
Abstract
Background
Features of pulmonary embolism may be different in elderly than the in young patients. The purpose of the study is to examine the characteristics of PE in elderly and young patients.
Patients and Methods
We conducted a retrospective study by examining the digital medical records of consecutive patients (>18 years old)who underwent CTPA at our center for suspected pulmonary embolism between 2013 and 2019. We classified the patients as elderly (≥65 years) and younger group (<65).
Results
Enlarged complete artery occlusion (67.5% vs 32.1%, P = .0001), polo mint sign (47.2% vs 25.2%, P = .0001) and partial filling defect with acute angle(57.7% vs 30.5%, P = .0001) were more frequent in younger patients compared to elderly group. Shrunken complete artery occlusion (62.6% vs 32.5%, P = .0001),thickened small arteries (64.1% vs 33.3%, P = .0001),bilateral pleural effusions(16.8% vs 4.9%, P = .002),variation in the size of segmental vessels (30.5 vs 8.9, P = .0001) and mosaic perfusion pattern (55.0% vs 28.5%, P = .0001) occurred more often in the elderly group compared to younger patients. Presence of right ventricular dysfunction (RV/LV diameter ratio ≥ 1), lower oxygen saturation determined while breathing room air on admission and increased pulmonary artery diameter seem to be associated with an increased risk of in-hospital mortality in pulmonary embolism patients in logistic procedures. In another logistical procedure, age and pulmonary artery diameter are important determinants of in-hospital death in patients with pulmonary embolism.
Conclusions
The CT findings of pulmonary embolism in elderly and young patients are significantly different, with chronic features in the elderly and acute features in the younger. Age and characteristics of acute and chronic pulmonary embolism, such as a high RV/LV ratio, low oxygen saturation on admission, and an increased pulmonary artery diameter, may determine outcomes.
Introduction
Pulmonary embolism (PE) is a common and life-threatening condition in patients presenting in the emergency department and hospital with acute chest pain, dyspnea or syncope.1,2 The clinical presentation of PE may be atypical or subtle in elderly patients. 3 While the overall incidence of pulmonary thromboembolism did not change over 30 years, the rate in the population over 65 years doubled in this period. 4 The incidence of pulmonary embolism and its atypical clinical picture increase with age. 5 Physicians treating elderly patients may have difficulty diagnosing pulmonary thromboembolism because it shares similar symptoms with other conditions.6–8 Age can be a facilitator for other risk factors, such as heart failure, immobility, or malignancy, which are known to be associated with an increased risk of PE. 9 Studies in patients with PE indicated the some clinical and laboratory findings of old patients with PE were different from the younger group.10,11 Computed tomographic pulmonary angiography has been the basic test in most centers in the evaluation and management of patients with suspected pulmonary thromboembolism.12–14 Features of pulmonary embolism may be different in elderly than the in young patients. The purpose of the study is to examine the characteristics of PE in elderly and young patients.
Patients and Methods
We conducted a retrospective study by examining the digital medical records of consecutive patients (>18 years old) who underwent computed tomography pulmonary angiography at our center for suspected pulmonary embolism between 2013 and 2019. This was an observational, hospital-based study to identify the possible differences in CT features, clinical findings, comorbidity and laboratory results between the younger and elderly patients with PE.
We chose the patients with PE confirmed by CTPA in all cases registered during the study period as inclusion criterion. Patients whose CTPA results were not diagnostic were excluded from the study. In this study, we classified the patients as elderly (≥65 years) and younger <65 years).
Lower extremity compression ultrasound was performed to all patients. After injecting 50-75 mL of contrast medium containing iodine, CT angiograms were taken with the main 64-row scanners. Echocardiography, compression ultrasonography and laboratory measurements within 48 h after the diagnosis of PE were included in the analysis.
Image Analysis
The last consensus of these two chest physician was used as a reference standard for the diagnosis of PE. Pretest probability scoring (eg, Well or Revised Geneva scores) is generally not used in our center. Most pulmonary CTA examinations in our center are requested by the physician based on clinical suspicion such as acute or worsening dyspnea, pleuritic chest pain, hemoptysis, sudden fall in saturation and clinical deterioration in otherwise unexplained.
