
Abstract
Introduction
Hemophilia A is a rare inherited bleeding disorder. Less than 1% of FVIII level in plasma is classified as severe, 1%–5% as moderate, and above 5% as mild disease. The aim of this study is to share clinical and surgical experiences in Hemophilia A with extended half-life (EHL) recombinant FVIII preparations.
Material and Methods
A retrospective observational study between 2024 and 2025, inpatient or outpatient follow-up was carried out in the Pediatric Hematology clinic of our university hospital. A total of 18 patients diagnosed with severe FVIII deficiency were included in this study.
Results
The average age of the patients was 8.4 years (min. 20 months—max. 17 years). All patients were male and inhibitor negative severe FVIII deficiecy patients. Patients were numbered as P1-18 respectively. P1, P4, and P8 are 20 months, 3 years, and 4 years old respectively. They were evaluated as previously untreated patients (PUP) with a new diagnosis of severe FVIII deficiency and the other patients were previously treated patients (PTPs). P10 had 2 infected decayed molars and 1 incisor extracted in the same dental session. P13 underwent circumcision operation. P18 had refixation surgery due to a left arm radius and ulna bone fracture, and a cast was applied. All three surgical operations were performed under treatment of recombinant FVIII Efmoroctocog alfa (Ealfa/Elocta®) successfully.
Conclusion
Efmoroctocog alfa seems to be effective in EHL FVIII replacement therapy and surgical management of hemophilia A. Compared with standard half-life (SHL) FVIII products, EHL FVIII products such as Ealfa have the potential to optimize prophylactic outcomes by decreasing the burden of treatment or increasing the level of bleed protection.
Introduction
Hemophilia A (HA) is a rare bleeding disorder primarily linked to the X chromosome, resulting from mutations in the FVIII gene. This mutation leads to either a malfunction or a reduced production of clotting factor FVIII, which in turn causes insufficient blood coagulation. 1 The severity of HA correlates directly with the levels of FVIII in the blood; lower levels indicate a heightened bleeding risk, consequently increasing morbidity and mortality rates. In cases of severe HA, FVIII plasma activity drops below 1% of normal levels, leading to spontaneous bleeding in joints and other tissues, which are significant health complications associated with the disorder. Approximately 90% of HA cases occur in males, with a prevalence rate of 17.1 per 100,000 males, of which 6.0 per 100,000 cases are classified as severe. 2
The standard treatment for patients with HA involves replacing the deficient clotting factor VIII through intravenous administration of FVIII products. Treatment for acute bleeding can be both on-demand and prophylactic to either treat or prevent burden of bleeding episodes. 3 In recent years, prophylactic treatment using standard half-life (SHL) FVIII products has necessitated multiple weekly intravenous infusions, posing challenges for patient adherence and presenting cost inefficiencies for healthcare systems. FVIII products can be categorized into two groups: SHL concentrates, which include traditional plasma-derived or recombinant FVIII, and extended half-life (EHL) concentrates, known for advantages of their long-acting properties. 4
Efmoroctocog alpha (Ealfa) (Elocta®/Eloctate®) is a recombinant factor VIII Fc fusion protein classified as an EHL product designed for treating hemophilia A. Despite the global launch of this EHL FVIII product nearly ten years ago, there remains a need for published data regarding its clinical, treatment, and surgical application. The extension of FVIII half-life with Ealfa varies among individuals but is reported to be between one to three times that of standard FVIII concentrates. 5 The effectiveness and safety of Ealfa bolus injections have been documented in a study involving 59 patients, including 10 who were under 12 years of age at the time of surgery. Similar to standard FVIII concentrates, continuous infusion of Ealfa can yield more stable factor VIII activity levels; however, safety and efficacy data for this administration method are still lacking. 6
Currently, there is a gap in pediatric population to suggest comprehensive overview of the literature addressing the efficacy of prophylactic therapy with EHLs in HA patients globally. 7 This study was designed to fill this gap in the literature and presents the features of surgery, bleeding burden management, and treatment with EHLs in pediatric patients with severe HA.
