
Abstract
Background:
Oral anticoagulation therapy with vitamin K antagonists (VKA) such as warfarin and acenocoumarol is recommended in patients with atrial fibrillation (AF) and risk factors for embolism. The quality of anticoagulation control with VKA may be assessed by the time in therapeutic range (TTR). In our country, there are no data available about the quality of anticoagulation in patients with AF. The primary goal of our study was to assess the level of effective anticoagulation in a multicenter network of anticoagulation clinics in Argentina, which included patients with nonvalvular AF (NVAF) treated with VKA oral anticoagulants.
Methods:
The TERRA trial is a multicenter, cross-sectional study involving 14 anticoagulation clinics that were invited to participate and recruit 100 consecutive patients with NVAF treated with VKA for more than 1 year. The international normalized ratio (INR) values were retrospectively obtained from patient charts, and TTR was calculated using the Rosendaal method.
Results:
A total of 1190 patients were included in the analysis. Mean age was 74.9 ± 9.9 years, and 52.5% of the patients were male. Median TTR was 67.5% (interquartile interval 54-80). During 55% of the TTR, INR was >3. Interinstitution variability was substantial, with a range of 57.7% ± 17% to 87.7% ± 17%, P < .001. The 10th percentile of TTR was 41%, the 20th percentile was 50%, the 30th was 58%, and the 35th percentile was 60%. In 40% of patients, TTR was <70%.
Conclusion:
In this multicenter study, mean TTR values in patients with AF under VKA were similar to those in international therapeutic clinical trials (55%-65%). Marked variations among institutions were observed and, although average results obtained were high, one third of the patients exhibited a TTR below 60%. This cutoff value is conservative according to current recommendations, and guidelines suggest that when management with VKA cannot be improved, patients should be switched to direct oral anticoagulants. The addition of TTR calculation to clinical practice may help improve the quality of oral anticoagulation in patients with AF, thus improving anticoagulation outcomes.
Introduction
Oral anticoagulation therapy with vitamin K antagonists (VKAs) such as warfarin or acenocoumarol is a strong evidence-based recommendation for patients with atrial fibrillation (AF) and risk factors for embolic events. Clinical trials that assessed the efficacy of VKA against placebo showed a 64% reduction in the incidence of stroke and a 26% decrease in mortality. 1 In recent years, direct oral anticoagulants (DOAs, formerly called “new oral anticoagulants”) have been developed, in some cases with better results than VKA in terms of reduction in mortality, embolic events and bleeding, or at least with results noninferior to VKA. 2 Current recommendations of clinical practice guidelines are inconsistent; some consider DOAs as the first option, while others consider them to be similar to VKA. 3,4,5 However, they agree that DOAs should be prescribed in patients who do not wish to undergo routine international normalized ratio (INR) monitoring controls or when regular controls do not result in adequate anticoagulation. The quality of VKA control can be assessed by means of the percentage of INR within range, mean INR, and time in therapeutic range (TTR). 6 Although the results obtained by the 3 methods are obviously interrelated, they are quantitatively different. 7 The TTR is calculated based on the INR obtained in periodic blood samples of patients, using linear interpolation method of Rosendaal. 6 As a result, the daily INR value can be estimated, together with the percentage of days with adequate protection (targeted INR between 2 and 3) and the time exposed to a higher risk of bleeding or embolic events, that is, an INR below 2 or above 3, respectively. In clinical trials, the risk of bleeding or stroke has been correlated with adequate anticoagulation control using TTR. 8,9
In classic clinical trials that established the benefits of oral anticoagulation with warfarin, TTR averaged 64%, and in recent clinical trials, the range was between 55 and 64%. 10,11,12,13 Acenocoumarol is the VKA most often used for anticoagulation therapy in Argentina, and it is commonly used in other countries as well. 14
In Argentina, some health care institutions have reported data about TTR levels in a population treated with acenocoumarol, but there was no community registry available to provide data reflecting routine clinical practice. Furthermore, in anticoagulation clinics, TTR is not calculated routinely (partly due to limited access to the appropriate software) and is not usually taken into consideration when modifying or selecting an anticoagulation treatment.