The presence of at least one filling defect in the pulmonary artery tree was defined as PE.15,16
Signs of acute PE included direct features such as enlarged complete artery occlusion, polo mint sign, railway track sign, and partial filling defect with acute angle, while indirect features comprised triangular subpleural consolidation or ground-glass opacity.
Signs of chronic PE encompassed direct features such as shrunken complete artery occlusion, partial filling defect with obtuse angles to the vessel wall, thickened small arteries leading to pulmonary artery stenosis, band/web, and intimal irregularities. Indirect features included enlargement of the main pulmonary artery, tortuous vessels, poststenotic dilatation, bronchial collaterals, nonbronchial collaterals, variation in the size of segmental vessels, mosaic perfusion pattern, bronchial dilatation, pericardial involvement, and chronic infarct appearance such as linear band or pleural nodule.17–22
In this study, the presence of two or more direct acute or chronic radiological signs was considered as acute or chronic pulmonary embolism. However, cases with acute pulmonary embolism characteristics on CT were evaluated as acute embolism on chronic ground if they had chronic pulmonary embolism characteristics on CT.
In the axial view, a cross-section was reached where all heart chambers were visible. Here, the widest cross-section of the right ventricle was found, and the widest diameter was manually measured perpendicular to the interventricular septum. A similar procedure was performed for the left ventricle to complete the measurement (it is not necessary that both ventricles be in the same cross-section). 23
Statistical Analyses
Data were described as mean ± SD for numeric factors and as percentages and frequencies for nominal factors. Comparative analyzes for nominal data were made by chi-square or Fisher's exact test. Depending on the distribution characteristics for numerical factors, differences between groups were compared using t-test or Mann-Whitney test. The factors associated with in-hospital mortality were assessed with a multivariable logistic regression model. The variables(RV/LV diameter ratio,pulmonary artery diameter,oxygen saturation,age and gender) were determined by clinical judgment and included in the model. Multivariate linear regression analysis was performed with pulmonary artery diameter, as the dependent factor. Age, male sex, oxygen saturation, left atrium area and mosaic pattern are predictor factors. Predictor factors were recorded into the multivariate model using a stepwise procedure.
P < .05 values were considered statistically important. Statistical analyzes with SPSS Statistics software were done(version 17.0).
Results
The specific ICD codes were used to identify patients with pulmonary embolism. We included 254 patients with PE in the 6 years studied (Figure 1). The elderly group had a mean age of 80.6 years, and the younger patients had a mean age of 41.4 years.

Flow Chart of the Study.
Echocardiography information was obtained in 157 of 254 patients (61.8%). Elderly patients have lower left ventricular ejection fraction and higher systolic pulmonary artery pressure than younger patients. The clinical and radiological features of the elderly and younger patients are shown in Table 1.
Characteristics of Elderly and Younger Patients.

Values are presented as mean ± standard deviation or number (%).
*Anticoagulant therapy (which is initiated in D-dimer-positive patients suspected of having pulmonary embolism based on symptoms).
Enlarged complete artery occlusion (67.5% vs 32.1%, P = .0001), polo mint sign (47.2% vs 25.2%, P = .0001) and partial filling defect with acute angle(57.7% vs 30.5%, P = .0001) were more frequent in younger patients compared to elderly group.
Shrunken complete artery occlusion (62.6% vs 32.5%, P = .0001),thickened small arteries (64.1% vs 33.3%, P = .0001),bilateral pleural effusions (16.8% vs 4.9%, P = .002),variation in the size of segmental vessels (30.5 vs 8.9, P = .0001) and mosaic perfusion pattern (55.0% vs 28.5%, P = .0001) occurred more often in the elderly group compared to younger patients. The prevalence of right ventricular/left ventricular ratio ≥1 in elderly patients is higher than in younger patients (55.0% vs 19.5%, P = .0001, respectively). In-hospital mortality rates are higher in elderly pulmonary embolism patients than in younger patients (10.7% vs 2.4%, P = .009, respectively). Chronic pulmonary embolism is more common in elderly patients than in younger patients (n:84/131, 64.1% vs n:37/123, 30.1%, P = .0001,respectively). 5.9% of all patients (n:15/254) and 15.6% of patients (n:15/96) with RV/LV ≥ 1 received thrombolytics. Receiving thrombolytics can be considered as a surrogate for high risk PE.
