
Abstract
Background
The risk of venous thromboembolism (VTE) among patients with atopic dermatitis (AD), especially when receiving treatment with Janus kinase inhibitors (JAKi), has been reported in observational studies. however, the causal relationships between them remain unclear. We aim to explore the causal effects of AD and JAKi on VTE, including deep vein thrombosis (DVT) and pulmonary embolism (PE).
Methods
Two-sample Mendelian randomization (MR) analyses were conducted to examine the causal between genetic susceptibility to AD or JAKi target genes (including JAK1, JAK2, JAK3 and tyrosine kinase 2 [TYK2]) and VTE (encompassing DVT and PE) using summary statistics from genome-wide association studies and eQTLGen project. Inverse variance weighting with random effect method was used as the main analytic approach. Pleiotropy and heterogeneity tests were conducted to assess the robustness of the findings.
Results
No significant causal effects were found between AD and the risk of (odds ratio [OR]: 0.97, 95% confidence interval [CI]: 0.91-1.03, P = .352), DVT (OR: 0.99, 95% CI: 0.89-1.10, P = .789), and PE (OR: 1.06, 95% CI: 0.93-1.20, P = .387). Similarly, there was no causal association between the expression of JAK1, JAK2, JAK3 or TYK2 and VTE, DVT and PE.
Conclusion
The MR analysis revealed no genetic causal relationships between either AD or JAKi target genes and VTE. These findings may provide a reference for clinicians in prescribing JAKi for patients with AD.
Summary Table
What is known about this topic?
The association between atopic dermatitis (AD) and venous thromboembolism (VTE) was conflicting according to available research studies. Evidence from observational studies regarding the association between Janus kinase inhibitors (JAKi) and VTE also remains controversial.
What does this paper add?
There were no significant causal effects of AD on VTE. No significant causal effects of JAKi target genes on VTE were also observed. These findings may provide a reference for clinicians in prescribing JAKi for patients with AD.
Introduction
Atopic dermatitis (AD) is one of the most common chronic immune-mediated inflammatory dermatosis, affecting up to 10% of adults and 20% of children globally. 1 Adults with AD may experience recurrent eczematous lesions and intense pruritus, impairing life quality.2,3 The pathogenesis of AD involves genetic predisposition, immune dysregulation, skin barrier dysfunction and microbiome abnormalities. 4 Increasing evidence suggests that AD is a systemic disorder, associated with an increased risk of cardiovascular diseases, including stroke, myocardial infarction and heart failure.5,6 Some systemic immunomodulatory agents that are used in the treatment of AD have achieved favorable clinical outcomes in clinical trials, including Janus kinase inhibitors (JAKi). 7
Venous thromboembolism (VTE), comprised of deep vein thrombosis (DVT) and pulmonary embolism (PE), is a complex circulatory disease with genetic determinants, 8 associated with high recurrence rates and mortality.9,10 Recent genome-wide association studies (GWAS) have identified some genetic variants of immune-mediated inflammatory diseases, with well characterized effects on influencing the development of VTE. 11 Despite efforts in epidemiologic studies to investigate the potential associations of AD with VTE, the results were inconsistent.12–14 In addition, the US Food and Drug Administration issued a black box warning about an increased risk of blood clots for JAKi therapy in treating chronic inflammatory conditions. 15 While the meta-analyses did not identify a significant increase in the risk of VTE in dermatology patients receiving JAKi.15,16 Furthermore, the risk of VTE among patients with AD and the corresponding safety profile of JAKi was unclear.
Mendelian randomization (MR) is a genetic method for causal inference that emulates the design of randomized controlled trials, demonstrating effectiveness in recent years. 17 It utilizes genetic variants, such as single-nucleotide polymorphisms (SNPs), as instrumental variables (IVs) to deduce causal relationship between exposure and outcome. 18 MR analysis relies on the random assignment of genetic variants during meiosis, which effectively avoids the influence of confounders and minimizes the chance of reverse causality. 19
In this study, we performed a two-sample MR study to clarify the causal effects of AD and JAKi on VTE, including PE and DVT.
Materials and Methods
Study Design
Based on publicly available GWASs summary statistics, we performed a two-sample MR analysis to infer the causal relationship between genetic susceptibility to AD or JAKi target genes (including JAK1, JAK2, JAK3 and tyrosine kinase 2 (TYK2)) and VTE (including DVT and PE). SNPs were estimated as valid IVs. The IVs had to fulfil three fundamental assumptions of MR analysis: (i) significantly associated with exposure in interest; (ii) independent of any potential confounders; (iii) influence the outcome only via exposure. 18 An overview of the study design is shown schematically in Figure 1. All included GWAS studies in our analysis were approved by their respective ethical standards committees. This study was conducted according to the STROBE-MR guidelines.

