
Abstract
Severe sepsis remains the most common cause of death in critically ill patients, and thrombin plays a crucial role in the pathogenesis of sepsis-associated disseminated intravascular coagulation (DIC). The purpose of this study was to profile prothrombin fragment (F1.2), thrombin–antithrombin complex (TAT), and
Keywords
Disseminated intravascular coagulation (DIC) is a complication of many diseases including sepsis, cancer, and trauma. Several factors contribute to the development of DIC including aberrations in the endothelium and altered levels of various endogenous procoagulant, anticoagulant, and fibrinolytic factors. Excessive thrombin generation or the failure to stop local thrombin production is characteristic of this syndrome and can lead to impaired fibrin degradation leading to intravascular fibrin deposition. 1 –3 Thrombin generation also enhances the modulation of inflammation associated with DIC. Low platelet counts are also observed with DIC. 4 Production of microthrombi can reduce organ perfusion and cause organ shut down. Mortality from sepsis doubles when it is complicated by DIC. 2
Several groups have attempted to classify DIC by assigning a score based on the results of several blood tests including
Since DIC can be caused by several underlying diseases, the therapeutic treatment of this syndrome is difficult. In 2001, Xigris, a recombinant form of activated protein C was approved by the Food and Drug Administration for patients with severe sepsis and an increase risk of death. 6,7 In 2011, Xigris was withdrawn from the market due to failure of the PROWESS-SHOCK study. 7
Thrombomodulin (TM) is a transmembrane protein that complexes with thrombin to activate protein C. Recently, recombinant human soluble TM (r-TM) has been developed by Asahi Kasei Pharma for the treatment of DIC in Japan (ART-123). The ART-123 is a soluble TM with multiple mechanisms of action that protect the microcirculation in severe sepsis. The r-TM appears to enhance the reversal of DIC in these patients. It does this by stopping the thrombin-mediated clotting and enhancing the protein C activation at the site of clot formation. In addition, r-TM has been shown to have a strong antiinflammatory component. 8,9 Previous clinical trials with r-TM have shown minimal bleeding risk. 10,11 Therefore, a global phase 2b study was undertaken to evaluate the use of ART-123 (r-TM) in reducing mortality in patients with sepsis-associated DIC. The study design and treatment randomization and clinical results have been previously published. 12 Because of the multitargeted mechanism of action, results from the post hoc analyses of the global phase 2b data, commercial experience gained with the use of ART-123 in Japan, and an acceptable safety profile, it is anticipated that ART-123 holds promise and may demonstrate a survival benefit better than Xigris in patients with severe sepsis and coagulopathy. In the clinical trials conducted for Xigris, coagulopathy was not an entry criterion.
The ART-123 is commercially available only in Japan as Recomodulin for the treatment of DIC. This approval was based on a phase 3 trial in which the comparator arm was heparin. The phase 2b global trial was studied in patients with sepsis having DIC or at risk of DIC, and the comparator arm was placebo (standard of care). Global development regulations require the comparator arm to be either a product approved for the indication to be studied or it be placebo controlled.
The purpose of this study was to determine the biomarker levels, including prothrombin fragment (F1.2), DD, and thrombin–antithrombin complex (TAT), at the baseline and throughout the study period to investigate whether there was a difference in the downregulation of these markers after treatment with r-TM and placebo for sepsis-induced DIC.
Materials and Methods
Patients
Patients with sepsis and suspected DIC were enrolled in the randomized, double-blind, placebo-controlled, phase 2b study to evaluate the safety and efficacy of r-TM, ART-123, and also to evaluate coagulation and fibrinolytic parameters. This study was conducted in compliance with the ethical principles of the Declaration of Helsinki and in compliance with all International Conference on Harmonization (ICH) Good Clinical Practice (GCP) Guidelines. The study design and clinical outcomes have been previously described in detail. 12 Briefly, adult patients (>18 years) admitted to 1 of the 233 study centers in 17 countries with sepsis and suspected DIC, identified locally at each center using a score based on the platelet count and PT international normalized ratio (INR) derived from the ISTH DIC score, were screened for inclusion. 5 Patients were excluded from the study if any of the following criteria were present: unable to obtain informed consent; presence of any disorder other than sepsis that could alter coagulation; recent history of significant bleeding or increased risk of bleeding (eg, surgery within 12 hours of screening); presence of a disorder requiring anticoagulation; use of drotrecogin alfa (activated) within the 24 hours prior to enrollment or intended use; use of anticoagulants, antiplatelet agents, and thrombolytics within the 72 hours prior to study dosing, or intended use with the exception of heparin locks/flushes or deep vein thrombosis (DVT) prophylaxis; platelet count <20 000; and life expectancy <90 days or current use of any chemotherapy agents.