Dyspnea was the most common symptom seen in older and younger group in terms of the clinical presentation of PE. The patients’ dyspnea durations are shown in Table 2. Acute dyspnea is more common in young patients (67.5% vs33.6,P = .001, respectively) while chronic dyspnea is more common in elderly patients (48.1% vs14.6, P = .001, respectively).
The Duration of the Patients’ Dyspnea.

Syncope was significantly more frequent in the elderly patients than younger group,see Table 1. Comorbidity (oncologic disease,cerebral disease,chronic kidney disease, any lung diseases) was significantly more frequent in the elderly patients than younger group.
In terms of the laboratory parameters, there were significant differences in the mean creatinine and proBNP values, which were higher in the elderly group.
Oxygen saturation was significantly lower and pulmonary artery diameter was larger in elderly patients compared to the younger group.
Presence of right ventricular dysfunction (RV/LV diameter ratio ≥ 1)[OR:16.1(95% CI:1.9 to 135.3), P = .01] and lower oxygen saturation determined while breathing room air on admission [OR:0.88 (95% CI:0.82 to 0.94), P = .0001] seem to be associated with an increased risk of in-hospital mortality in pulmonary embolism patients in logistic procedures (Table 3).
The Predictors of in-Hospital Death in Pulmonary Embolism Patients in Logistic Procedures.

Note: Multivariate logistic model showing adjusted odds ratios of statistically significant variables with confidence intervals (CI). Non-significant variables considered for inclusion included age,gender.
The predictors of in-hospital death in pulmonary embolism patients in logistic procedures are shown in Table 4. Accordingly, in-hospital death in pulmonary embolism patients is associated with age and increased pulmonary artery diameter.
The Predictors of in-Hospital Death in Pulmonary Embolism Patients in Logistic Procedures.

Note: Multivariate logistic model showing adjusted odds ratios of statistically significant variables with confidence intervals (CI). Non-significant variables considered for inclusion included gender.
Predictors of pulmonary artery diameter in regression analysis are shown in Table 5. According to linear regression analysis, the main pulmonary artery diameter is determined by age, mosaic pattern and left atrium area.
Predictors of Pulmonary Artery Diameter in Regression Analysis.

Table 6 shows the clinical characteristics of deceased patients and their cause of death.
Clinical Characteristics of Deceased Patients.

Signs of serious infection are seen in 9 of the 17 cases (52.9%) that died. A high RV/LV ratio was seen in 16 of the 17(94.1%) deceased cases.
CT features of patients are shown in the Figures 2–6.
EY 91 Year old Female. Total Occlusions in the Left Upper Lobe Anterior Segment Artery. PA:32 mm.

MK 89 Year old Female. Total Occlusion of the Right Upper Lobe Anterior Segment Artery. PA:36 mm.