Mendelian randomization study design. GWAS, genome-wide association study; SNP, single nucleotide polymorphism; AD, atopic dermatitis; VTE, venous thromboembolism; PE, pulmonary embolism; DVT, deep venous thrombosis; MR, Mendelian randomization.
Genetic Variants Associated with Exposure
The IVs for AD were derived from the Early Genetics and Lifecourse Epidemiology (EAGLE) Eczema consortium's GWAS, encompassing 20 population-based cohorts and involving 10,788 cases and 30,047 controls of European ancestry exclusively. 20 GWAS datasets were available from the IEU Open GWAS project (https://gwas.mrcieu.ac.uk). We also obtained cis-expression quantitative trait loci (cis-eQTLs) for JAKi target genes expression (JAK1, JAK2, JAK3 and TYK2) from the eQTLGen project (n = 31 684) (https://www.eqtlgen.org/cis-eqtls.html). 21
Genome-Wide Association Studies Summary Data for Outcome
GWAS datasets used for VTE, DVT, and PE were extracted all from the FinnGen biobank (https://www.finngen.fi/en): VTE (I9_VTE: 9176 cases and 209,616 controls), DVT (I9_PHLETHROMBDVTLOW: 4576 cases and 190,028 controls), and PE (I9_PULMEMB: 4185 cases and 214 228 controls). 22 There was no overlap in the selection of populations between the exposure groups and the outcome groups. The details of all GWASs included in our study were shown in Table 1.
Details of GWASs Included in the Mendelian Randomization.
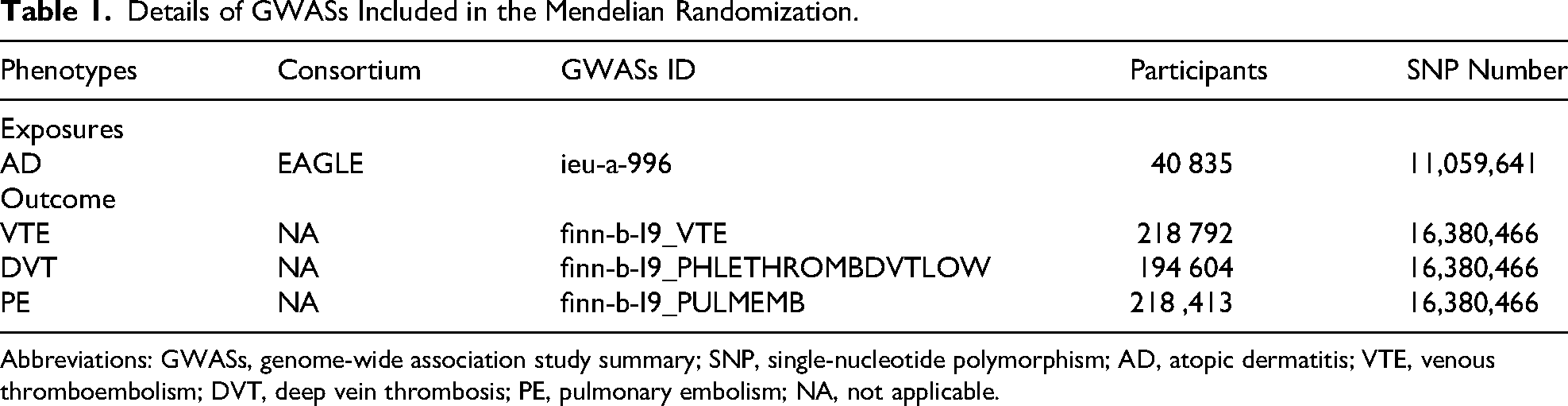
Abbreviations: GWASs, genome-wide association study summary; SNP, single-nucleotide polymorphism; AD, atopic dermatitis; VTE, venous thromboembolism; DVT, deep vein thrombosis; PE, pulmonary embolism; NA, not applicable.
Selection of Instrumental Variables
To extract the SNPs associated with the exposures robustly, we set a threshold limit of P < 5 × 10−8, a linkage disequilibrium (LD) r2 < 0.001 and a clump window size of 10,000 kb. The strength of IVs was evaluated using the F-statistic, which is calculated by the following formula: F = (β/SE)2. 23 SNPs with an F-statistic of <10 were removed, which suggests the weak IV. 24 The effect allele across the GWASs of exposure and outcome were harmonized. SNPs, characterized by inconsistent alleles or palindromic sequences, were removed from the analysis. In addition, SNPs absent in the outcome datasets were not substituted with proxy variants. We removed potential pleiotropic SNPs by the MR Pleiotropy RESidual Sum and Outlier (MR-PRESSO) method. SNPs with significant P-value for MR-PRESSO global test (<0.05) were considered as outliers and were removed prior to each MR analysis.