After enrollment, the patients were randomly assigned in a 1:1 ratio to receive either intravenous (iv) ART-123 (n = 371; 0.06 mg/kg/d) for 6 days or placebo (n = 370), in addition to standard of care as determined by the treating clinician. The dose of ART-123 administered was 0.06 mg/kg (0.01 mL/kg) up to a maximum dose of 6 mg (1 mL) for patients who weighed >100 kg. Patients were followed for 28 days after study inclusion. The primary end point for this trial was all-cause day 28 mortality. A 3.8% absolute survival benefit (82.2% vs 78.4%, P value = .273) was observed in the ART-123 arm. Post hoc analyses identified a patient population (patients with severe sepsis with septic shock and/or respiratory failure and coagulopathy identified by INR >1.4) that is expected to show at least an 8% absolute survival benefit on day 28 mortality (post hoc rates of 64% vs 52%).
Blood samples were drawn for the biomarkers at the baseline (day 0), 24 hours after the first dosage (day 1), day 3 immediately before the next dosage (day 3 pre), 24 hours after the second dosage (day 3 post), and on days 7 and 14. The samples were collected only when the patients were in the hospital, resulting in about 40% of the patients not having samples drawn on day 14. Most of the missing samples were a result of patients who had been discharged from the hospital. The remaining was a result of patient deaths (day 14 mortality rates were TM 12.7% and placebo 14.6%).
In addition to the patients from the randomized trial, normal healthy volunteers (n = 30; 15 males and 15 females) from a separate study have been included as normal controls.
Sample Analysis
Citrated whole blood was drawn from these patients, and plasma was prepared and frozen at −70°C and shipped to the central laboratory, Covance (Princeton, New Jersey). Samples were then organized in complete patient sets and shipped to Loyola Hemostasis and Thrombosis Research Laboratories on dry ice for analyses. The plasma samples were analyzed using the commercially available enzyme-linked immunosorbent assay kits for prothrombin F1.2 complex, TAT (Dade Behring Siemens, Miami, Florida) and Asserachrom DD (Stago, Parsippany, New Jersey). The samples were analyzed blindly in batches, and results were transmitted to Covance for input into the clinical trial database.
After the study was completed the randomization code was sent, and the data were analyzed using descriptive statistics and the rank-based testing method. The descriptive statistics includes graphs of the median values across time with the interquartile range error bars. The upper limit of the range represents the third quartile (ie 75% percentile), and the lower limit represents the first quartile (ie 25% percentile). The rank-based method has been used to incorporate informative missingness (ie deaths) and to allow for skewed data. This method is similar to the rank-based Wilcoxon test, but in the present application patients who die are treated as if they have no change from the baseline for the purpose of assigning ranks and testing. 13 Patients with missing data not due to death are excluded from the tests. A single sample from each of the healthy volunteers was analyzed in a similar manner.
Results
The cumulative results for each of the individual thrombin generation markers, namely F1.2 and TAT, and of the fibrin degradation marker, namely DD, were compiled from the placebo, ART-123-treated groups, and the normal controls (Tables 1 –4). The results for the baseline were compared with the controls (Table 1). A clear difference is seen in each of the markers between the normal control patients and the patients with sepsis and suspected DIC. The treatment groups from the randomized study are generally balanced.