The primary goal of our study was to assess the level of effective anticoagulation in a multicenter network in Argentina, in patients with nonvalvular AF under oral anticoagulation with acenocoumarol or warfarin, and followed with TTR measurements using a simple electronic spreadsheet adapted to the daily practice of hemostasis laboratories.
Materials and Methods
The TERRA (Tiempo en Rango en la Republica Argentina) trial was a cross-sectional multicenter registry. A total of 14 institutions with anticoagulation clinics were invited to participate. To avoid bias, we recommended that all institutions include the first 100 patients with nonvalvular AF under VKA who attended their periodic anticoagulation control, and INR levels were retrieved retrospectively for the previous 12 months. Patients had to meet the following inclusion criteria: Have received oral anticoagulation therapy for more than 1 year. The first 3 months of VKA administered de novo were excluded from the analysis, given that measured values are known to be unstable during that initial period. Have had at least 8 control monitoring visits during the year prior to the enrollment visit. Be older than 21 years old. Have AF not associated with rheumatic valve disease. Have AF not associated with prosthetic valves.
At the same time, a log-book was completed, entering the first 200 consecutive patients who attended their INR control visit and recording the reason for anticoagulation. If the reason was AF, the record had to state whether the patients would be included and, if that was not the case, the reason for exclusion.
Collection of Information and Data Sources
For data collection, a special electronic record designed by one of the authors (CT) for the study was used, which included an automatic calculator of TTR levels using Rosendaal formula and was validated against regular calculators with full concordance in 100 patients. An electronic form was provided to each center (see Appendix Figure B1). When patients came to their visits, INR values, dates, and drug doses from the previous 12 months were obtained from their charts.
The Study and Associated Ethical Issues
The study was conducted according to personal information privacy policy established by local, national, and international regulations and in conformance with the Guidelines for Good Epidemiology Practices. Record confidentiality was observed. The study protocol was approved by each of the participating institutions’ Ethics Committees. Some committees requested the participants to sign an informed consent while others did not, and the decision of each institution’s authorities was respected.
Demographic Data and Other Parameters
The reason for anticoagulation due to AF was recorded, that is, primary prevention or secondary prevention after peripheral embolism or stroke. Other demographic data were sex, age, and embolic or hemorrhagic complications in the previous year.
Statistical Analysis Plan
Assessment of Study Variables
Quantitative data were expressed as mean and standard deviation or median and interquartile interval (IQI), according to their distribution. The main variable of interest was TTR, calculated for each patient. The calculation was repeated by modifying the desired range to INR values of 1.9 to 3.1. We explored the correlation of TTR with age and percentage of visits within therapeutic range (number of visits with an INR between 2 and 3 by total number of visits) with Pearson correlation coefficient and linear regression and compared TTR levels according to gender and between institutions with nonparametric tests (Wilcoxon rank-sum test and Kruskal-Wallis 1-way analysis of variance).
Statistical Power and Size of the Sample
The expected TTR value was 64% and the desired 99% confidence interval (CI) ± 4% was 60 to 68. The necessary sample size to obtain the stated CI was estimated in 1009 patients.
Results
Vitamin K Agonists Therapy for Any Cause, Prevalence of AF, and Patient Selection for the TERRA Registry
Of the 14 participating institutions, 11 completed the log-book reporting the first 200 patients who attended the center to check their INR value for any cause and ultimately collected data on 2605 patients under VKA (Table 1); 50.2% of the visits were due to AF, acounting for a total of 1307 patients. Among them, 798 (61%) patients were included in the TERRA registry. The most common cause for exclusion was recent onset of anticoagulation. A total of 476 patients with AF included in the TERRA registry were enrolled by the other 3 institutions or by the same 11 institutions after completing their first 200 patients. Hence, a total of 1274 patients (798 + 476) were included in the prospective AF registry; of these, the organizing committee excluded 84 because they attended fewer than 8 annual visits. The remaining 1190 patients comprised the population analyzed in the registry.