Material and Methods
Patient Selection and Registration
A retrospective observational study was carried out between 2024 and 2025, in 0–17 years old pediatric patients who are under follow-up at our inpatient or outpatient Pediatric Hematology clinic of our university hospital which is already a hemophilia treatment centre (HTC). Demographic information, the frequency of follow-ups, clinical symptoms, the number and sites of bleeding episodes, inhibitor levels (if applicable), complications, previous surgeries, and treatment and prophylaxis strategies of 18 patients diagnosed with severe HA who were monitored at our pediatric hematology clinic; were documented and retrospectively analyzed. Based on the World Hemophilia Organization (WHO) definitions, which consider the relationship between bleeding severity and clotting factor levels, severe FVIII deficiency is defined as <1 IU/dL (<0.01 IU/mL) or less than 1% of normal. All patients included in this study met this criterion. All pediatric Hemophilia A patients with Factor VIII levels above 1% were excluded from this study. The patients included in this study are identified in Table 1 as P1 to P18.
Demographic and Clinical Characteristics of the Patients in Study Group.

Statistical Analysis
The primary and secondary endpoints supporting the main objective were descriptively presented, showing mean (standard deviation [SD]) and median (interquartile range [IQR]) values for all study group data. Annualized rates for descriptive analysis were calculated based on the number of bleeding events, injections, or total factor dispensed or consumed over the specific treatment period, divided by the duration in days and multiplied by 365. This manuscript primarily utilizes descriptive statistics, with no further statistical analyses conducted.
Results
The average age of the patients was 8.4 years (ranging from 20 months to 17 years), and all participants were male and severe FVIII deficiency pediatric patients. Patients were sequentially numbered P1 through P18. P1, P4, and P8 were 20 months, 3 years, and 4 years old, respectively. P1 exhibited a subcutaneous hematoma (4 × 5 cm) following a frontal head impact, P4 had bloody stools attributed to gastroenteritis, and P8 presented with a 2 × 3 cm hematoma in the frontal region. These three patients did not experience any bleeding episodes before diagnosis, other than non-life-threatening nosebleeds, bruises on the body, and local prolonged bleeding at the vaccination site and these Previously untreated patients with newly diagnosed severe FVIII deficiency (PUP) received Ealfa at a dosage of 25 IU/kg twice daily after acute bleeding treatment. After initial treatments, these patients transitioned to a regimen of 25 IU/kg twice weekly for primary prophylaxis. FVIII inhibitor tests for these three patients returned negative results after the eighth, 20th, and 32nd doses. The remaining patients were previously treated patients (PTPs). Despite P10's severe FVIII deficiency, no bleeding episodes were recorded during follow-up while receiving 25 IU/kg secondary prophylaxis weekly. Table 1 presents the demographic and clinical characteristics of all patients.
P10, aged 7 and diagnosed with severe FVIII deficiency, was on secondary prophylaxis with Ealfa at 25 IU/kg weekly. Following a dentist's request, a single dose of Ealfa (50 IU/kg) was administered one hour prior to the extraction of two infected molars and one incisor. The patient did not experience any bleeding necessitating additional doses during the 48-h postoperative follow-up, indicating successful management of the surgical procedure with a single dose.
In another procedure, P13 underwent circumcision. Prior to surgery, the patient's inhibitor level was recorded as <0.2 BU. Ealfa was administered intravenously at 50 IU/kg the day before the operation as a prophylactic measure and repeated at the same dose two hours prior to surgery, with normal coagulation parameters on the day of the procedure. Tranexamic acid was also initiated intravenously 4 times a day at a dosage of 10 mg/kg. The second dose of Ealfa was given 36 h post-surgery, and the patient showed no signs of bleeding, leading to discharge after 48 h. During follow-up visits, no bleeding was noted on days 5 and 10.