Control and Study ART-123 Baseline
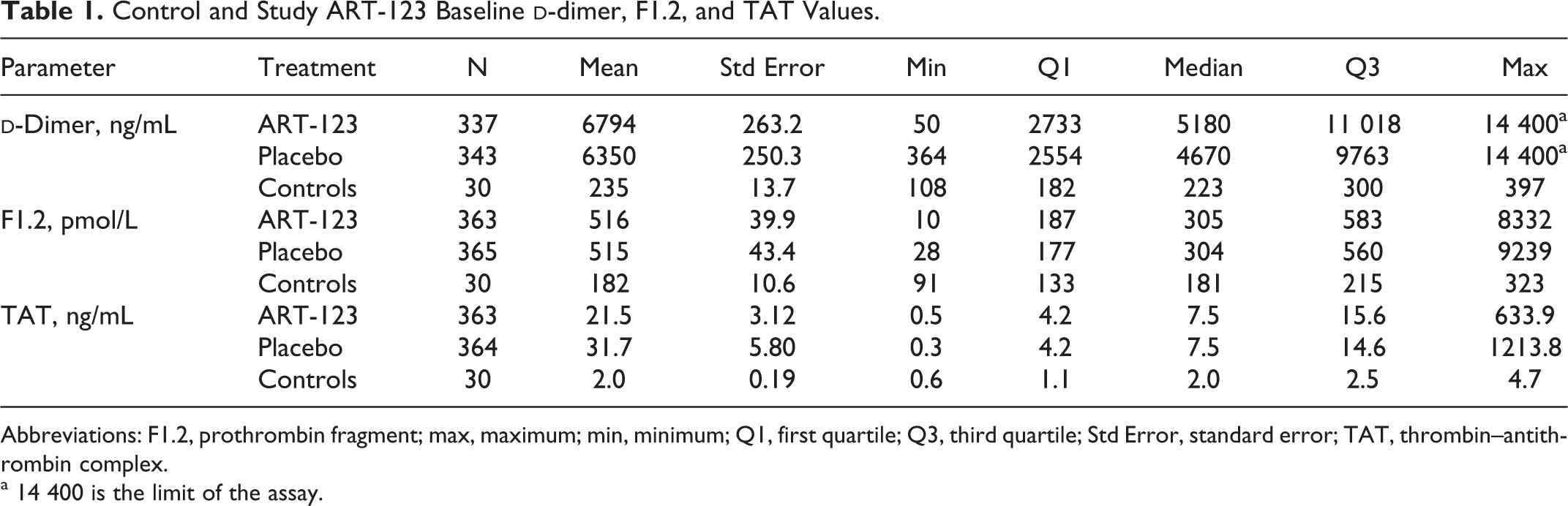
Abbreviations: F1.2, prothrombin fragment; max, maximum; min, minimum; Q1, first quartile; Q3, third quartile; Std Error, standard error; TAT, thrombin–antithrombin complex.
a 14 400 is the limit of the assay.
The F1.2 Values From Patients in the ART-123 Study From Days 1 to 14.
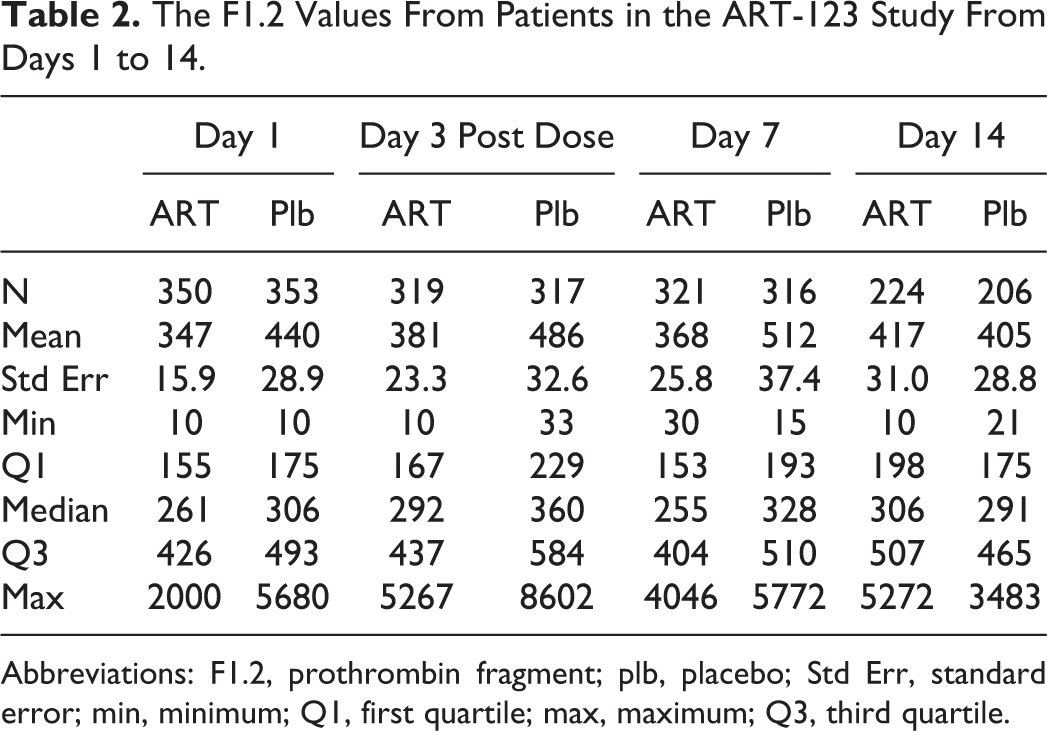
Abbreviations: F1.2, prothrombin fragment; plb, placebo; Std Err, standard error; min, minimum; Q1, first quartile; max, maximum; Q3, third quartile.
The TAT Values From Patients in the ART-123 Study From Days 1 to 14.