Statistical Analyses
Five classic MR methods were used for analysis in our study, including inverse variance-weighted (IVW), weighted median, MR-Egger, weighted mode and simple mode. The multiplicative random-effect IVW method was used as the main MR analysis with the other four methods serving as complements, as these four approaches could provide more robust estimates in a broader set of scenarios but are less efficient. 25 When only one genetic instrument was available, the Wald method was applied to estimate the causal relationship between the exposure and outcome. 26 The odds ratios (ORs) or β coefficient and 95% confidence intervals (95% CIs) were used to describe the MR results.
Heterogeneity was assessed using Cochran's Q test from the IVW approach, with a P-value <.05 indicating the presence. Funnel plots were generated for visualizing the heterogeneity of IVs. In addition, the intercept of the MR-Egger regression was used to assess directional pleiotropy. Finally, we performed a leave-one-out sensitivity analysis to evaluate whether a single SNP drove or biased the MR estimate. All analyses were performed using the “TwoSampleMR” and “MRPRESSO” packages in R (version 4.2.3).
Results
Selection of Instrumental Variables
In the MR-PRESSO method for analysis of AD on VTE, rs12144049 and rs8066625 were identified as outliers and removed. In total, 10 SNPs were ultimately selected as IVs for analysis of AD on VTE, 12 SNPs for analysis of AD on DVT and 12 SNPs for analysis of AD on PE. In the eQTLGen summary data, we obtained 5 significant cis-eQTLs derived from whole blood expression for JAKi target genes. The final SNPs for MR analysis are listed in Supplementary Table 1 and 2.
Causal Effects of AD on VTE
Figure 2 shows the estimates of the effects for AD on VTE, DVT and PE. The random-effects IVW method showed no significant association between AD and the risk of VTE (OR: 0.97, 95%CI: 0.91-1.03, P = .352), DVT (OR: 0.99, 95% CI: 0.89-1.10, P = .789), and PE (OR: 1.06, 95% CI: 0.93-1.20, P = .387). Cochran's Q statistical test showed no heterogeneity in the results of AD on VTE, DVT and PE (all P > .05). All P-values of MR–Egger intercept tests were >0.05, indicating the absence of horizontal pleiotropy (Table 1). Additionally, the leave-one-out analysis showed that effect estimates were not affected by individual SNP (Figure S1). Scatter plots are shown in Figure S2.

The genetic association of AD with VTE/DVT/PE. AD, atopic dermatitis; VTE, venous thromboembolism; DVT, deep vein thrombosis; PE, pulmonary embolism; MR, Mendelian randomization; IVW, inverse variance weighted.
Causal Effects of JAKi on VTE
We conducted MR analysis on the blood expression data of 4 JAKi target genes and 3 VTE outcomes, respectively (for all results, see Figure 3). No significant association of JAK1, JAK2, JAK3 and TYK2 on VTE, DVT and PE was observed (all P > .05). Due to the limited SNPs, the Cochran Q test and the MR–Egger intercept test were not performed. (Table 2).

The genetic association of JAKi with VTE/DVT/PE. JAK1, Janus Kinase 1; JAK2, Janus Kinase 2; JAK3, Janus Kinase 3; TYK2, Tyrosine Kinase 2; VTE, venous thromboembolism; DVT, deep vein thrombosis; PE, pulmonary embolism; MR, Mendelian randomization; IVW, inverse variance weighted.
The Results of Heterogeneity and Pleiotropy Between Exposure and Outcome.

Abbreviations: AD, atopic dermatitis; VTE, venous thromboembolism; DVT, deep vein thrombosis; PE, pulmonary embolism.
Discussion
In this study, we firstly explored the genetic causal effects of AD and JAKi on the risk of VTE by a two-sample MR analysis based on summary statistics from eQTL data and GWAS summary data. Our findings did not yield evidence of a significant causality for AD on VTE from a genetic standpoint. Additionally, we did not find a significant association between JAKi target genes and VTE.
