
Abstract
Objective
To explore the impact of physical restraint (PR) on the occurrence of venous thromboembolism (VTE) in stroke patients.
Methods
Totally 321 stroke patients were randomly enrolled and categorized into 2 groups according to whether PR was used or not. Moreover, the effect of PR on VTE in stroke patients was explored, and the independent influencing factors for the occurrence of VTE in stroke patients were also identified.
Results
Among the enrolled patients, 68 cases (21.18%) developed VTE, including 60 with muscular calf vein thrombosis, 6 with great saphenous vein thrombosis, and 2 with deep vein thrombosis (DVT). Of these 68 patients, 49 had cerebral infarction and 19 had intracerebral hemorrhage (ICH). Also, there were 39 patients (39/96) developing VTE with PR, and 29 (29/225) developing VTE without PR. Through analyzing the relationship between the incidence of VTE in stroke patients and clinicopathological parameters, it was discovered that diagnose (χ2 = 33.058 P = 0.000), history of diabetes (χ2 = 12.80 P = 0.000), muscle strength (χ2 = 21.608 P = 0.000), activity of daily living (ADL) (χ2 = 41.952 P = 0.000), and PR (χ2 = 31.004 P = 0.000) were significantly correlated with the occurrence of VTE. Moreover, as revealed by multivariate analysis of variance ICH (OR 4.485 (1.653–12.169), P = 0.003), previous history of diabetes (OR 2.511 (1.257–5.018), P = 0.009), low ADL (OR 0.208 (0.109–0.397), P = 0.000), and PR (OR 5.048 (2.520–10.113), P = 0.000) were the independent risk factors for VTE in stroke patients, while muscle strength (OR 0.679 (0.366–1.259), P = 0.219) had an impact on the occurrence of VTE, but was not an independent risk factor.
Conclusion
This treatment center can lower the occurrence of VTE by standardizing the use of PR. Meanwhile, for the patients with ICH who have a history of diabetes and poor ADL, more education and care should be provided to minimize the occurrence of VTE.
Introduction
Stroke is a common neurological disorder, which can be classified into ischemic stroke and hemorrhagic stroke. It occurs when the blood flow to a certain part of the brain significantly decreases or when there is intracranial arterial bleeding, resulting in the sudden impairment of brain function. 1 In general, stroke refers to a group of cerebrovascular diseases caused by organic brain injuries, 2 and is associated with the high incidence rate(276.7/100,000), high prevalence rate (2022.0/100,000), high mortality rate(153.9 /100,000), and high economic burden (2412.5/100,000).3,4 It is characterized by rapid onset, multiple complications, and a high economic burden. Stroke is the leading cause of disease-related mortality among Chinese residents. 5 Patients with stroke are prone to venous blood stasis due to prolonged bed rest, restricted movement, and increased prothrombin activity. Additionally, vascular endothelial damage caused by cerebrovascular diseases or central nervous system disorders can result in a hypercoagulable state of the blood, often resulting in venous thromboembolism (VTE). 6
VTE encompasses deep vein thrombosis (DVT) and pulmonary embolism (PE), and it ranks third among cardiovascular diseases worldwide. It is also one of the common and serious complications in patients with stroke. According to surveys, the incidence of DVT in stroke patients ranges from 4.80%–45.00%, 7 while that of PE is 0.50%–5.00%. 8 These conditions have posed significant threats to the health and life of patients. VTE is regarded as a significant potential preventable cause of death. However, its insidious onset and inconspicuous clinical symptoms in stroke patients may result in a higher probability of misdiagnosis and missed diagnosis, thereby increasing the unexpected mortality rate.9,10 Therefore, the early assessment and prevention of VTE in stroke patients are of vital importance for reducing the mortality and disability rates and enhancing the patients’ life safety.
Physical restraint (PR) represents the use of any physical or mechanical equipment, materials, or tools attached to or close to the body of the patient, or the use of facilities that restrict the patient's free physical movement, or restrict physical movement to a desired position or to prevent the patient from properly accessing the body. 11 It is an important medical auxiliary measure for stroke patients, with a clinical use rate of 39.9%–84.7%. It helps control the behavior of patients with delirium and agitation, protect the safety of patients, and avoid unplanned extubation and falls. However, unreasonable PR can cause psychological and physiological complications in patients.12,13 As reported in some recent studies, factors like D-dimer, homocysteine and age affect the occurrence of VTE, while the effect of PR on the occurrence of VTE in stroke patients has rarely been reported. Consequently, this study aimed to recruit clinical cases from the treatment center of our hospital, analyze the impact of PR on the occurrence of VTE in stroke patients, further analyze its independent risk factors, and optimize the clinical practice of our hospital.