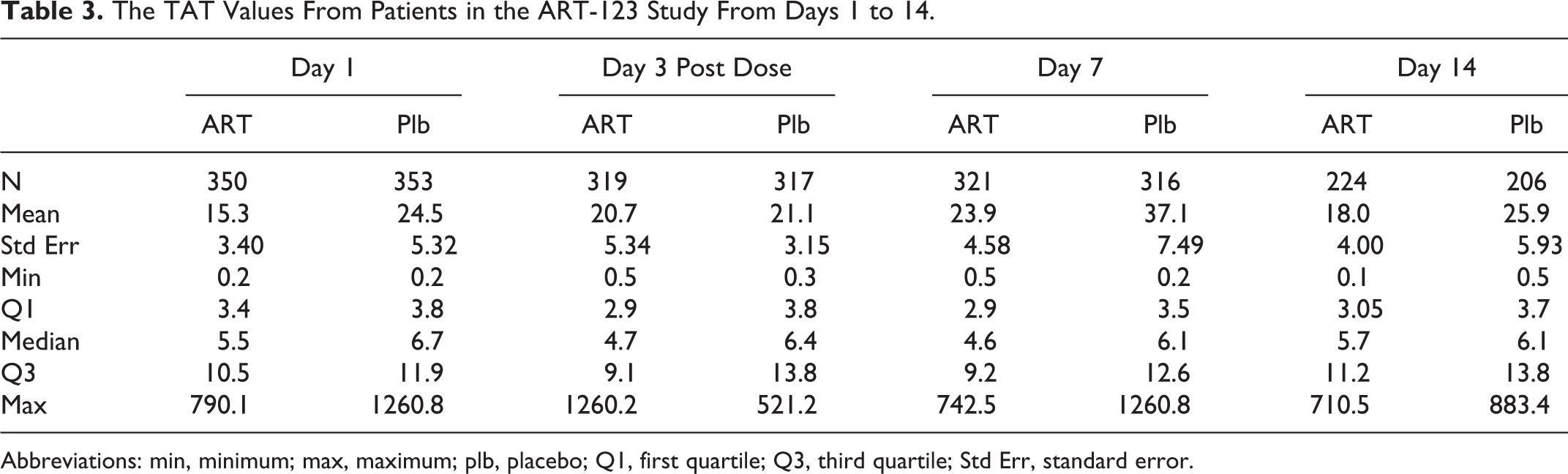
Abbreviations: min, minimum; max, maximum; plb, placebo; Q1, first quartile; Q3, third quartile; Std Err, standard error.
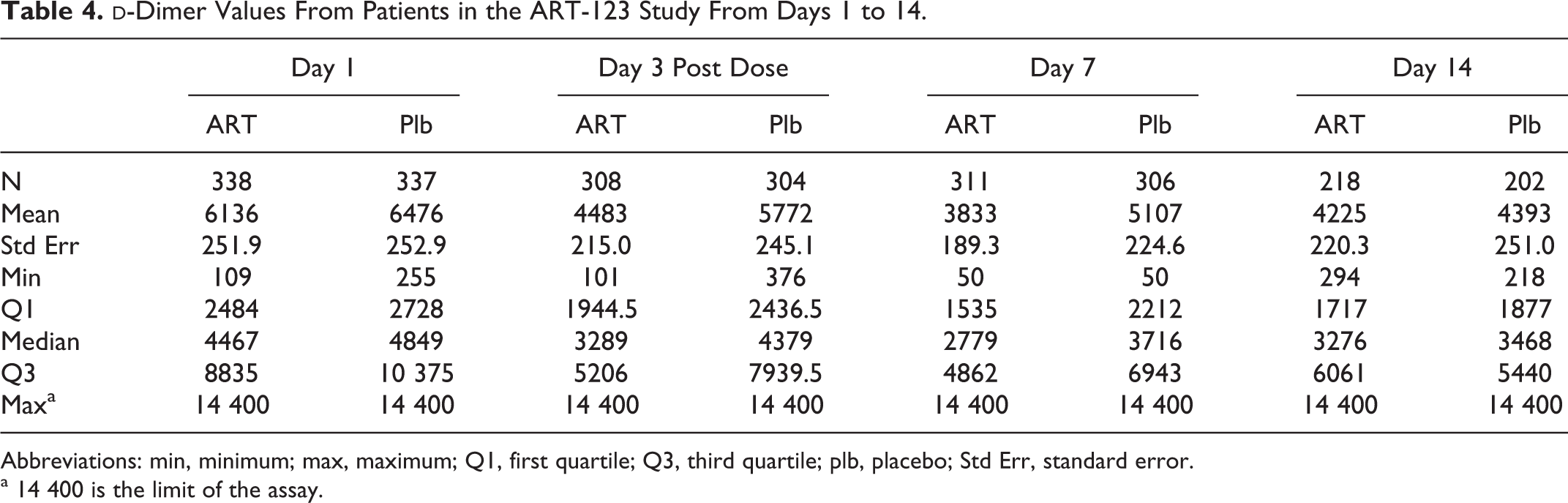
Abbreviations: min, minimum; max, maximum; Q1, first quartile; Q3, third quartile; plb, placebo; Std Err, standard error.
a 14 400 is the limit of the assay.
