
Abstract
Background
Effective anticoagulation control is critical in patients with atrial fibrillation (AF) to prevent thromboembolic events. Warfarin remains widely used in resource-limited settings like Nepal, where maintaining therapeutic levels is often challenging. This study aimed to assess the proportion of anticoagulation control and identify associated factors in patients with AF receiving warfarin therapy.
Methods
A cross-sectional study was conducted among 235 AF patients receiving warfarin at a tertiary care hospital in Nepal. Anticoagulation control was evaluated using the Time in Therapeutic Range (TTR) calculated by the Rosendaal method. Sociodemographic, clinical, and medication-related data were collected and analyzed to identify factors associated with suboptimal TTR (<65%).
Results
The results showed that only 72 (30.6%) patients had a Time in Therapeutic Range of ≥ 65%. The mean percentage TTR is 40.14%. About 99 (42.1%) had International Normalized Ratio (INR) in the therapeutic range (2 - 3) on the hospital visit day. Statistical significance was found between good anticoagulation control and female gender. Similarly, good anticoagulation control was observed in the patients who never consumed Vitamin K-containing foods and among the patients with more than 5 years of therapy.
Conclusion
This study demonstrated that a significant proportion of individuals receiving warfarin therapy for atrial fibrillation in Nepal had suboptimal anticoagulation control. The relatively high prevalence of out-of-range INR values warrants further investigation to identify underlying causes and contributing factors. The study emphasizes the important role of clinical pharmacists in improving warfarin management and recommends regular, structured monitoring of PT-INR levels to enhance treatment effectiveness and reduce the risk of complications
Keywords
Introduction
Atrial fibrillation (AF), which is the most prevalent cardiac arrhythmia, affected 52.55 million individuals in 2021, marking a 137% increase since 1990. It has a significant impact on morbidity and mortality in clinical practice. 1 Men and women 40 years of age and older have a 1 in 4 lifetime risk of developing AF. Stroke risk and risk of death are five times and two times greater among individuals with AF compared to the general population, respectively. 2
Anticoagulation therapy is a cornerstone in the management of AF to reduce the risk of stroke and thromboembolism, with warfarin being frequently given due to its effectiveness and affordability.3,4 Warfarin has a narrow therapeutic window and requires frequent monitoring of patient's coagulation profile. Deviations of blood concentration of warfarin from its narrow therapeutic window can cause bleeding(side effect) due to over-anticoagulation or thrombosis (therapeutic failure) due to under-anticoagulation.5,6 The effectiveness of anticoagulation management is commonly assessed by using the Time in therapeutic range, which represents the proportion of a person's INR within the target range. 7 A higher TTR is associated with improved clinical outcomes including a decreased risk of thromboembolic and bleeding events, with an optimal threshold set at ≥65%.8,9 There is a 29% increase in the chance of death and a 10%–12% rise in the risk of an ischemic stroke and other thromboembolic events for every 10% increase in time spent outside of TTR.7,10,11 The most recent European Society of Cardiology (ESC) guidelines suggest a TTR of >70% for AF to ensure effective Vitamin K antagonist (VKA) treatment. 12 An estimated TTR of less than 55% indicates insufficient anticoagulation with VKAs. 13
It has been discovered that many variables such as demographics, comorbidities, concurrent drug use, dietary modifications, adherence to the therapy, and frequency of INR monitoring affect anticoagulation management in patients on warfarin therapy. 14 It is imperative to comprehend these aspects to improve patient outcomes and optimize anticoagulation management.
Despite the extensive use of warfarin in Nepal, there is limited research evaluating anticoagulation control, patient adherence, and associated factors in the Nepalese population. Since maintaining an optimal therapeutic range is essential in preventing complications, it is necessary to assess the effectiveness of warfarin therapy in real-world scenarios. Hence, the current study aims to bridge this gap by evaluating the anticoagulation control in AF patients at a tertiary care center in Nepal, providing evidence to enhance patient management and clinical decision-making.