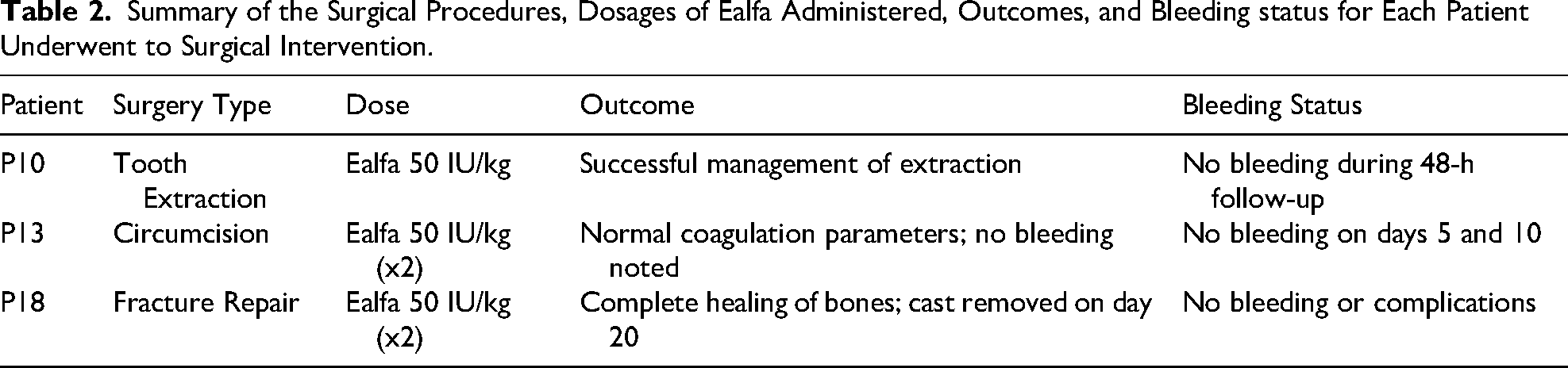
P18 presented with swelling and pain in the left arm at the emergency department. The patient had severe HA (FVII level 0.8%) and was being monitored as inhibitor negative. He was receiving prophylaxis with SHL rVIII at 25 units/kg twice weekly. Diagnosed with fractures of the left arm's radius and ulna, EHL rVIII-Ealfa was urgently initiated at a dose of 50 units/kg twice daily due to the risk of significant bleeding. An orthopedic surgeon performed a refixation surgery after 12 h, followed by cast application. The patient continued receiving Ealfa at 50 units/kg twice daily for the first three days post-surgery and then switched to 25 units/kg daily from the fourth to the seventh day. The patient experienced no bleeding or complications and was discharged with a prophylactic regimen of 25 units/kg Ealfa twice weekly. The cast was removed on day 20 during an outpatient visit, showing complete healing of the bones. Table 2 displays Summary of the surgical procedures, dosages of Ealfa administered, outcomes, and bleeding status for each patient underwent to surgical intervention.
Summary of the Surgical Procedures, Dosages of Ealfa Administered, Outcomes, and Bleeding status for Each Patient Underwent to Surgical Intervention.
Discussion
Current guidelines advocate for primary prophylaxis in patients with severe hemophilia. Prophylaxis should be tailored to individual patients based on their age, weight, FVIII recovery times, bleeding frequency, and activity levels. 8 Nevertheless, patients may still face chronic joint damage from daily activities and bleeding events in joints and muscles. Thus, it is advisable to adjust prophylaxis treatments based on a patient's lifestyle. 9
Recombinant DNA technology has facilitated the development of first-generation recombinant FVIII (rFVIII) concentrates utilizing human albumin-stabilized ovary cells from Chinese hamsters (OCh) or kidney cells from baby hamsters (KBh). 10 The subsequent second-generation KBh-derived rFVIII was formulated using sucrose instead of albumin, while the OCh-derived product has evolved into a third-generation rFVIII that does not contain additional human or animal plasma proteins. Additionally, a B-domain deleted rFVIII was developed without compromising its hemostatic efficacy. 11 The overall clinical considerations of Ealfa in HA are summarized in Table 3.
The Overall Clinical Considerations of Efmoroctocog Alfa in Haemophilia A Patients.

This study presents clinical and surgical experiences with Ealfa, a third-generation rFVIII. Further research on the clinical and surgical applications of third-generation rFVIIIs remains necessary. While there is a overview on initiating prophylaxis early in children, debates continue regarding the intensity of prophylactic regimens and methods of initiation. Although there are risks such as early inhibitor development, the inhibitors were found to be negative in the three newly diagnosed PUP patients at the eighth, 20th, and 32nd doses in this study, which provides valuable insights in clinical practice to mitigate concerns regarding inhibitor development.