Table 2 and Figure 1 show the compiled F1.2 results from the ART-123-treated group and the placebo group for the duration of the study. In comparison to the controls, as displayed in Table 1, the median F1.2 levels were markedly higher and remained elevated for the entire duration of the study period. The administration of ART-123 resulted in a decrease in the F1.2 in the treatment group. The decrease was significantly different between treatment groups based upon the rank-based test (P < 0.001) for days 1, 3, and 7. No difference was observed between the treatment groups in the F1.2 at day 14. A wide scatter in the F1.2 levels in both the ART-123 and the placebo group was observed.
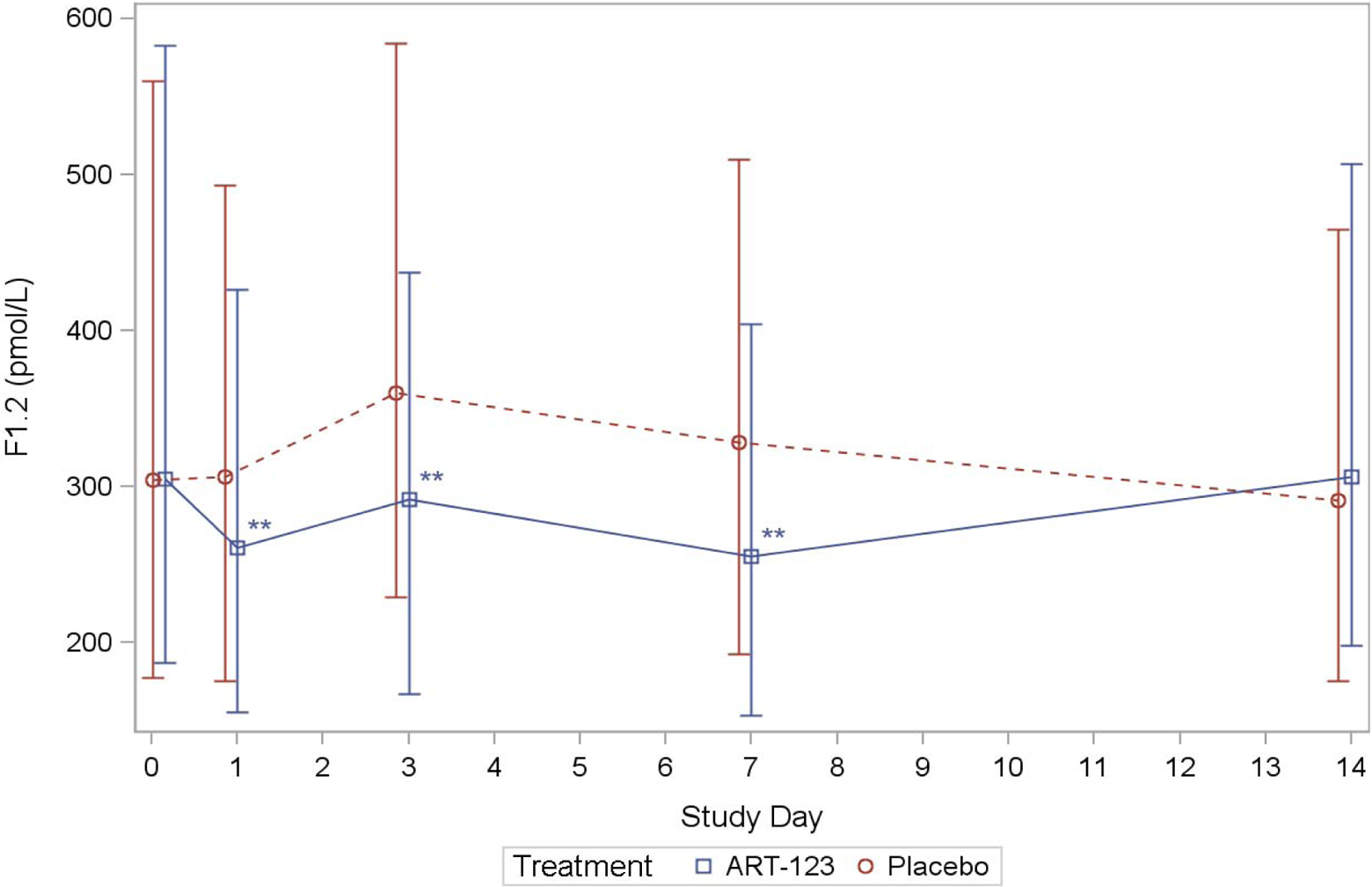
Comparison of the F1.2 levels in patients treated with ART-123 or placebo in sepsis-induced DIC. The P-value was calculated using Wilcoxon test using the change from baseline and imputing a change of zero for subjects who died. * P-value < 0.05, ** P-value < 0.01.