Materials and Methods
Study Setting and Design
This study was a single-centered, descriptive, cross-sectional study carried out among patients with AF receiving warfarin therapy. The study was conducted at Manmohan Cardiothoracic Vascular and Transplant Center (MCVTC), under Tribhuvan University, Institute of Medicine (IoM) from August 5, 2023, to November 7, 2023.
Inclusion and Exclusion Criteria
This study included patients with AF who were 18 years old and above, had a minimum of two INR records taken at least 2 weeks apart, and had been on warfarin therapy for at least one month. Patients with incomplete clinical information and those without written consent were excluded from the study.
Sample Size and Sampling Technique
The following formula was used to determine the sample size of a descriptive cross-sectional study.
15

From the literature review of the previously published study, we got a prevalence of good TTR among the Asian population (p) of 16.7% and a precision error of 5%. 16
Estimated sample size, n = (z2 ×p × (1-p)) / d2 = (1.962 × 0.167(1-0.167)) / 0.052 = 213.7(approx. 214). Considering the non-response rate as 10%. The required sample size = 214 + 214 × 0.1 = 235. A purposive sampling technique of non-probability sampling was used.
Study Variables
The dependent variable was time in the therapeutic range value. Independent variables were age, gender, INR value, duration of warfarin therapy, presence of comorbid diseases, dose, concomitant medication, and foods interacting with warfarin.
Clinical Criteria
TTR value ≥65% is regarded as good anticoagulation control for patients with AF. 4 Generally, INR value from 2.0-3.0 is regarded as the therapeutic range, ≤1.99 is regarded as the sub-therapeutic range, and >3.0 is regarded as a supra-therapeutic range.10,17 Alcoholics are sub-classified into former alcoholics, non-alcoholics, and present alcoholics. Former alcoholics are individuals who did not consume alcohol in the last 12 months but who did previously consume alcohol. Non-alcoholics are individuals who have never consumed alcohol, and alcoholics are people who still consume alcohol. 18 Smokers are sub-classified into ex-smokers, non-smokers, and smokers. Ex-smokers are individuals who smoked previously but left at least a month ago. Non-smokers are individuals who never smoked, and present smokers are individuals who still smoke. 19 Drugs concomitantly administered with warfarin, such as aspirin, vitamin K supplements, antibacterials such as ciprofloxacin, levofloxacin, rifampin, azithromycin, sulfamethoxazole/trimethoprim, anti-fungal medications such as fluconazole, thyroid medications such as levothyroxine, anti-arrhythmias such as amiodarone, quinidine or propafenone, antacids/laxatives, carbamazepine, etc were also noted. 20 Foods interacting with warfarin were noted, such as vitamin-K containing foods (green leafy vegetables, spinach, broccoli, lettuce/salad, cabbage, soybean/soyabean oil, olive oil, avocado, canola oil, and cranberry/grapefruit juice), 21 coumarin-containing foods such as cinnamon, strawberry, cherries, green tea, celery, honey, carrot, and peppermint. 22 Patients were also assessed for the consumption of garlic for its potential interaction with warfarin and noted as consumed occasionally, every day, or never.23,24
Data Collection Tool
A data collection tool was prepared after reviewing similar articles that assessed anticoagulation management in patients with AF on warfarin therapy. Clinical and demographic data was collected from all patients fulfilling the inclusion criteria. Demographic information on cardiovascular factors and co-morbidities was included. The data collection tool included clinical characteristics such as INR values, bleeding records, and a revised clinical stratification tool for predicting stroke ie, CHA2DS2 – VASc score which allocates 1 point for heart failure, hypertension, diabetes mellitus, and vascular diseases; 2 points for age ≥75 years and prior stroke/transient or ischemic attack. 25 Bleeding risk was calculated using HAS-BLED score which allocates 1 point for each variable like Hypertension (uncontrolled systolic blood pressure >160 mm Hg), Abnormal renal and/or liver function, previous stroke, Bleeding history or predisposition (anemia), Labile INR, Age >65, medication usage predisposing to bleeding (clopidogrel, NSAIDs, aspirin), Alcohol use (≥8 drinks/week). 26 A questionnaire from a previous study 4 was adapted, revised, and validated to meet the objectives of our study. The tool was pre-tested, and necessary modifications were made before using it for actual data collection.