Research by James E. Frampton demonstrated the effectiveness of Ealfa in preventing and managing bleeding in both PTPs and PUPs with severe hemophilia A, as evidenced in phase III studies, including its application in perioperative settings (in PTPs). 12 Our study included both PTPs and PUPs, and as illustrated in Table 1, no active bleeding occurred among any patients receiving Ealfa prophylaxis or treatment during the 6-month follow-up.
The efficacy of Ealfa in preventing and treating bleeding episodes in PTPs with severe HA has been validated in two open-label, non-comparative, multinational phase III trials (A-LONG and Kids A-LONG)13,14 and confirmed in a long-term extension study (ASPIRE). 15 The pharmacokinetic parameters of Ealfa in this study are outlined in Table 4.
Pharmacokinetic Parameters of Efmoroctocog Alfa of Phase III Studies.

Efmoroctocog alfa (Ealfa/Elocta®), an extended half-life (EHL) recombinant FVIII product, has the potential to offer cost-effectiveness compared to standard half-life (SHL) FVIII preparations, despite its higher upfront cost. The prolonged half-life of Efmoroctocog alfa allows for reduced dosing frequency, which can lower the overall treatment burden and improve adherence to prophylactic regimens. This, in turn, may lead to fewer bleeding episodes and reduced healthcare utilization, such as emergency visits, hospitalizations, or additional treatments for bleed-related complications. Additionally, the enhanced bleed protection provided by EHL products can improve patients’ quality of life and productivity, further contributing to indirect cost savings. While initial acquisition costs may be higher, the potential for long-term savings through optimized prophylaxis and better clinical outcomes makes Efmoroctocog alfa a cost-effective option for managing Hemophilia A, particularly in patients requiring intensive prophylactic therapy.14,15
In a study by Kremer Hovigna et al, a three-year-old boy diagnosed with severe hemophilia A at six days old began prophylaxis at twelve months after experiencing his first joint bleed. For the planned replacement of a central venous catheter due to leakage from a prior port-a-cath, the patient received a bolus of 60 IU/kg/d Ealfa one hour before surgery, followed by a continuous infusion of 4 IU/kg/hour (0.4 mL/h). The lower starting rate of 4 IU/kg/h was chosen due to anticipated higher FVIII levels with Ealfa compared to standard half-life recombinant FVIII concentrates. During the surgery period, a total of 472 IU/kg of Ealfa was utilized over seven days (averaging 67 IU/kg/d), with the surgery and recovery being free of complications. 16