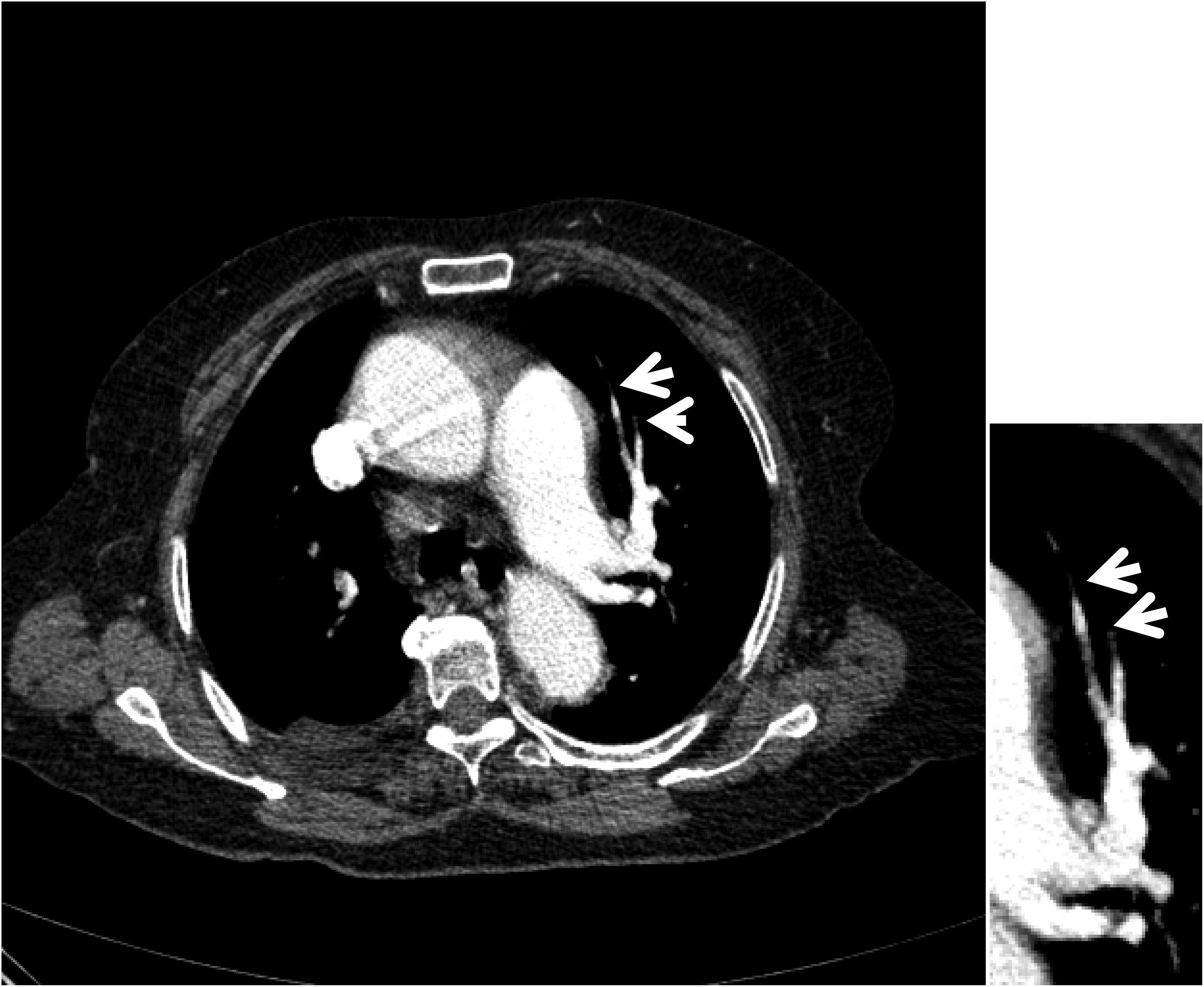
SÜ 91 Year old Female. Chronic Mural Thrombus in the Right Main Pulmonary Artery.

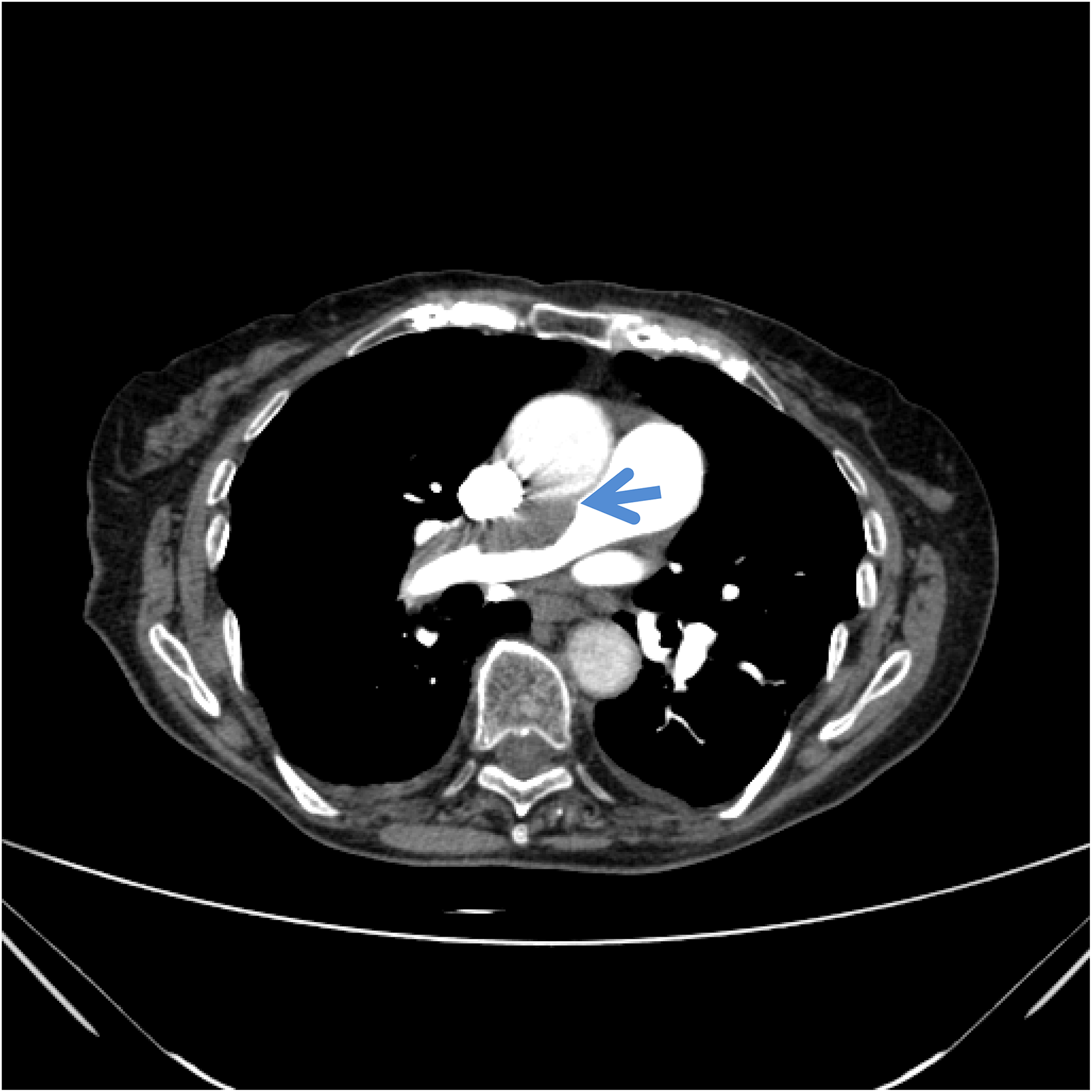
GY 91 Year old Female. Acute Thrombus in the Main Pulmonary Artery and Bilateral Pleural Effusion.

F.N.A. 21 Year old Female. PA: 30 mm. Web View in the Lingular Artery.
Discussion
This study suggests that elderly patients with pulmonary embolism typically exhibit chronic CT features, whereas younger patients tend to display more pronounced acute pulmonary embolism features.With age,increased comorbidity,prolonged hospital stay, decreased mobility, the development of chronic inflammatory diseases, decreased venous tone, increased need for surgical procedures, decreased fibrinolytic activity and weakened immunity may play a role in the more frequent occurrence of chronic pulmonary embolism characteristics in the elderly.24–26 Besides,individuals in a lifelong or intermittently procoagulant state may consistently develop small pulmonary embolisms that go unnoticed clinically.27–29 Over time, these small embolisms can result in chronic pulmonary embolism.27,28 While it is well known that chronic thromboembolic pulmonary hypertension (CTEPH) occurs in approximately 3.8% of acute pulmonary embolism cases, 30 the extent to which CTEPH develops in cases of silent recurrent embolism is not yet clear. It is possible that silent embolisms begin at a young age and continue intermittently for many years, gradually enlarging the diameter of the pulmonary artery. Silent recurrent pulmonary embolism events are difficult to detect. However, early diagnosis of chronic silent recurrent pulmonary embolism in young individuals may be critical to prevent potential complications by administering anticoagulant therapy during high-risk periods, such as infection or surgery. Further, chronic pulmonary embolism and a high RV/LV ratio are more common in elderly patients, which may partially explain the increased risk of in-hospital mortality in this population. Low oxygen saturation and right ventricular enlargement, which can result from acute or chronic pulmonary embolism, appear to play a significant role in in-hospital mortality. Furthermore, enlargement of the main pulmonary artery diameter, a characteristic of chronic pulmonary