Table 3 and Figure 2 show the TAT values in both the treated and the placebo groups throughout the study period. Similar to the F1.2 levels, in the TAT studies the baseline samples from the placebo and ART-123 groups were 4-fold higher in contrast to the control. In the ART group the median TAT levels showed a stronger decrease in comparison to the placebo group. The decrease in the TAT level was significantly different between the treatment groups based upon the rank-based test on days 1 and 3 (P < 0.001) and on day 7 (P < 0.05). On day 14, there was no difference in the TAT levels between the groups. The TAT levels remained elevated in comparison to the controls for the entire study, and wide interpatient variations were evident as shown in Table 3.
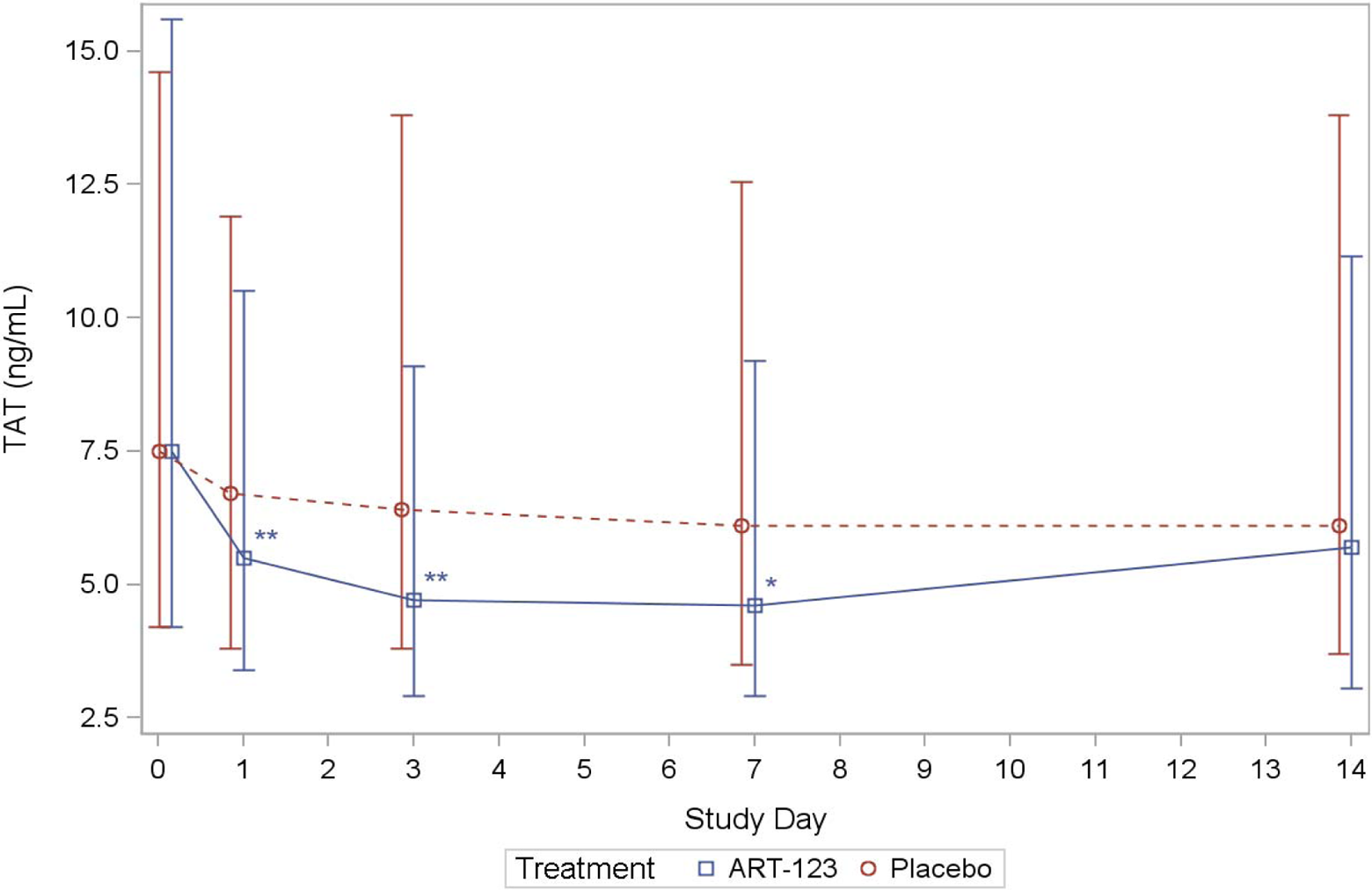
Comparison of the F1.2 levels in patients treated with ART-123 or placebo in sepsis-induced DIC. The P-value was calculated using Wilcoxon test using the change from baseline and imputing a change of zero for subjects who died. * P-value < 0.05, **P-value * 0.01.