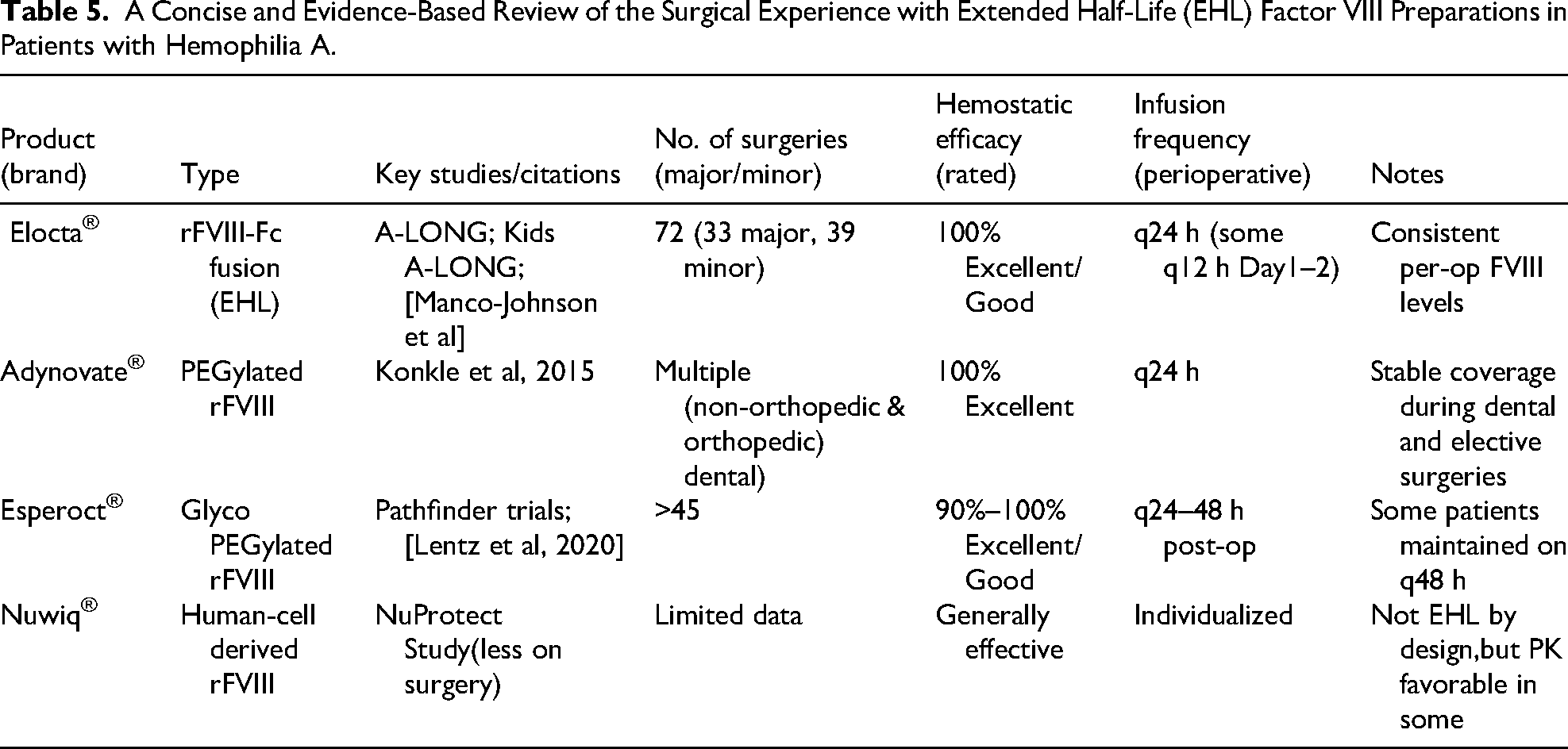
Manco-Johnson et al reported outcomes from 33 major and 39 minor surgeries performed on HA patients using Eloctate® (rFVIII-Fc). A median of 2.5 doses of 50 IU/kg were administered within the first 24 h post-surgery, achieving excellent or good hemostatic efficacy in 100% of the procedures. 17 A concise, evidence-based review of surgical experiences using EHL factor VIII preparations in Hemophilia A patients is provided in Table 5.
A Concise and Evidence-Based Review of the Surgical Experience with Extended Half-Life (EHL) Factor VIII Preparations in Patients with Hemophilia A.
In our research, the first surgical intervention involved P10 with severe FVIII deficiency, who received a single dose of Ealfa (50 IU/kg) one hour before the extraction of two decayed and infected molars along with one incisor, followed by an additional dose at the 48–72 h follow-up. This indicates the successful management of surgical procedures in severe FVIII deficiency cases using rFVIII Ealfa.
The 24-month, prospective, non-interventional, European multicenter A-SURE study evaluated the real-world effectiveness of prophylaxis using Ealfa (FVIIIFc) compared to SHL-FVIII products in hemophilia A patients. The A-SURE study confirmed that rFVIIIFc offers distinct advantages over SHL FVIII products, including enhanced bleed protection, reduced injection frequency, and lower factor consumption, thus addressing key unmet needs associated with SHL FVIII prophylaxis. 18 No new inhibitors developed in patients treated with rFVIIIFc, even among those with a history of inhibitors. Despite the severe deficiency of all HA patients in our study, compared to mild/moderate or severe cases in A-SURE, no inhibitor development was observed in either PUP or PTP patients at the one-year follow-up. Furthermore, the efficacy rates of standard treatments, prophylaxis, and surgeries using Ealfa in our study align closely with those found in the A-SURE study, as detailed in Table 1.