In contrast with recent systematic review of observational studies suggesting that AD was statistically associated with increased risk of VTE, our MR findings did not support the causal association of AD on VTE.14,27 The discrepancy between the results of our analysis and previous studies may be partly explained by the following reasons. Firstly, these studies were hindered by inadequate consideration of important confounders, such as hormone therapy and smoking status.28,29 Besides, the previous systemic reviews included limited number of studies and small sample sizes.14,15 MR can eliminate the impacts of confounding bias and reversal causality by employing randomly allocated genetic variants as IVs to make reliable causal inferences. 30 Moreover, MR analysis based on the large GWAS datasets was performed in this study. To mitigate bias and bolster the robustness of our MR results, we devised a succession of sensitivity analyses. These findings indicate that, although diverging from some prior observational studies, our results and conclusions drawn from the MR study were credible. While our MR study did not find evidence supporting a genetic causal effect of AD on VTE, it remains possible that AD could influence the onset or progression of VTE. The pathophysiologic mechanism linking AD and VTE remains unknown but may be related to AD's impact on the three classical mechanistic pathways contributing to the risk of thrombosis, including Endothelial injury, venous stasis, and hypercoagulability. 31 Active systemic inflammatory mediators and cytokines, including interleukin (IL)-6 and monocyte chemotactic protein-1, can modulates thrombosis and affect hypercoagulability.32,33 Additionally, inflammatory cytokines in AD, such as IL–4 and IL-13, may interact with coagulation cascades in animal models.34,35 More research is needed to thoroughly explore the potential association between AD and VTE, delving into greater depth.
Consistent with recent systematic reviews, we did not find any significant impact of the expression of all JAKi target genes on the risk of VTE, DVT, and PE.16,36 Our MR analysis estimates the effect of target genes associated with drug action, rather than the direct effect of drug use on diseases. This method is robust and has been widely applied to evaluate the association between antihypertensive drug target genes and psychiatric disorders, as well as to assess the impact of metformin targets on the risk of cardiovascular diseases and cancer.37,38 Additionally, to enhance the validity and reliability of the findings, we established strict criteria for the selection of IV. The boxed warning has been issued for multiple medications that target the JAK-STAT signaling pathway, as the ORAL Surveillance study highlighted safety concerns of JAK inhibitors and found an increased risk of VTE. 39 It is noteworthy that the majority of major adverse cardiovascular events and VTE have been observed in rheumatoid arthritis individuals with pre-existing cardiovascular risk factors, including hypertension, dyslipidemia, and diabetes mellitus. Another study showed that the incidence rates of VTE with JAK inhibitors were lower for patients with fewer cardiovascular risk factors across conditions. 40 It seems that populations with low cardiovascular risk have low incidence of the examined JAKi-related VTE. Therefore, the connection between JAK inhibitors and the risk of VTE might be due to factors beyond the diseases themselves, which is in line with our MR findings. In clinical practice, it is likely appropriate to consider an individualized approach to VTE risk management for patients who may benefit from JAK inhibitors. 41
There are limitations to this study. First, the predominantly European-descent population in the GWAS for the MR study reduced the impact of population stratification bias, but this limited the broader applicability of our findings. Second, in our analysis of JAKi, we were constrained to examining expression data from whole blood samples due to limitations in the available data. Finally, the lack of individual-level genotyping data hindered the assessment of causal effects of AD and JAKi on VTE across various age groups and genders.
Conclusion
This is the first MR study to elucidate the genetic causal effect of AD and JAKi on VTE. In this study, no genetic causal relationships were observed between either AD or JAKi target genes and VTE, encompassing DVT and PE. These findings may provide a reference for clinicians in prescribing JAKi for patients with AD. However, these results need to be further confirmed by well-designed prospective clinical studies.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251413253 - Supplemental material for Association of Venous Thromboembolism Risk with Atopic Dermatitis and Janus Kinase Inhibitors Treatment: A Mendelian Randomization Study
Supplemental material, sj-docx-1-cat-10.1177_10760296251413253 for Association of Venous Thromboembolism Risk with Atopic Dermatitis and Janus Kinase Inhibitors Treatment: A Mendelian Randomization Study by Zhiqiang Chen, MS, Shuaibo Wang, and Yifei Wang, PhD in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgements
We extend our sincere gratitude to all participants and researchers who contributed to the corresponding GWAS for their commitment to sharing summary-level data publicly.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Authors’ Contribution
Y. W., Z.C., and S.W. contributed to the conception or design of the work. Y.W. and Z.C. contributed to the acquisition, analysis, or interpretation of data for the work. S.W. wrote the first draft of the manuscript with critical revisions from Y.W. and Z.C. All gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Program of Anhui, (grant number AHWJ2024BAc30041).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data used in the present study had been publicly available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.