Data Collection
Socio-demographic data were collected from face-to-face interviews with participants. Clinical data, such as INR values, were obtained from the participant's medical report. Other necessary information was collected by interviewing the participants directly. The study participants were informed about the study and its objectives and screened for eligibility. Participants were asked for their written consent before they were enrolled. Throughout the data-collecting process, regular supervision and monitoring were conducted to ensure the accuracy and consistency of the data.
Assessment of Anticoagulation Control
Anticoagulation control was assessed with the help of TTR by Rosendaal's method. This method adds each patient's time within the therapeutic range and divides it by the total time of observation and assumes that between tests INR varies linearly. 27 The calculation of TTR was conducted with the assistance of a template developed and made freely available by INR Pro. 28 TTR value < 65% was regarded as poor anticoagulation control. 4 INR values from 2 weeks to 3-month intervals were used to calculate the Time in the Therapeutic range.
Data Management and Statistical Analysis
Collected data were entered and analyzed in the Statistical Package for Social Sciences (SPSS) software version 20. Descriptive data are presented as frequency and percentage and continuous data are expressed as Mean ± SD (Standard Deviation). Univariate and multivariate analyses were used to measure the association of dependent and independent variables, and a 95% confidence interval (CI) and P-values less than .05 were used to determine statistical significance.
Ethical Issues and Considerations Regarding Human Participants
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Committee (IRC), Institute of Medicine, Tribhuvan University, Maharajgunj, Kathmandu, Nepal (Approval number: 51(6-11) E2) and Manmohan Cardiothoracic Vascular and Transplant Center, Tribhuvan University, Maharajgunj, Kathmandu, Nepal (Approval number. 171080/81). Patient identification information, such as names or other personal information, was removed to maintain the confidentiality and anonymity of study participants.