Another surgical case involved the circumcision of patient P13. Prior to the surgery, the patient's inhibitor level was noted as <0.2 BU. Ealfa was given at 65 IU/kg the day before the procedure and repeated at the same dose two hours prior, considering the patient's normal coagulation parameters on the day of surgery. Tranexamic acid was also initiated intravenously at a dose of 4 × 10 mg/kg. A second dose of Ealfa was administered 36 h post-operation, and the patient was discharged after 48 h with no bleeding episodes. Follow-up visits on days 5 and 10 showed no bleeding incidents. Efmoroctocog alfa is recognized as an effective EHL FVIII replacement therapy, and our surgical findings demonstrate that Ealfa is both effective and well-tolerated in HA surgeries.
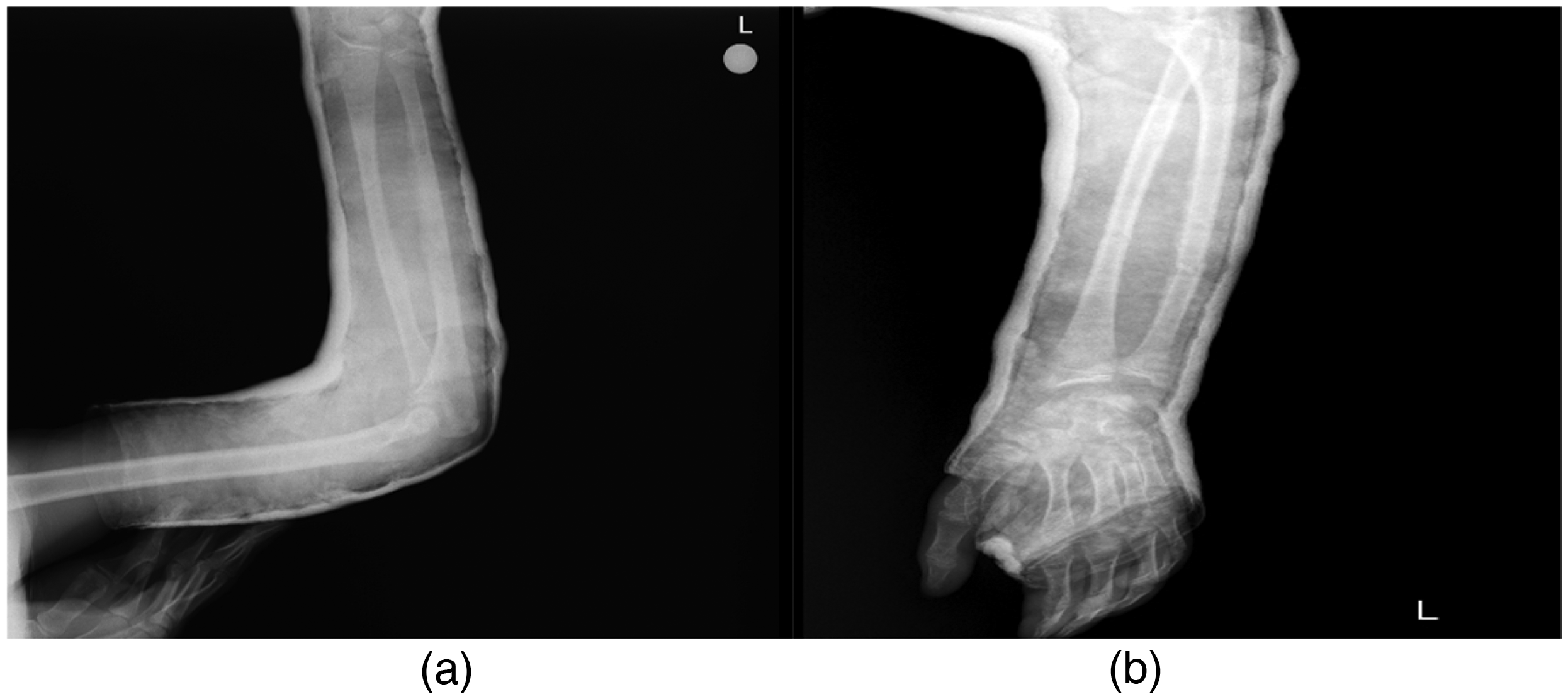
P18, who experienced left arm swelling and pain, was diagnosed with severe HA (FVII level 0.8%) and was under observation as inhibitor negative. Receiving SHL rVIII prophylaxis at 25 units/kg twice weekly, he was found to have fractures in the radius and ulna of the left arm. Due to the risk of significant bleeding, urgent treatment with EHL rVIII Ealfa was initiated at 50 units/kg twice daily. The orthopedic surgeon performed a refixation operation after 12 h and applied a cast. Post-surgery, the patient continued receiving Ealfa at 50 units/kg twice daily for three days, followed by 25 units/kg daily from days 4 to 7. The patient experienced no bleeding or complications and was discharged with a prophylactic regimen of 25 units/kg Ealfa twice weekly. The cast was removed on day 20 during an outpatient visit, indicating complete healing of the ulna and radius. This significant surgical operation was effectively managed with Ealfa treatment and prophylaxis. Preoperative and postoperative views of the fractured bones and clinical healing under Ealfa treatment are depicted in Figure 1 and 2.