Data and Methods
General Information
Totally 321 inpatients who visited the Neurology Departments of our hospital from October 2024 to April 2025 were randomly selected.
The inclusion criteria in this study were as follows: (1)Patients confirmed by imaging examinations and meeting the diagnostic criteria for stroke 14 ; (2)The first-onset patients; (3)Those providing informed consent.
The exclusion criteria included: (1)Those with mental disorders; (2)Those with impaired functions of important organs; (3)Those with incomplete clinical data; (4)Those with a history of thrombosis; (5)Those using sedative drugs.
Basic information such as age, gender, past medical history (hypertension and diabetes), diagnosis, muscle strength, Barthel score, and D-dimer of patients was recorded. Muscle strength was evaluated by manual muscle testing (MMT) (0: no muscle contraction; 1: palpable muscle contraction but unable to cause joint movement; 2: able to perform gravity-resistant movement, with joint range of motion < 50%; 3: able to perform 100% full-range joint movement but unable to resist resistance; 4: joint range of motion of 100%, and able to resist moderate resistance; and 5: joint range of motion of 100%, with normal muscle strength). Barthel score was assessed using the activity of daily living (ADL) scale, with a total score of 100 points. To be specific, 0–40 points indicate severe dependence, 41–60 points suggest moderate dependence, and 61–100 points represent mild dependence.
Research Methods
All patients were divided into 2 groups based on whether they were physically restrained. Besides, they received daily care from nurses at the level of chief nurse or above in our hospital. The specific contents included general care (position management, diet and nutrition, rest and activity), medication care (adherence to the doctor's instructions for medication), and health education (ankle pump exercises, and functional exercises). For patients with PR, the attending physician and the responsible nurse jointly evaluated their consciousness, muscle strength, behavior, and treatment/equipment conditions, so as to determine whether PR was necessary.
The restraint adaptations included: 1)Patients exhibiting scratching or self-tube-pulling behaviors; 2)Patients being agitated or having aggressive behaviors; 3)Patients using life-supporting treatments/equipment and having agitated and aggressive behaviors.
For patients meeting the restraint criteria, the restraint-related contents were informed to the patients, their guardians or proxies before the PR was carried out. After a joint decision and signature of the “Safety Notification Form”, the PR was performed. The tightness of the restraint should be appropriate to accommodate 1–2 fingers. After the patients were restrained, the looseness of the restraint belt, local skin color, temperature, and local blood circulation were dynamically observed. If any abnormalities occurred, the doctor was promptly notified for handling, and hydrocolloid dressings were provided for protection. To ensure the homogeneity of the restraint methods, the PR methods for patients were chosen based on the “Inpatient Body Restraint Nursing Standards”, and the appropriate restraint tools and methods were selected in accordance with the patient's condition. In this study, the PR for patients was limb restraint. The upper limb restraint tools included restraint belts + restraint gloves (Figure 1), and the lower limb restraint tools were restraint belts (Figure 2). Five days after admission, all patients underwent routine duplex venous and arterial ultrasound examinations of both lower extremities to confirm the presence of VTE. Additionally, during their hospital stay, the responsible nurses conducted routine daily checks on the patients’ lower extremities for signs of edema, redness and so on. Once any of these symptoms were detected, another duplex venous and arterial ultrasound examination would be immediately conducted to confirm the diagnosis.This project was approved by the Ethics Committee of Jiangsu University Affiliated Jurong Hospital (Approval Reference Code: JRH-IEC-2025008), and all patients and their families obtained informed consent.

Upper limb restraint.

Lower limb restraint.
SPSS23.0 (IBM SPSS Statistics Armonk, NY: IBM Corp) software was used to carry out all statistical analysis. The χ2 test was used to analyze the effect of PR on the occurrence of VTE, and logistic regression was used to conduct univariate analysis of the influencing factors of VTE in stroke patients, and multivariate analysis of the influencing factors of VTE occurrence was carried out using logistic regression. The odds ratio (OR) of each factor was calculated. All data were calculated for the OR value and the confidence interval (CI) at the 95% confidence level.Two-sided significance tests were used with α = 0.05, unless otherwise indicated, and P < 0.05 was considered to indicate statistically significant test results.