Reasons for Anticoagulation in Anticoagulation Outpatient Clinics According to the Logbook.a
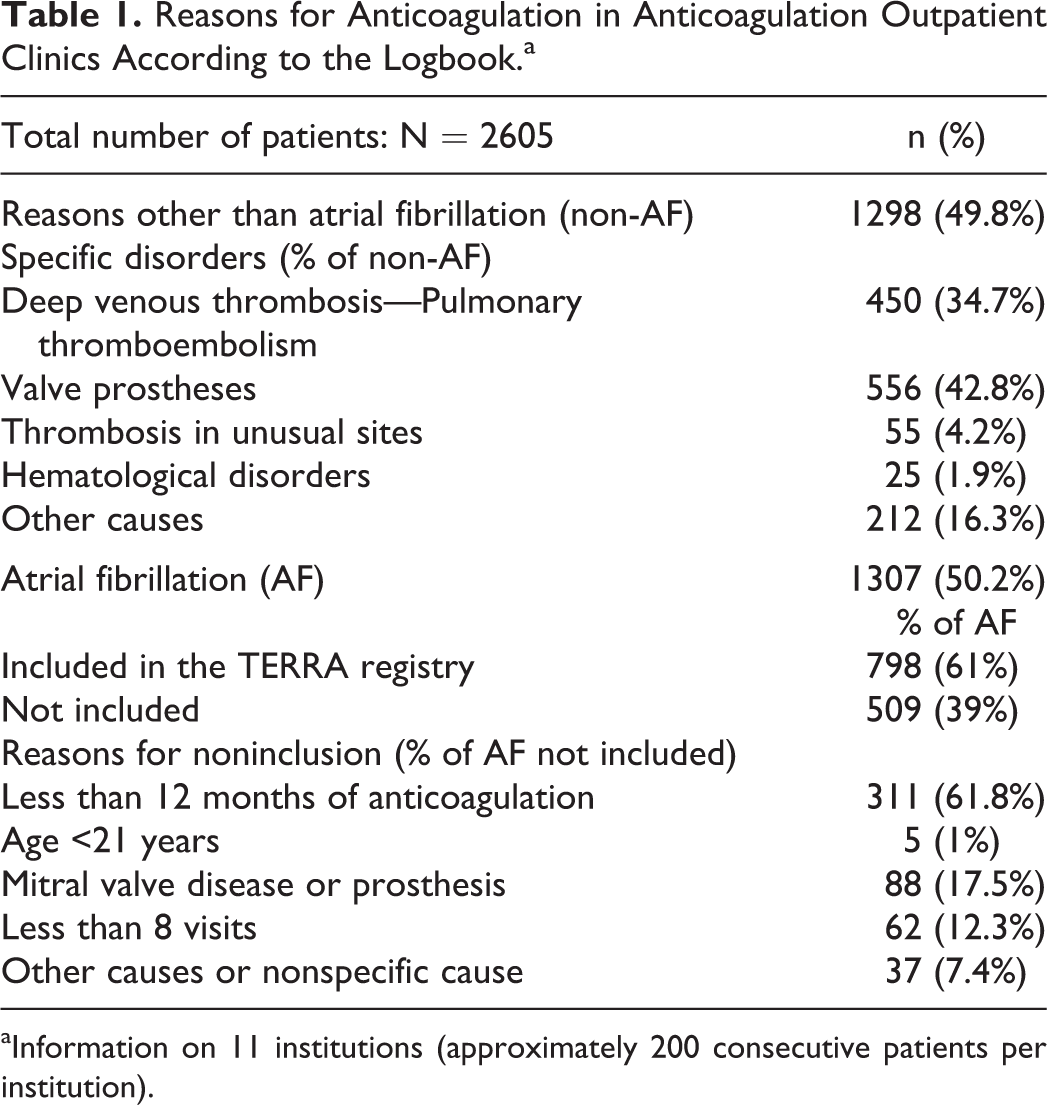
aInformation on 11 institutions (approximately 200 consecutive patients per institution).