embolism, is associated with in-hospital mortality. In addition to these characteristics of acute and chronic pulmonary embolism, infection or sepsis is also a significant factor in in-hospital mortality. Signs of serious infection are seen in 9 of the 17 cases (52.9%) that died. According to these data, the clinical presentation and outcomes of pulmonary embolism demonstrate significant differences between elderly and younger patients. A study investigating whether radiological findings on CT pulmonary angiography (CTPA) during acute PE could indicate the presence of preexisting CTEPH found that 89% of patients had at least one finding suggestive of chronicity, regardless of whether they had a prior history of symptomatic VTE. 31 These authors noted that patients presenting with acute or recurrent PE may (unknowingly) already have chronic thromboembolic disease or CTEPH, and a number of imaging parameters have been identified that suggest chronic pulmonary vascular disease, but none of these parameters are currently requested or reported on CTPAs performed to confirm acute PE in clinical practice. 31 In a study conducted on patients aged 70 years on average who underwent CT with suspected pulmonary embolism, RV/LV ≥1 was found in 64.1% of all patients, 63% of patients without PE and 70% of patients with PE. 23 The high rate of right ventricular dysfunction seen in this study may be due to unevaluated chronic pulmonary embolism and left ventricular dysfunction. Evaluation of radiological findings indicating chronicity in studies may change the results.
Another important result of the current study is that the main pulmonary artery diameter is associated with age, mosaic pattern, and left atrial area. Elderly patients with a larger pulmonary artery diameter are more likely to have higher pulmonary artery pressure, which in turn increases the likelihood of chronic thromboembolic pulmonary hypertension in these patients. CT-determined main pulmonary artery diameter ≥29 mm had a positive predictive value of 0.97 for predicting pulmonary hypertension. 32 Since the diagnosis and treatment of CTEPH is difficult in developing countries, patients continue their lives with alternative diagnosis and wrong treatment. 