Table 4 and Figure 3 show a comparison of the DD levels between the ART-123 and placebo groups throughout the study. The DD levels remained elevated throughout the study in comparison to the controls. In the ART-123 group, the median DD levels showed a stronger decrease in comparison to the placebo group. The decrease was significantly different between the treatment groups on days 1, 3, and 7 based upon the rank-based test (P < 0.001). Similar to the other parameters, there was wide variations observed in the DD levels. On day 14, the median DD levels were similar in both the treatment groups. These data show that both the thrombin generation markers and the DD were elevated in the placebo group during the entire study.
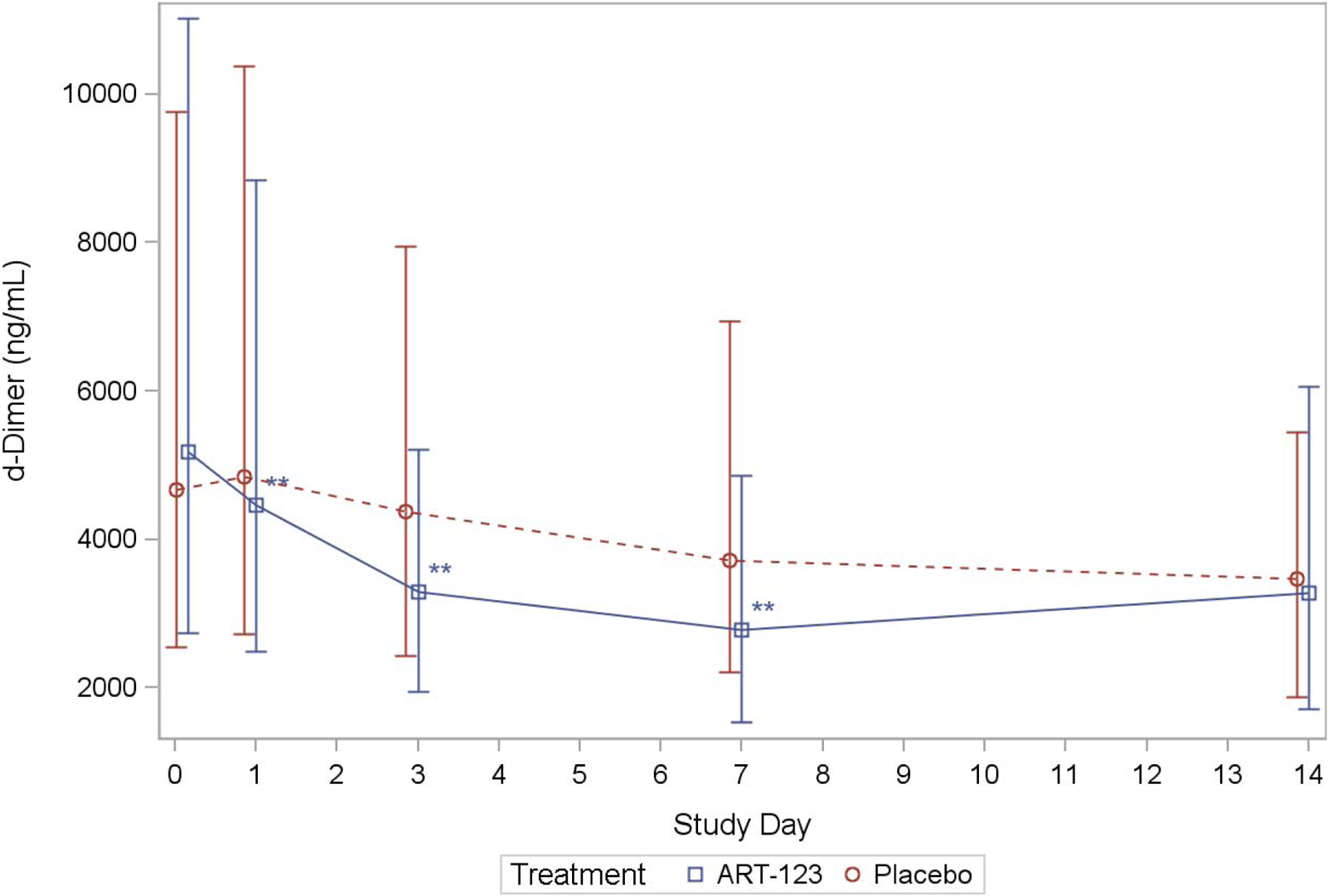
Comparison of the D-Dimer levels in patients treated with ART-123 or placebo in sepsis-induced DIC. The P-value was calculated using Wilcoxon test using the change from baseline and imputing a change of zero for subjects who died. *P-value < 0.05, **P-value < 0.01.