Demographic Data and Adverse Events
Table 2 summarizes the main demographic characteristics of the patients included and the reasons for anticoagulation. Hemorrhagic and embolic complications in the 12 months prior to the enrollment visit were reported: 7 (0.6%) patients had a stroke, 9 (0.8%) patients had a transient ischemic attack (TIA), and there were no peripheral embolic events. Gastrointestinal hemorrhage occurred in 7 (0.6%) cases and 1 (0.1%) patient had an intracranial hemorrhage. Because of the retrospective nature of our study, the design does not allow for and was not intended to establish any relationship between INR or TTR values and the complications reported.
Demographic Variables and Reason for Anticoagulation due to AF.a
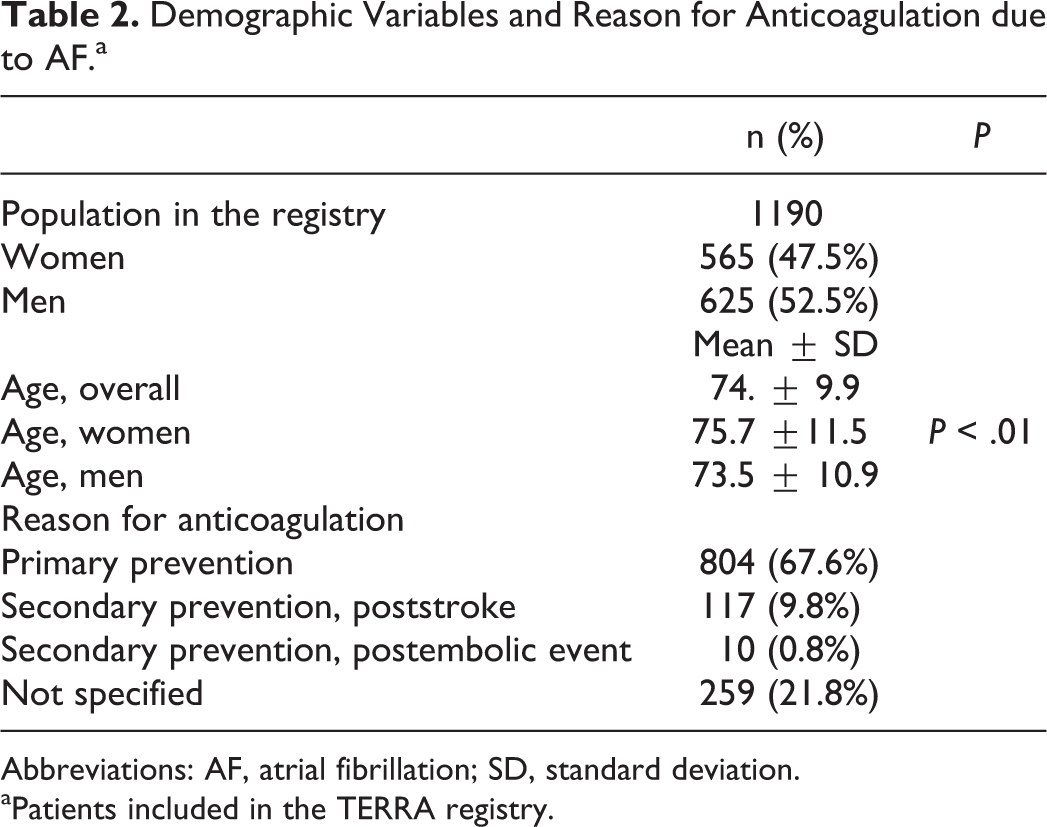
Abbreviations: AF, atrial fibrillation; SD, standard deviation.
aPatients included in the TERRA registry.
Levels of TTR
The median value of monitoring visits with INR dosage was 11 (IQI 10-12). Median TTR was 67.5% (IQI 54-80). The interinstitution difference in TTR was statistically significant. Figure 1 shows the medians and IQI of TTR levels per institution, where obvious differences are observed (Supplementary Table 1A summarizes TTR levels, both overall and for each institution). When time percentage out of range was analyzed, a slight predominance was noted in time with an INR above 3, accounting for 55% of the out of range time against 45% of the time with an INR below 2. Median TTR in the 84 patients excluded by the organizing committee was 73.6% (IQI 51-93).