Results
Socio-Demographic and Clinical Characteristics
The sample comprised 235 participants of which 165 (70.2%) were female. The mean age of the participants was 50.1 ± 14.2. The most common co-morbid conditions were hypertension (111, 47.2%) and rheumatic heart disease (106, 45.1%). The overall results on socio-demographic and clinical characteristics are presented in Table 1.
Socio-Demographic Data of the Patients with AF Receiving Warfarin at MCVTC.

Others* include Seizure disorders = 3 and Gout = 2
Dose and Duration of Therapy
Participants were found to be treated by warfarin for a median duration of 4 (IQR: 1-8) years, and the mean per day dose of warfarin was 4.32 ± 1.84.
INR Distribution
Most participants, 99 (42.1%), had INRs in the therapeutic range of 2–3 on the day of the hospital visit, as shown in Figure 1.
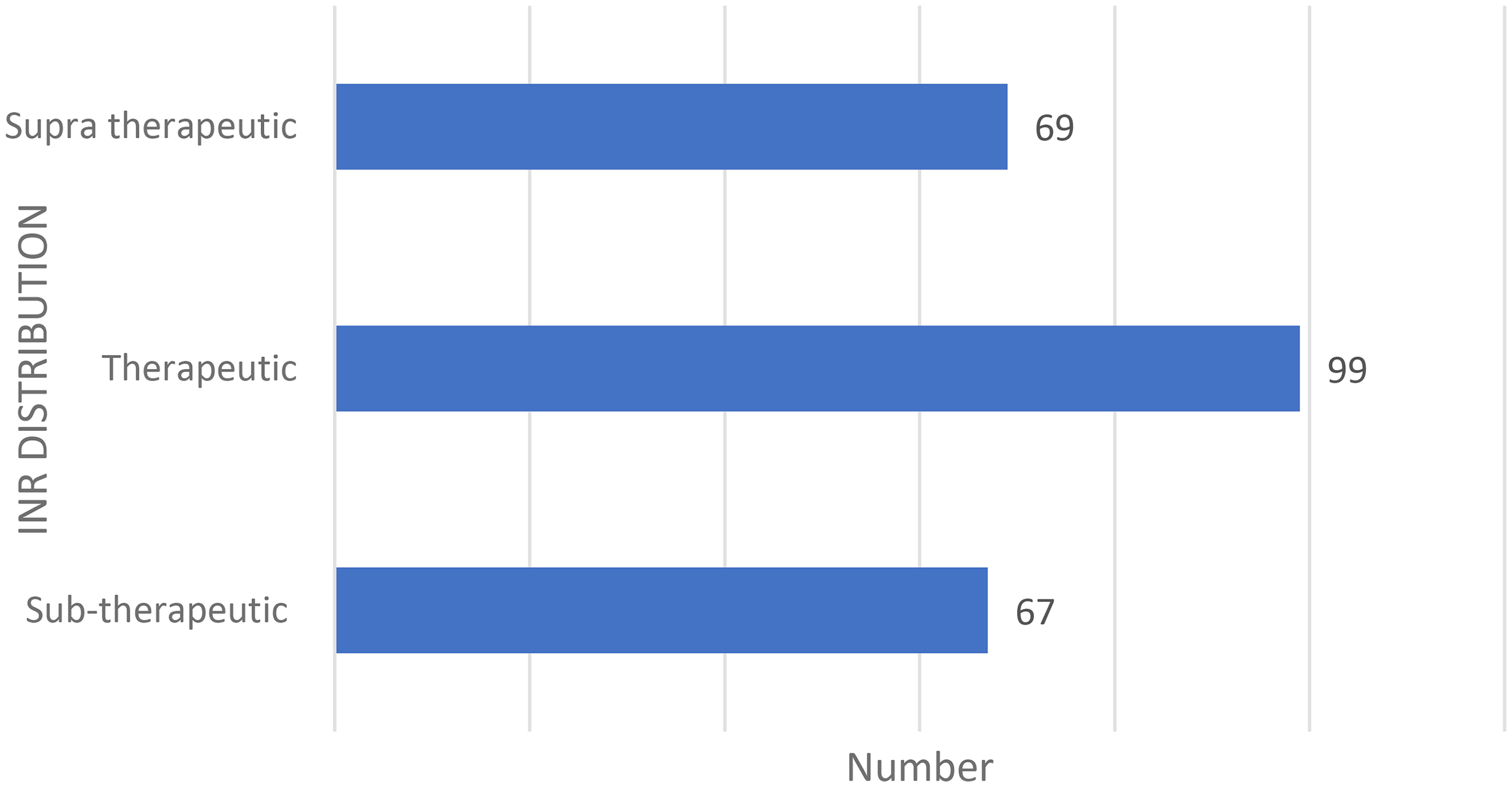
INR Distribution of Patients with AF Receiving Warfarin on the Day of Hospital Visit.
Time in Therapeutic Range (TTR)
According to Rosendaal's method, the median percentage TTR is 31.6 (IQR: 0-72)%, as shown in Figure 2.

Bar Diagram of Anticoagulation status of Patients with AF Receiving Warfarin at MCVTC.
Bleeding Events
The majority of the participants suffered bleeding events like gum bleeding (103, 43.8%), followed by nose bleeds (68, 28.9%). Purpura was noted in 23(9.8%) participants, while hematuria occurred in 16(6.8%) participants. Upper gastrointestinal (UGI) bleeding was less frequent, observed in 8(3.4%) participants, whereas both intracranial and retinal hemorrhages were reported in 2(0.9%) participants each. The least common was hemoperitoneum, recorded in just 1(0.4%) participant.
CHAD2DS2 – VASc and HAS-BLED Score
Among the three risk categories- high, intermediate, and low risk- females were found to be at a higher risk of stroke and bleeding compared to males. 77 females were at a high risk of stroke, and 71 females were at a high risk of having bleeding events, as shown in Figure 3.