Results
Baseline Data
In total, 344 patients were enrolled. Among them, 3 patients died, 7 dropped out of treatment, and 12 had incomplete data. Eventually, 321 patients were included, including 225 (70.1%) not using PR, while 96 (29.9%) using PR. The specific information of these 321 patients is shown in Table 1.
Patients’ Information.
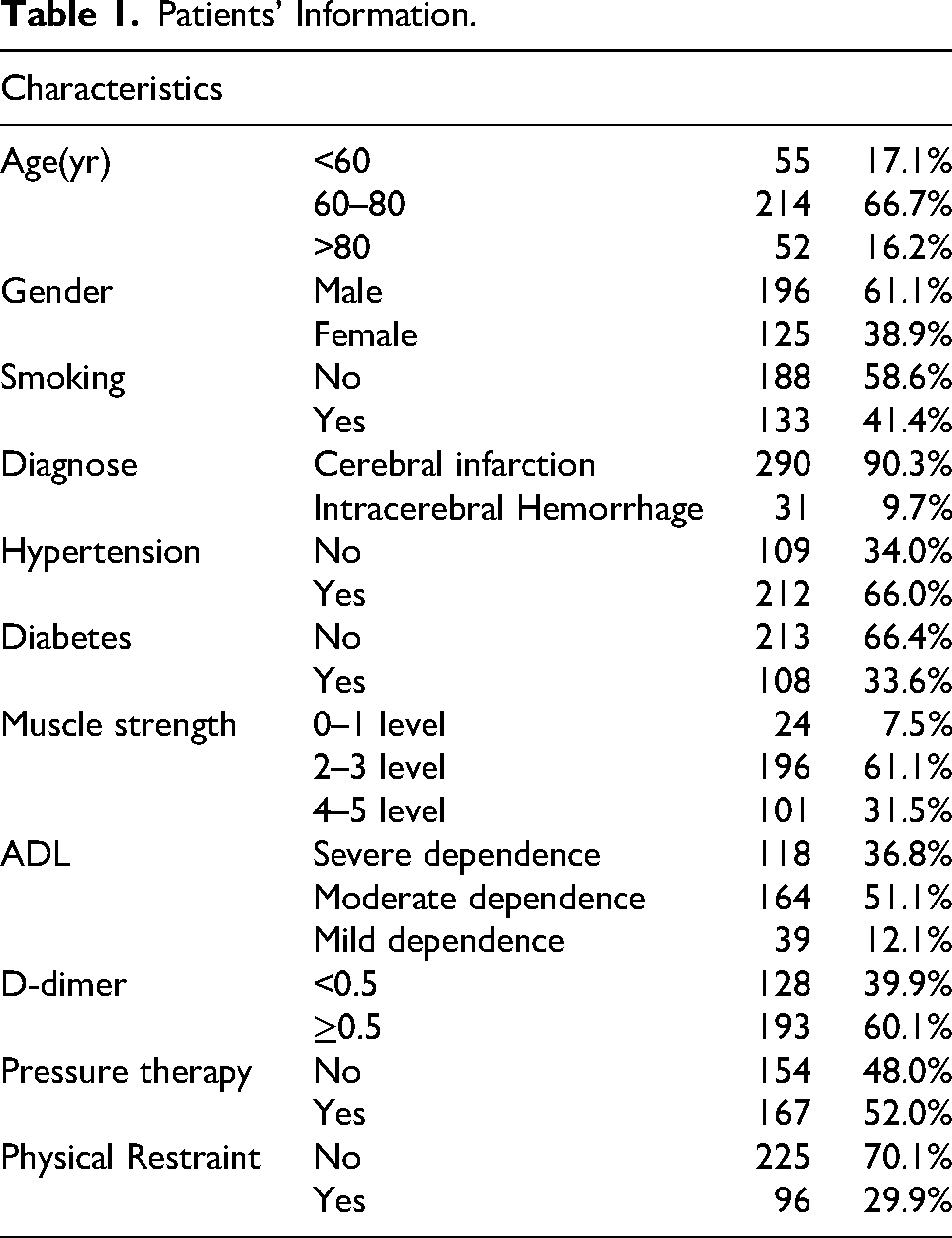
Patients’ Information.