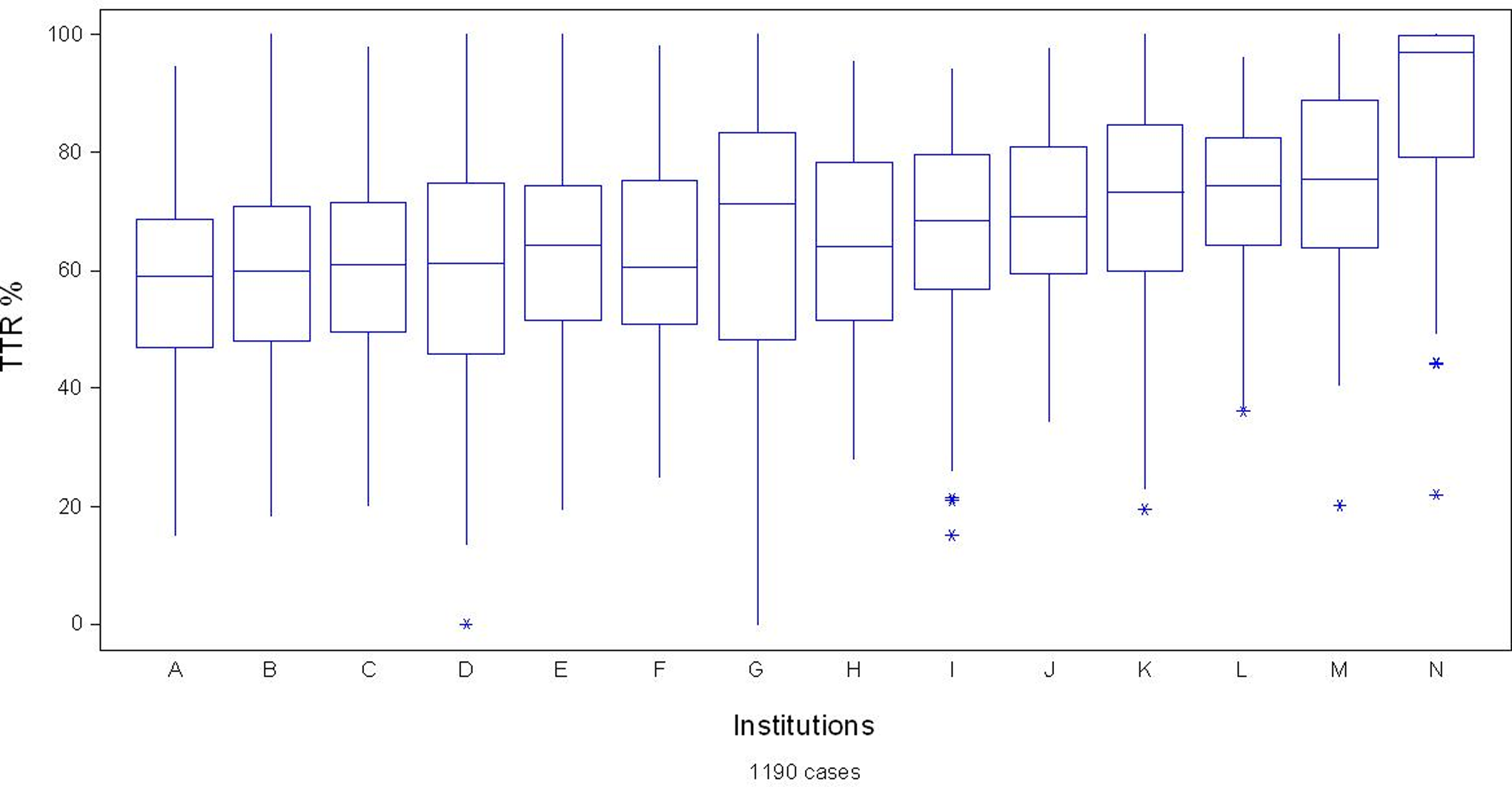
Box and Whisker Plot showing the median and interquartile interval of time in therapeutic range (TTR) levels in the 14 participating institutions.