33 The wider left atrial area in the elderly group suggests the presence of left ventricular dysfunction. Left atrial dilation is typically caused by chronic elevation of left atrial pressure, which is commonly associated with left ventricular systolic and/or diastolic dysfunction. 34 Chronic vascular disease indicated by the mosaic perfusion pattern and left ventricular dysfunction are observed to contribute to the widening of the pulmonary artery diameter along with age.
Limitations
It should be noted that this study has some limitations. First, the study is the retrospective nature. Second, the sample size is relatively small and external verification is required in a larger population. Thirdly, in the study, patients did not undergo ventilation/perfusion scintigraphy, and right heart catheterization. Fourth,right ventricular function was not assessed on echocardiography.
Conclusions
In elderly patients, the CT features of pulmonary embolism generally possess a chronic nature, while in young patients, they typically exhibit acute characteristics. When evaluating pulmonary embolism in elderly patients, the physician should take into account the chronic features of CT and not ignore them. Age and characteristics of acute and chronic pulmonary embolism, such as a high RV/LV ratio, low oxygen saturation on admission, and an increased pulmonary artery diameter, may determine outcomes.
Footnotes
Abbreviations
Ethical Approval
This study was approved by Ethical Review Committee of the Kırıkkale University prior the commencement of study (Decision number: 2019.11.12- Date: 18.12.2019). Informed Consent was not necessary for retrospective data used in this study.
Author Contributions
ME and A E planned to work.
Ş İ and A B Ç, H A made the analysis.
M.E., A.E. and Ş İ prepared the draft.
All authors participated in the interpretation of the results and the writing of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors of this article do not declare any relationship with any company whose products or services may be related to the subject of the article.
Data Availability
All data supporting the findings of this study are included in the article and its Supplementary data files(SPSS 17.0).
Methodology
Retrospective, Observational, Performed at one institution.
Guarantor
The scientific guarantor of this publication is Dr Mehmet Ekici.