Of the enrolled patients, 68 cases had VTE (including 60 with muscular calf vein thrombosis, 6 with great saphenous vein thrombosis, and 2 with DVT), 49 people are patients with cerebral infarction, and 19 have intracerebral hemorrhage (ICH). There were 29 patients (29/225) with VTE in the non-restraint group, and 39(39/96) in the restraint group. Through analyzing the association between the occurrence of VTE and clinicopathological parameters, it was found that diagnosis (χ2 = 33.058 P = 0.000), history of diabetes (χ2 = 12.80 P = 0.000), muscle strength (χ2 = 21.608 P = 0.000), ADL (χ2 = 41.952 P = 0.000), and PR (χ2 = 31.004 P = 0.000) were significantly related to the occurrence of VTE. While age, gender, smoking history, history of hypertension, D-dimer, and whether undergoing pneumatic therapy were not significantly correlated with the occurrence of VTE. (Table 2)
Relationship Between Occurrence of VTE and Clinicopathological Factors.

Relationship Between Occurrence of VTE and Clinicopathological Factors.
Chi square test.
To improve the transparency and avoid selective reporting, all variables were incorporated in the multivariate logistic regression analysis. The results indicated that ICH(OR 4.485 (1.653–12.169), P = 0.003), previous history of diabetes(OR 2.511 (1.257–5.018), P = 0.009), low ADL (OR 0.208 (0.109–0.397) P = 0.000), and the use of PR(OR 5.409 (2.520–10.113) P = 0.000) were the significant independent risk factors for VTE. Moreover, muscle strength(OR 0.679 (0.366–1.259) P = 0.219) influenced the occurrence of VTE, but was not an independent risk factor. (Table 3)
The Influencing Factors of VTE Were Clarified by Multiple Logistic Regression.
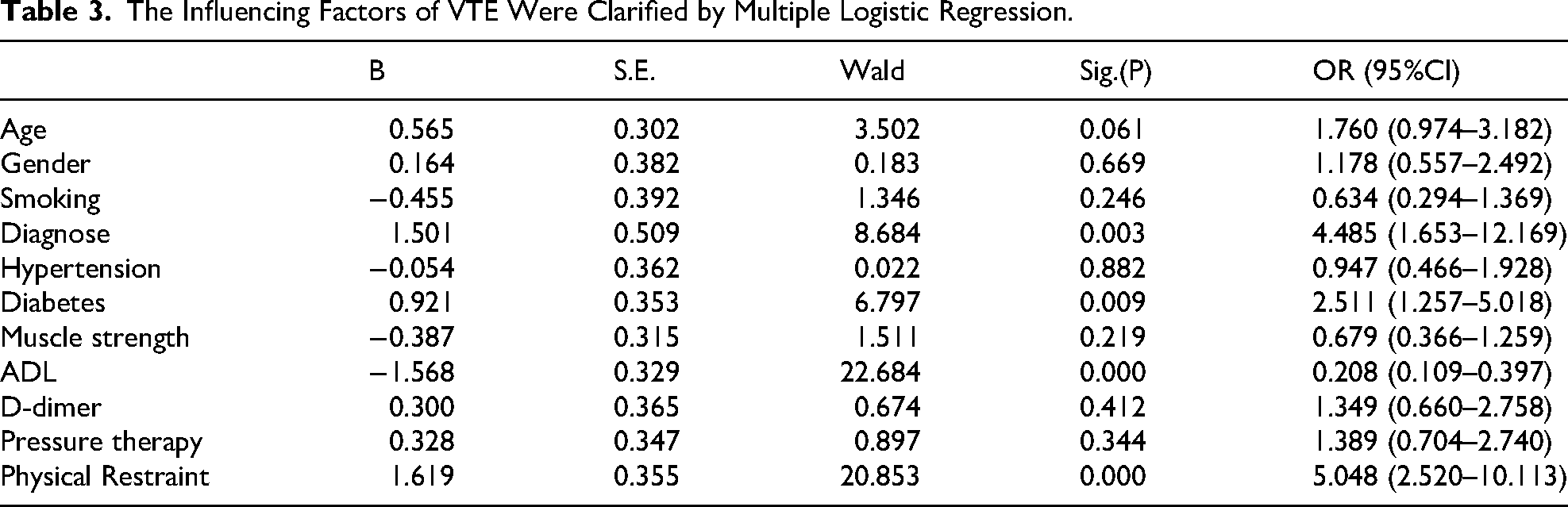
The Influencing Factors of VTE Were Clarified by Multiple Logistic Regression.
