequate perfusion. Due to inadequate oxygen supply, tissues produce acidic substances through anaerobic metabolism, leading to the accumulation of acidic metabolic products (such as lactate and hydrogen ions) in the blood and a decrease in ABE values. 20 Additionally, microthrombi and endothelial injury lead to microcirculatory disturbances, which in turn affect tissue and organ oxygenation, further exacerbating metabolic acidosis. Furthermore, abnormal activation of the coagulation system leads to excessive consumption of coagulation factors in the blood. This imbalance between coagulation and fibrinolysis not only affects blood clotting but also may lead to microthrombus formation and further impairment of organ perfusion. 21 Moreover, sepsis itself is caused by a systemic inflammatory response, and the occurrence of DIC further exacerbates the inflammatory process. Some inflammatory factors activate the coagulation system, while also increasing vascular permeability, causing edema and organ dysfunction. 22 Especially in critical organs such as the liver, kidneys, and heart.23,24 The kidney is crucial for maintaining acid-base balance, and renal injury can lead to the accumulation of acidic substances and loss of buffering capacity. 25 Importantly, ABE, as an important indicator for assessing fluid resuscitation and metabolic status in sepsis patients, can reflect whether the acid-base balance has been effectively corrected.26,27 Changes in ABE values directly reflect the pathophysiological status of sepsis-associated DIC patients and are closely associated with mortality.
Although some studies have explored the prognostic value of ABE in sepsis, shock, and other critical illnesses, the role and clinical prognostic value of ABE in sepsis-associated DIC patients have not been investigated. A study by Joaquin Cantos et al showed that negative ABE (<−3 mmol/L) patients had higher mortality than those with neutral ABE (≥−3 and <4 mmol/L) (adjusted HR = 1.43; 95% CI 1.02–2.01). Additionally, in patients with GFR >60 mL/min/1.73 m2 (N = 493), higher mortality was observed in those with negative ABE (adjusted HR = 2.43, 95% CI 1.07–5.53). 13 A study of 143 shock patients found that ABE < −3.63 mmol/L was associated with a HR of 3.19% and 95% CI (1.62-6.27) for 28-day hospital mortality. 11 Lactate, PH, and BE are all suitable predictors of mortality in ICU patients, with BE and PH not outperforming lactate in predicting mortality. 28
The observed U-shaped association between ABE and mortality suggests that both excessively low and excessively high ABE values reflect distinct but clinically relevant pathophysiological states in sepsis-associated DIC. On the one hand, reduced ABE indicates worsening metabolic acidosis, impaired tissue perfusion, or progression of coagulopathy, all of which are well-recognised drivers of organ dysfunction and early mortality.29–31 On the other hand, markedly elevated ABE may represent overcompensated alkalosis, aggressive buffering responses, or metabolic disturbances related to hyperventilation, which often accompany severe systemic inflammation or advanced organ failure, potentially explaining the elevated mortality risk at the upper end of the ABE spectrum.32,33 Taken together, these findings support the concept that changes in ABE may function as an early warning indicator for deterioration in patients with sepsis-associated DIC. Rather than a linear risk gradient, the U-shaped pattern highlights that both extremes of ABE warrant clinical attention.
By monitoring ABE values, clinicians can detect disease progression early and adjust treatment strategies, such as optimizing fluid resuscitation, adjusting medication use, and providing early hemodynamic support. In the future, ABE could be combined with other clinical indicators (eg comorbidities, hemodynamic parameters) to further improve the accuracy of prognostic prediction. The simplicity and reliability of ABE in assessing patient metabolic status make it an important component in developing robust multivariable predictive models. Furthermore, Machine learning algorithms excel at capturing complex, nonlinear interactions among variables, offering enhanced predictive capabilities beyond traditional statistical models, particularly in identifying subtle risk patterns. Incorporating ABE into machine learning algorithms is promising to provide significant benefits for predicting patient outcomes.
Limitations
Nevertheless, there are several limitations in this analysis. First, this is a single-center retrospective analysis, and further validation is needed through larger-scale, multi-center prospective studies. Sepsis-associated DIC patients may differ by region and underlying etiology, so cross-regional and cross-population studies are needed to assess the generalizability and accuracy of the findings. Second, due to the limitations of the database itself, some confounding factors that may affect the results were not included, which could impact the accuracy of our findings. Third, we only considered the first ABE value at first day post admission and did not perform dynamic monitoring. Future studies should focus on the dynamic changes of ABE during treatment and explore its use as a tool for monitoring treatment response. Finally, while ABE serves as a valuable indicator for assessing acid-base balance, it reflects only a single aspect of the overall metabolic profile. We did not include other key metabolic markers, such as serum osmolarity, and ketone bodies, which could offer a more comprehensive assessment of patient status and prognostic risk in sepsis-associated DIC. The omission of these additional metrics may have introduced some degree of bias into our findings.
Conclusion
The relationship between ABE and both 30-day and 90-day ICU all-cause mortality exhibits a U-shaped pattern, with identified inflection points of ABE at 3.1 mmol/L for 30-day ICU all-cause mortality and 3.0 mmol/L for ICU all-cause 90-day mortality. Maintaining ABE levels near these thresholds may indicate optimal metabolic balance, potentially contributing to improved survival outcomes. Deviations from these inflection points, whether towards acidosis or alkalosis, were linked to a higher risk of mortality, highlighting the need for careful monitoring and management of ABE levels to mitigate adverse outcomes in critically ill patients.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251415379 - Supplemental material for Prognostic Impact of Alactic Base Excess in Critically Ill Patients with Sepsis-Associated Disseminated Intravascular Coagulation: A Retrospective Observational Study
Supplemental material, sj-docx-1-cat-10.1177_10760296251415379 for Prognostic Impact of Alactic Base Excess in Critically Ill Patients with Sepsis-Associated Disseminated Intravascular Coagulation: A Retrospective Observational Study by Shu Zhang, Yang Chen, Kaihe Xie, Na Xu, Ting Liu, Jipeng Liu, Qingzhen Han and Lin Wang in Clinical and Applied Thrombosis/Hemostasis
Footnotes
List of Abbreviations
Acknowledgements
We gratefully acknowledge the MIMIC-IV database research team and extend our sincere thanks to all the participants who contributed to this study.
Ethics Approval and Consent to Participate
Ethical approval for data collection was approved by the institutional review boards of the BIDMC (2001-P-001699/14) and Massachusetts Institute of Technology (No.0403000206). In this work, all data were anonymised and could therefore be exempt from local ethics review committee.
Consent for Publication
All authors have reviewed and approved the final version of the manuscript for submission.
Authors’ Contributions
Shu Zhang: Data curation, Formal analysis, Conceptualization, Methodology, Writing-original draft. Yang Chen: Data curation, Formal analysis, Conceptualization, Methodology, Writing-review & editing. Kaihe Xie: Writing- review & editing. Na Xu: Writing- review & editing. Ting Liu: Writing- review & editing. Jipeng Liu: Writing- review & editing. QingZhen Han: Conceptualization, Methodology, Formal analysis, Writing – review & editing, Supervision. Lin Wang: Conceptualization, Methodology, Formal analysis, Writing – review & editing, Supervision. All named authors meet the criteria for authorship as outlined by the International Committee of Medical Journal Editors, take collective responsibility for the integrity of the work, and have provided their approval for its publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Suzhou Industrial Park Medical and Health Innovation Research Project, (grant number CXYJ2024A08).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on reasonable request to corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.