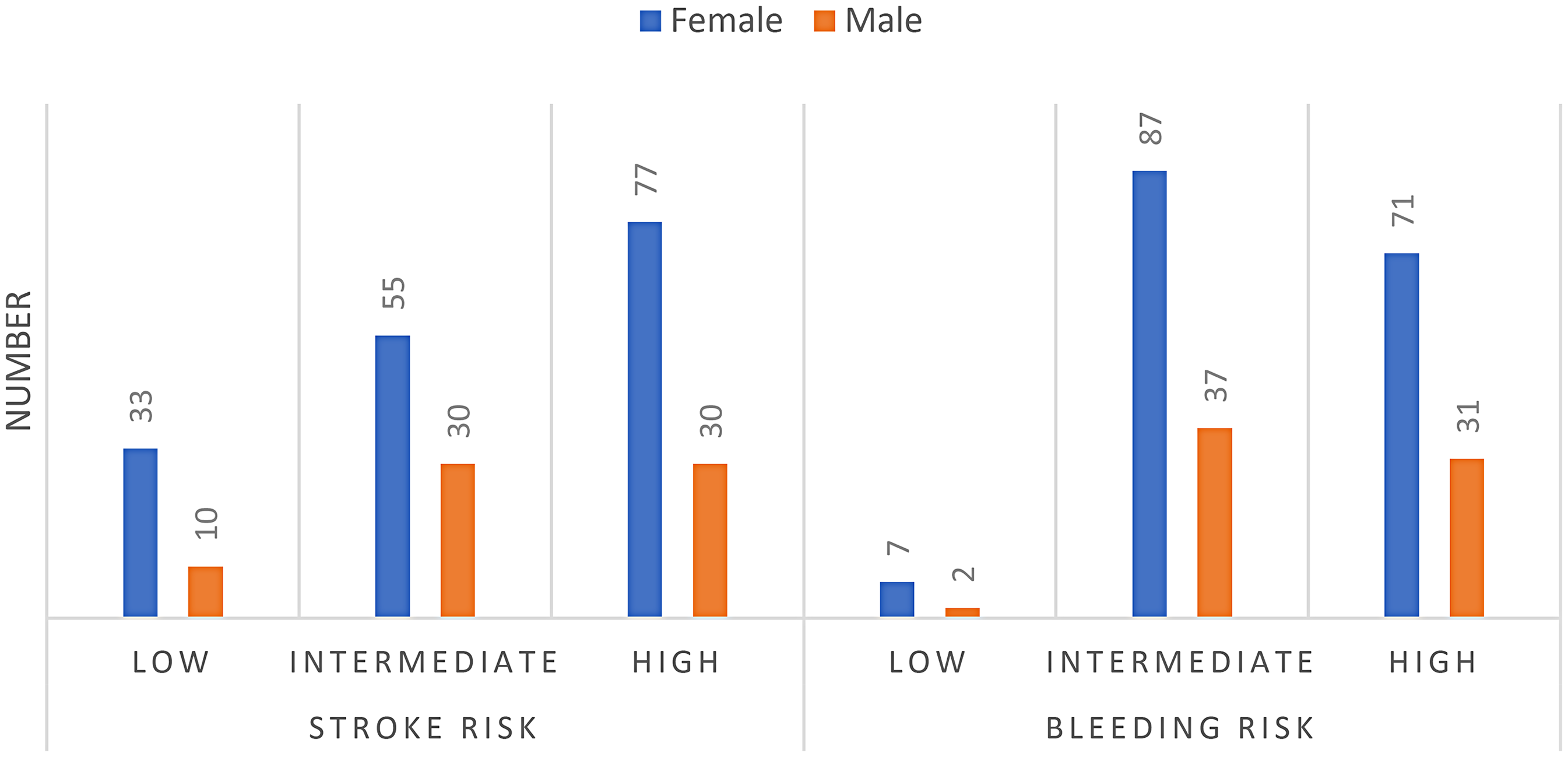
Interpretation of CHAD2S2 – VASc and HAS-BLED Score.
Foods Interacting with Warfarin
It was found that most participants, 162 (68.9%), occasionally consumed foods containing coumarin such as honey, celery, strawberries, cinnamon, carrots, etc Most of the participants, 137 (58.3%) occasionally consumed vitamin K-containing foods such as green leafy vegetables, spinach, broccoli, lettuce, cabbage, soybean, olive oil, cranberry juice, etc A majority of participants, 132 (56.2%) consumed garlic daily as summarized in Table 2.