(a) Anterior-posterior(AP) View of Radius and Ulna Bone Fracture of Left Arm Before Refixation Surgery.(1.Day of Diagnosis). (b) Lateral(L) View of Radius and Ulna Bone Fracture of Left Arm Before Refixation Surgery.(1.Day of Diagnosis).
(a) AP View of Left Arm in 15. Day of Surgical Refixation Operation of Radius and Ulna Bone Fracture and a Cast was Applied. (b) L View of Left Armof 15. Day After Surgical Refixation Operation of Radius and Ulna Bone Fracture and a Cast was Applied.
Conclusion
The early implementation of prophylaxis enables patients with severe hemophilia to maintain a high quality of life without substantial physical or psychological limitations. The increasing adoption of secondary and tertiary prophylaxis minimizes joint morbidity and enhances quality of life even in later stages. Ongoing investigations are focused on strategies to reduce treatment costs while sustaining high-quality care, especially through personalized approaches. Consequently, third-generation rFVIII-EHL preparations are viewed as a vital option, offering extended half-life and efficacy for various treatments, prophylaxis, and surgical interventions. To achieve optimal outcomes in the management of HA, further controlled clinical studies, like the one presented here, are essential.
Limitions
The main limitation of this study is the relatively small sample size, consisting of only 18 patients, which may limit the generalizability of the findings to larger populations of individuals with Hemophilia A. Additionally, the study was conducted within a single institution, which could introduce bias and restrict the diversity of patient characteristics, such as genetic or environmental factors. The follow-up period, spanning from 2024 to 2025, may not be sufficient to assess long-term outcomes and potential complications associated with the use of Efmoroctocog alfa (Ealfa/Elocta®) in extended half-life (EHL) FVIII replacement therapy. Lastly, the heterogeneity of surgical procedures and the lack of detailed data on bleeding episodes outside of surgical contexts may limit the ability to draw comprehensive conclusions about the overall efficacy and safety of EHL FVIII products in all clinical scenarios.
Footnotes
Acknowledgements
The authors are thankful to all individuals who have contributed to this study.
Ethical Considerations
This study was approved by the Ethics Committee of Istanbul S.B.Ü. Kanuni Sultan Suleyman Traning and Research Hospital (approval number: 131, date: June 6, 2024)
Consent for Publication
Has been obtained from the patients’ parents. The patients’ parents gave informed written consent for their personal or clinical details along with any identifying images to be published in this study.
This manuscript has not been submitted or is not being considered by other publications.
Authors’ Contributions
Author Huseyin Avni Solgun declare that he have participated in the design, execution, and analysis of the paper, and that he has approved the final version
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Authors keeps the right for all data, samples or models in this manuscript and can be accessed via email to corrospending author.
Artificial Intelligence
Artificial Intelligence (AI) supported technologies (such as Large Language Models [LLMs], chatbots or image generators, ChatGPT) were not used in the study.