VTE is a disease where the blood in the inner part of leg veins becomes abnormally coagulated due to various factors, forming a blood clot, which leads to vascular obstruction and backflow disorders. 15 It can cause related pathological changes and clinical symptoms, such as pain and limb swelling, not only affecting the daily life activities of the patient but also influencing the prognosis of the disease. In severe cases, it may even endanger life.16,17 Patients with stroke are more prone to VTE due to various reasons like venous blood stasis, vascular endothelial damage, and hypercoagulable state of the blood. Previous studies mostly focus on the effects of D-dimer, C-reactive protein, age, and the National Institutes of Health Stroke Scale (NHISS) score on VTE in stroke patients, while there have been few reports on the impact of PR on the occurrence of VTE. In this study, 321 stroke patients were enrolled, with an incidence rate of 21.18% for VTE. As discovered by Yan D 18 in the construction of a risk prediction nomogram model for VTE formation in patients with acute ischemic stroke, the incidence rate was 22.78%, which was basically in consistence with the results of this study. In addition, Liu 19 conducted a survey on patients in the recovery period of stroke and found that the incidence rate was 34.2%, significantly higher than that reported in our study. Such discrepancy may be attributed to the different disease stages included. Meanwhile, it is also closely related to the attention of doctors and nurses in our hospital, early or ultra-early pneumatic treatment, and ankle pump exercises.
In this study, 321 stroke patients were enrolled, including 290 with cerebral infarction and 31 with ICH. Among patients with cerebral infarction, 16.89% developed VTE, which was significantly lower than that of 61.29% in ICH patients. This result was consistent with the findings of Ji R. 20 To reduce cerebral edema, patients with ICH were treated with diuretics such as mannitol, which led to blood concentration, insufficient blood volume, and increased blood viscosity, eventually resulting in a hypercoagulable state. Moreover, the long-term infusion of hypertonic fluids could cause damage to the vascular endothelium of veins, inducing platelet adhesion and aggregation on vascular walls, the release of bioactive factors, a decrease in anticoagulant activity, and abnormal fibrinolytic mechanisms, thereby promoting thrombosis. Additionally, a history of diabetes is a high-risk factor for VTE,21,22 consistent with the results of this study. Multivariate regression analysis indicated that a history of diabetes was an independent risk factor for VTE in stroke patients. The long-term hyperglycemic state would prevent red blood cells from effective aggregation or depolymerization, resulting in blood flow obstruction. Hyperglycemia would also increase the risk of atherosclerosis and the occurrence of VTE. Based on our chi-square test results, the lower muscle strength and the lower level of self-care ability were associated with the higher risk of VTE. However, multivariate regression analysis indicated that muscle weakness was not an independent risk factor for VTE (P > 0.05). Hua C 23 believed that clotting factors accumulated in stroke patients with hemiplegia owing to long-term bed rest. When the accumulation reached a certain degree, it would lead to venous dilation, vascular endothelial damage, and subsequently VTE. Warlow 24 also suggested that 60% of paralyzed patients among stroke patients had asymptomatic DVT, while the incidence rate of asymptomatic DVT in the non-paralyzed limbs was only 7%. This result was inconsistent with the findings of this study, which may be attributable to the different evaluation and classification methods of muscle strength. Hua C defined muscle strength by using the standard definition (0 level: The limb remains in the required position for 5 s without falling; 1 level: The limb falls at the end of 5 s without hitting the bed; 2 level: The limbs quickly fall onto the bed within 5 s, but can resist gravity; 3 level: The limbs fall rapidly but cannot resist gravity; 4 level: No movement; 5 level: Amputation or joint fusion), and classified muscle strength as normal (0–2 levels) and hemiplegic (3–5 levels). This might have led to a certain degree of deviation in the results. In the future, the sample size will be enlarged, and the classification of muscle strength will be strictly based on the 0–5 levels to analyze the impact of muscle strength on VTE in stroke patients. Low ADL was identified as an independent risk factor for VTE (P < 0.05), consistent with the results of Zhi G's study. 25 ADL includes activities such as independent eating and drinking, using the toilet, performing personal hygiene tasks, independent dressing and grooming. Stroke would cause functional limitations related to the injury. As reported in some studies, approximately 70%–80% of stroke patients have difficulty in self-care due to activity limitations. 26 Conversely, a decrease in ADL directly affects the range of movement of the patient's limbs. 27 Xiaoli W 28 found that patients with decreased ADL experienced more severe early conditions due to weakened daily activities such as sitting up and walking. Due to weakened daily activities like sitting up and walking, venous blood flow slows down, causing an increased risk of VTE. Therefore, in addition to preventing VTE for patients with decreased ADL, medical staff and caregivers should also encourage and assist patients to start rehabilitation functional exercises as soon as their condition stabilizes, aiming to lower the incidence of VTE and enhance the quality of life of patients.