Time in Therapeutic Range and its Correlation With Other Variables
No correlation was found between TTR and age or sex distribution (median TTR was 66.4% in women and 66.8% in men, P = .65). More patients were treated with acenocoumarol (1112, 93.4%) than with warfarin (78, 6.6%), while no differences were observed in TTR levels between both drugs (acenocoumarol 66.8% vs warfarin 64.2%, P .49).
The percentage of visits with an INR level between 2 and 3 (60%) correlated highly with the TTR measured using Rosendaal method (66.6%). Correlation and regression analyses showed an r coefficient of .869, P < .001 (data are plotted in Figure 2). In spite of this substantial correlation, individual prediction varied markedly, as can be visually inferred from the graph, where the dots are distributed vertically. For example, a patient with 60% of visits within range may exhibit a TTR that is quite variable, between 40% and 80%, thus invalidating this method as a predictor of adequate anticoagulation.
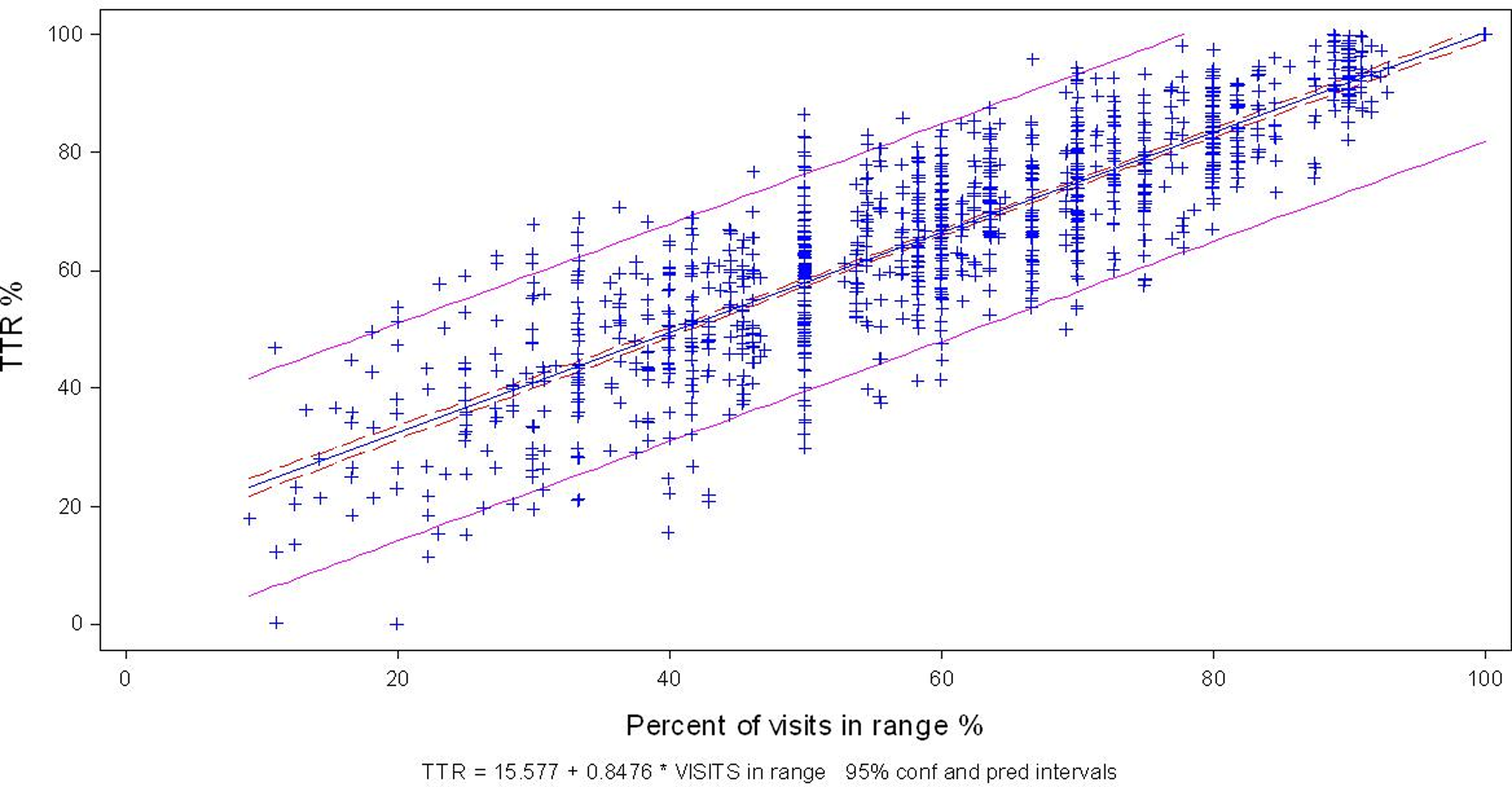
Individual prediction of time in therapeutic range (TTR) according to visits within range.
Analysis of Time Out of Range and Institutional Trends
During the time out of range, there was a slight predominance of INR values above 3 compared to values below 2. We explored whether this pattern differed between institutions and thus explained the variation in TTR (Supplementary Table 2A summarizes these findings). The interinstitutional difference in time out of range was statistically significant, with a P value < .001. The percentage of time with an INR below 2 varied between 28.6% and 69%, and, as shown in Figure 3, no correlation trend between institutional TTR values was observed.
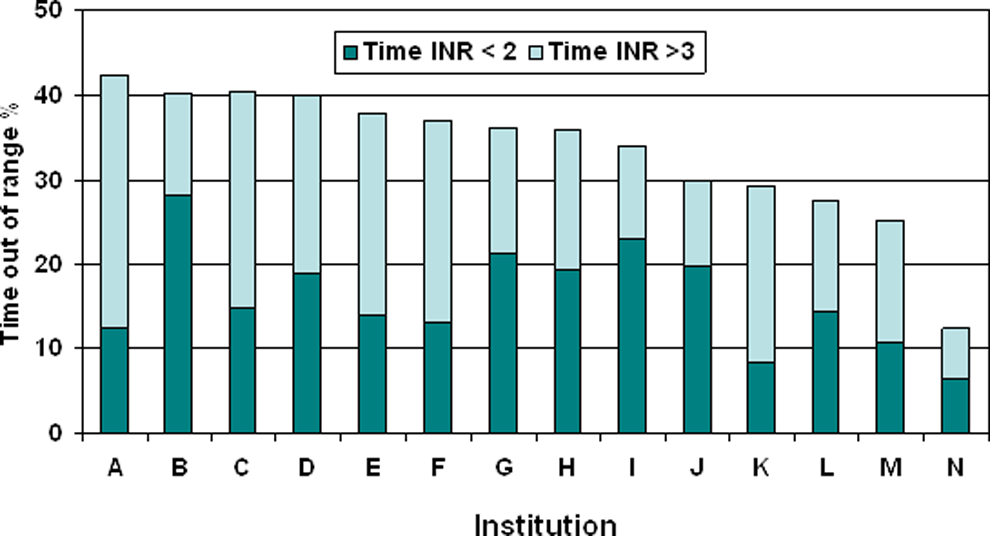
Correlation between the time out of range and its components, time with an international normalized ratio (INR) <2 and with an INR >3, and its distribution among institutions. There is no clear trend, although a noticeable interinstitutional variation can be observed.