Consumption of Foods Interacting with Warfarin.

Note: vitamin-K containing foods includes green leafy vegetables, spinach, broccoli, lettuce/salad, cabbage, soybean/soyabean oil, olive oil, avocado, canola oil, and cranberry/grapefruit juice and coumarin-containing foods such as cinnamon, strawberry, cherries, green tea, celery, honey, carrot, and peppermint.
Drugs Administered Concurrently with Warfarin
Altogether, 54.5% of participants were concurrently administered drugs interacting with warfarin. The majority of participants, 23.4%, were prescribed antibacterials, most of whom were receiving ceftriaxone, azithromycin, and levofloxacin. Similarly, 12.8% of participants were prescribed aspirin, followed by NSAIDs (9.4%), and amiodarone (8.5%), while carbamazepine had the lowest occurrence (0.4%). The interactions of these drugs with warfarin were verified using the online interaction database Epocrates®. 20 Epocrates is a frequently used database by physicians and has been shown by a recent study 29 to exhibit high integrity.
TTR Predictor Factors
The present study found that independent variables such as gender, non-consumption of vitamin K-containing foods, and duration of warfarin therapy were statistically significant with the outcome variable, ie, good anticoagulation control as summarized in Table 3.
Associated Factors of Good Anticoagulation Control in Patients with AF Receiving Warfarin at MCVTC.

The bivariate regression analysis of significant variables obtained from the chi-square test found that females had 1.935 (95% CI: 1.005-3.725) times higher odds of having good anticoagulation control than males. Individuals who never consumed vitamin-K-containing foods have 2.467 (95% CI: 1.072 - 5.674) times higher odds of having good anticoagulation control. Participants who had a duration of warfarin therapy of more than 5 years have 2.664 (95% CI: 0.508-2.689) higher odds of having good anticoagulation control than participants who had warfarin for less than 1 year, as shown in Table 4.
Bivariate Regression of the Significant Variables.

Discussion
Warfarin, being a medication with a narrow therapeutic index, necessitates ongoing monitoring of INR levels. The current study was conducted to evaluate anticoagulation control in patients with atrial fibrillation who were prescribed warfarin. It assessed anticoagulation levels and identified variables significantly influencing anticoagulation status in AF patients.
In our study, we observed a 70.2% female predominance. The most common co-morbidities were hypertension (47.2%) and rheumatic heart disease (45.1%). The predominance of females in our study can be attributed to Rheumatic Heart Disease, a leading cause of AF, particularly affecting the mitral valve in the form of mitral stenosis, which is more common in females. Studies conducted in Nepal as well as in India have also reported a higher prevalence of female patients with RHD as the most common co-morbidity.30,31
The present study observed a mean TTR of 40.14%. This result was comparable with findings from AF patients in Ethiopian (42.02%), 4 Chinese (38.2%), 32 Lithuanian (40%), 7 and Turkish (42.3%) 33 studies. A retrospective observational study conducted in India reported a median TTR of 13%. 34 In contrast to these findings, higher TTR values of 61.5% and 65% were reported by the FANTASIIA 9 and ORBIT-AF 35 registries respectively. The cohort study conducted in a European setting reported a mean TTR of 68.60%. 36 The differences may be related to study population characteristics, geographical barriers restricting the health care service, food habits across different countries, and anticoagulation management practices across various healthcare settings.