Yuan Y 29 discovered that PR increased the risk of complications in patients with severe stroke. On this basis, this study randomly enrolled 321 patients with cerebral stroke and divided them into 2 groups according to whether they were restrained or not. As revealed by our results, PR was an independent risk factor for VTE in patients with cerebral stroke (P < 0.05). Currently, there are few studies concerning the impact of PR on the occurrence of VTE in patients with cerebral stroke. Erturul 30 illustrated that in the intensive care unit, the use of PR might cause redness (P < 0.001), limb movement (P < 0.001), edema (P < 0.001), and color complications (P < 0.001). PR restricts the free movement of the patient's body or a certain part of the body and the patient's touching of a certain part of their body, limiting the activity while often causing damage such as limb edema, joint dysfunction, and skin lesions at the restraint site, finally increasing the risk of VTE. Tsuda 31 investigated the occurrence of venous thrombosis in psychiatric patients using PR and proposed that mental health professionals should closely monitor the formation of DVT in mentally ill patients under PR. Therefore, it can be seen that PR is closely related to VTE. In this regard, it is necessary for medical staff to implement the minimum PR under the premise of ensuring patient safety. Relevant organizations and departments at home and abroad have formulated corresponding legal systems.11,32 It is recommended to standardize or reduce the use of PR through methods such as ①educing the use of restraint and adopting alternative measures; ②avoiding blind implementation and standardizing the use process of restraint; and ③preventing the use of restraint and strengthening organizational education and management, thereby reducing the occurrence of VTE.
Conclusion
VTE is one of the common and serious complications in stroke patients, posing significant threats to the patients and their families. With the increasing attention paid to the risk factors for VTE, a better description of biological factors will help understand the pathogenesis of VTE in stroke patients and may assist in formulating better management strategies. In our single-center study, reducing the use of PR in stroke patients may lower the incidence of VTE. Additionally, we suggest strengthening education and care for stroke patients with a history of diabetes and a poor self-care ability to reduce the occurrence of VTE.
Limitations
The study still has some limitations. Firstly, this study is based on a single treatment center, which may introduce bias. Therefore, multi-center collaborative research is needed to verify our results. Secondly, the number of stroke patients involved in this study is relatively small, and the muscle strength grouping cannot be further divided into 0–5 levels. The results still need to be further verified. Finally, the included patients only had their history of hypertension and diabetes. The relevant indicators for stroke, such as the NHISS and homocysteine were not collected. Further investigations are still needed to expand the scope and clarify the influencing factors of VTE occurrence in stroke patients.
Footnotes
List of abbreviations
Acknowledgements
This study was funded by the Natural Science Foundation of Jurong Hospital Affiliated to Jiangsu University (No: JY20231004); Supported by Jurong City Urban Social Development Project (ZA42112).
Ethics Approval
Ethical approval to report this case was obtained from the Ethics Committee of Jiangsu University Affiliated Jurong Hospital (Approval Reference Code: JRH-IEC-2025008).
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Author's Contributions
YH and QW contributed equally to this work. The authors have no funding and conflicts of interest to disclose. The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. Conceptualization: Hui Yang. Yue Hu. Qin Wu. Data curation: Qin Wu. Chenlu Xu. Yan Wang. Yue Hu Formal analysis: Yue Hu. Hui Yang. Qin Wu. Funding acquisition: Hui Yang. Investigation: Yue Hu. Jianping Feng. Yi Wang. Lihua Liu. Methodology: Qin Wu. Yue Hu. Hui Yang. Project administration: Yue Hu. Jianping Feng. Yan Wang. Resources: Qin Wu. Lihua Liu Software: Yue Hu. Qin Wu. Supervision: Hui Yang. Zhangli Chen. Validation: Jianping Feng.Visualization: Hui Yang. Writing original draft: Yue Hu. Qin Wu. Writing review & editing: Yue Hu. Zhangli Chen. Qin Wu.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Jurong Hospital Affiliated to Jiangsu University, Jurong City Urban Social Development Project, (grant number JY20231004, ZA42112).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated andanalyzed during the current studyare available in the Science Data Bank, ![]() . DOI:https://doi.org/10.57760/sciencedb.27518.
. DOI:https://doi.org/10.57760/sciencedb.27518.