Discussion
Thrombin generation and dysregulation of fibrinolysis is a hallmark of sepsis-associated coagulopathy.
1
–8
These studies were carried out to determine the levels of thrombin generation markers, in particular the F1.2 and the TAT in patients enrolled in the ART-123 study.
12
In addition, the DD levels were measured to determine the extent of fibrin degradation in these patients. Since the ART-123-treated group was compared to the placebo group, the cumulative difference between these markers in the 2 groups may provide some insight into the therapeutic action of ART-123. In comparison to the control group without sepsis, the study group baseline levels of these markers, in both the ART-123-treated group and the placebo-treated group, were markedly elevated. The baseline values in the 2 treatment groups of the ART-123 study did not differ. Although the trend remained higher than the controls for all of these markers in the ART-123 group throughout the study, a comparison of the levels for all the 3 markers between the treatment arms showed a larger decrease in the ART-123 group through day 7, which was not apparent on day 14. The results on day 14, where there was no apparent difference between the levels of these markers in placebo and ART-123-treated groups, are likely due to the informative missing data introduced by patient death or recovery resulting in hospital discharge and the recovery from sepsis-associated activation of the generation of thrombin. Despite the data being widely scattered with large variability and the presence of missing data, the P values indicate that the differences in the rates of decline between the treatment groups are larger than one would expect from the random chance alone. This indicates that the differences are most likely a result of the intervention (ie treatment). The time course plots for the F1.2, TAT, and DD, for the 14 day period, showed a rapid decrease in TAT and F1.2, whereas it was gradual in the case of DD. This result can be explained with the pharmacokinetic/pharmacodynamic profile of ART-123. When ART-123 was dosed with 0.06 mg/kg/d for 6 consecutive days, the plasma concentration of ART-123 exceeded 500 ng/mL immediately after the first dose and reached its maximum concentration of 1600 ng/mL on day 6.
14
In the phase 1 study, a close correlation between a plasma concentration of ART-123 and an inhibition of prothrombinase activity was observed, in which ART-123 more than 200 ng/mL exhibited
The gradual decrease in the DD level is consistent with this observation and points to the fact that lower fibrin levels were endogenously formed following the inhibition of the thrombin generation in the ART-123-treated group. Therefore, these studies validate the hypothesis that modulation of the thrombin generation processes may play an important regulatory role in the pathogenesis of sepsis-associated coagulopathy. These data also suggest that TM downregulates the thrombin generation markers in sepsis-associated DIC.
Sepsis-associated coagulopathy is a complex syndrome in which inflammation-mediated activation of coagulation further augments the pathogenic process. Thrombin generation is central to the adverse outcomes in this syndrome. 16 Although, several therapeutic approaches were investigated in the management of this syndrome including activated protein C and antithrombin III, only limited benefits have been noted. 17,18 The ART-123 exhibits both antiinflammatory and thrombin modulatory activities. 19 The studies reported in this manuscript provide data on the increased generation of thrombin in sepsis-associated coagulopathy and its modulation by ART-123. These results suggest that ART-123 is potentially capable of controlling thrombin generation by inhibiting the thrombin generation triggered by sepsis-associated inflammatory processes. The ART-123, a soluble thrombomodulin, has multiple mechanisms of action that restores the microcirculation in severe sepsis. Especially, antiinflammatory mechanisms such as inhibition of high mobility group box 1 activity via the lectin-like domain and activation of thrombin-activatable fibrinolysis inhibitor are unique to TM compared to activated protein C. It has been reported that these unique pathways may be important to control the disease progress in severe sepsis. 19
Since ART-123 is in clinical use in Japan for the management of DIC with positive outcomes, these studies warrant additional clinical validation trials to prove the therapeutic efficacy of ART-123 in this indication. Therefore, a global phase 3 study on 800 patients is underway, and details of this study are available on the clinical trials Web site. 20
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K. Tsuruta, I. Kaul and Y. Osawa are all employees of Asahi Kasei Pharma American Corporation, of which former body, Artisan Pharma Inc., sponsored the phase 2b study of ART-123.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from Asahi Kasei Pharama American Corporation to carry out the investigation.