Our study reported that 30.6% of the participants achieved a TTR ≥ 65%. A study by Ng Diana et al evaluated the TTR at a tertiary cardiology referral center in Malaysia and found that 24.3% of people had good anticoagulation control with warfarin where TTR ≥ 60% was considered a good anticoagulation control in that study. 37 The low TTR is concerning because mortality increases with decreased TTR in warfarin-using individuals, with patients with <30% TTR having the highest mortality. 38 Another study by Liyew et al evaluated the TTR among hospital-admitted patients in Ethiopia and found that only 13% of patients attained good INR control (TTR ≥ 65%). 39 A study conducted in Namibia reported that only 10% of patients achieved a TTR of ≥ 65% 13 while a similar study conducted in Kenya indicated that 10.4% of patients reached a TTR of ≥ 70%. 40 Nonetheless, research conducted in the US and Europe has demonstrated that between 50 and 70% of patients had an appropriate anticoagulation level.41–45 The varying levels of anticoagulation control could be explained by the disparity in anticoagulation management services among the countries. According to Western reports, anticoagulation control has been enhanced by establishing anticoagulation clinics, computer-assisted warfarin dosing, self-testing, self-management among motivated patients, and coordinated follow-up clinics.46,47
In our study, only 42.1% of the INR tests were within the therapeutic range, and the remaining 28.5% and 29.4% of the INR values were below and above the expected therapeutic ranges, respectively. A similar study by Yimer et al reported that 35.15% of the INR values were within the therapeutic range and the remaining 49.55% and 15.23% of INR values were in the sub-therapeutic and supra-therapeutic ranges respectively. 4 Unlike this study, the multi-centered study conducted by Menzin et al in the US reported that the mean percentage of time patients spent in the therapeutic INR range was 62%. 48 The lower percentage of INR values within the therapeutic range in our study could be attributed to inadequate patient follow-up, the absence of specialized anticoagulation clinics, poor patient adherence, and irregular monitoring of the INR values. Effective anticoagulation control with warfarin can be achieved through patient education and close monitoring for dose adjustment. 49
This study reported a higher percentage of warfarin drug interactions (WDIs) 54.5%, most of whom (23.04%) were receiving antibiotics such as levofloxacin, azithromycin, and ceftriaxone. A similar study conducted in an Estonian setting by Gavronski et al reported a 57% prevalence of Warfarin drug interactions. 50 Another study conducted in the cardiology department of South Indian Teaching Hospital reported an 11.59% incidence of warfarin drug interactions. 51 The higher percentage of WDIs in our study may be due to the high prevalence of co-morbidities among the patients necessitating polypharmacy. Many medications, particularly antibiotics such as azithromycin and levofloxacin can potentiate warfarin's effect by inhibiting cytochrome P450 enzymes, leading to an increased risk of bleeding. 52
In our study, gender, non-consumption of vitamin K-containing foods, and longer duration of warfarin therapy were significantly associated with good anticoagulation control. Bivariate logistic regression showed that females had 1.935 times higher odds of having good anticoagulation control than compared to males. A study conducted in primary health care centers in Lithuania reported a similar finding that Males had a higher risk of poor anticoagulation control and suggested the presence of some important confounding variables among male participants. 7 In contrast to this finding, a study by Islam et al has revealed that over 50% of males and females had inadequate warfarin control (time in therapeutic range <65%), suggesting that both sexes face comparable difficulties in managing anticoagulation but adherence to therapy was found to be better in females than males (AOR:1.15, 95% CI 1.02 to 1.29). 53 Whereas, several studies have supported the female sex's association with lower TTR than the male sex.45,54,55 Good anticoagulation control among the female population in our study may be due to the adherence to therapy as demonstrated by a study conducted by Islam et al, 53 dietary habits, a larger proportion of the female population in the sample size due to the higher prevalence of RHD in females, and potential confounding variables that require further investigation.
Our study reported that patients with a duration of therapy >5 years had 2.664 (CI:1.174-6.045) times higher odds of having good anticoagulation control than patients with a duration of therapy less than 1 year. A similar result was reported in the study conducted in a Turkish setting by Turen et al The study revealed that duration of therapy > 10 years (OR: 2.2, 95% CI: 1.34-3.84, P-value: .002) is the independent predictor of good anticoagulation control. 56 This might be due to optimizing the warfarin dose through repeated hospital visits and INR monitoring compared to patients undergoing warfarin therapy for a short duration of time.
The bivariate regression analysis revealed that people on warfarin therapy, who never consume vitamin K-containing foods have 2.467 (CI: 1.072-5.674) times higher odds of having good anticoagulation control than patients who consume daily. According to a study conducted by Violi et al, patients on warfarin therapy showed a decrease in warfarin sensitivity for normal dietary intake of vitamin K ≥ 250 μg/day. This study highlighted the possible influence of dietary vitamin K on warfarin effectiveness by indicating an inverse relationship between the amount of anticoagulation and vitamin K intake. 57 However, another study conducted by Park et al found no significant association between the consumption of Vitamin K and anticoagulation control among patients taking warfarin. 58 The findings emphasize the necessity for more studies that take inter-individual variations in vitamin K intake into account.
Limitations
This study has several limitations that should be acknowledged. First, INR quality control measurements were not assessed, limiting our ability to evaluate inter- and intra-center variability in laboratory testing, which may have influenced the accuracy and consistency of INR values reported. Second, the study did not systematically document the frequency and clinical outcomes associated with sub-therapeutic or supra-therapeutic INR levels, such as bleeding or thrombotic events, which are crucial indicators of the safety and effectiveness of anticoagulation therapy. The current study assessed the concomitant administration of foods having potential interaction with warfarin though it didn’t assess the quantity consumed by patients. Due to limitations in data completeness and the retrospective nature of the study, INR levels at or immediately prior to the bleeding episodes were not consistently available for all cases.
Conclusion
The study revealed suboptimal anticoagulation control among a substantial proportion of atrial fibrillation patients receiving warfarin therapy in a Nepalese tertiary care hospital setting. While nearly half of the participants presented with an INR within the therapeutic range during their hospital visit, the overall TTR remained notably low. Anticoagulation control was significantly influenced by factors such as gender, dietary intake of vitamin K, and the duration of warfarin therapy. Notably, patients who consistently avoided vitamin K-rich foods and those with longer durations of therapy were significantly more likely to achieve optimal TTR levels. These findings highlight the complex, multifactorial nature of warfarin management.
Recommendation
The relatively high prevalence of out-of-range INR values observed in this study highlights the need for further investigation to identify underlying causes and contributing factors.
In light of these results, the study strongly recommends the potential role of clinical pharmacist in the warfarin management and implementation of rigorous and regular monitoring of patients’ prothrombin time-international normalized ratio (PT-INR) levels to optimize anticoagulation outcomes.
Future research should incorporate standardized INR quality control protocols to minimize inter- and intra-center variability in laboratory measurements. Additionally, the establishment of external quality assurance systems across laboratories is essential to enhance the reliability and comparability of INR data.
To improve the generalizability of findings, multicenter or national-level studies are recommended. These would provide a more comprehensive understanding of anticoagulation control practices and reflect regional differences in clinical and laboratory settings across Nepal.
It is also crucial that future studies systematically record and analyze bleeding and thrombotic events, particularly in relation to sub-therapeutic and supra-therapeutic INR levels, to better understand the clinical implications of poor anticoagulation control.
The adoption of prospective study designs with regular INR monitoring and patient follow-up will enable the collection of more accurate and actionable data regarding the effectiveness and safety of warfarin therapy.
Future prospective studies include detailed temporal tracking of INR values alongside adverse clinical events to better assess causality between INR fluctuations and bleeding outcomes.
Finally, patient education and adherence support programs should be strengthened to emphasize the importance of regular INR monitoring and compliance with warfarin therapy. These efforts may help maintain therapeutic INR ranges and reduce the risk of adverse events.
Footnotes
Acknowledgments
We thank to the Manmohan Cardiothoracic Vascular and Transplant Center for granting me permission to conduct this study and for providing access to the necessary resources and data. We are also grateful to all the healthcare professionals and administrative staff who assisted me in collecting and verifying patient records. Our special thanks go to the patients and their families, whose cooperation and willingness to participate in this research were essential for its successful completion
Ethical Considerations
Manmohan Cardiothoracic Vascular and Transplant Center and Institute of Medicine, Institutional Review Committee granted ethical clearance for this study with a reference number of 51(6-11) E2 and 171080/81 respectively. Study participants’ confidentiality and anonymity were kept by omitting patient identifications such as name or any other personal data.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing Statement
The corresponding author will provide the original data set supporting the study's findings upon reasonable request.