Change in TTR Levels When Modifying the INR Threshold to 1.9 to 3.1
Table 3 summarizes the variations in TTR percentages considering INR values between 2 and 3 as adequate (classic approach) and then changing acceptable values to 1.9 to 3.1. With the classic calculation, TTR was <50% in 20% of the patients, <60% in 35% of the patients, and <70% in 55% of the patients. When these criteria were modified, that is, INR values of 1.9 to 3.1 were used, patients with a TTR <50% accounted for only 10%, those with a TTR <60%, for 20%, and those with a TTR <70%, for 40% of the study population.
Change in TTR When the Acceptable INR Threshold is Modified.
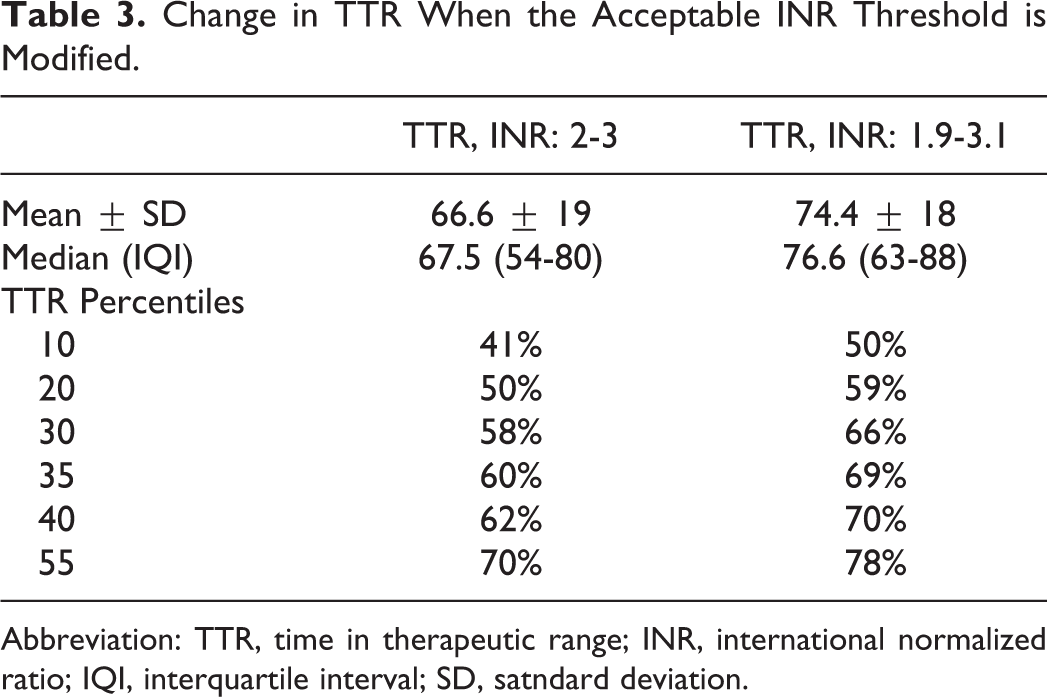
Abbreviation: TTR, time in therapeutic range; INR, international normalized ratio; IQI, interquartile interval; SD, satndard deviation.
Discussion
Our registry, involving a network of health-care institutions with anticoagulation clinics, has shown that the median value of TTR is 67.5%. This level of control compares well against international standards. Results showed substantial interinstitutional variations, while in most centers TTR values exceeded 60%.
The TTR levels are useful to assess the quality of treatment with VKA in the individual patient as well as for the global assessment of a group of patients treated. In previous studies, a clear correlation was observed between TTR and the risk of bleeding or embolism. In the SPORTIF III and V trials, patients with a TTR below 60% had a higher mortality and greater incidence of bleeding. 15 Embolic risk increases exponentially when INR levels are lower than 2. A case–control study in patients with ischemic stroke showed that, compared to an INR between 2 and 3, an INR of 1.9 increased the risk of stroke by 20% and an INR of 1.8 increased the risk by 50%. 16 A more recent study in a larger population showed that the annual incidence of stroke was 0.6% with INR values of 2 to 3, and increased 3-fold to 1.9% when INR values were between 1.5 and 1.9. 17 In the ACTIVE-W study (Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events), in which warfarin was better than the combination of aspirin and clopidogrel for the prevention of embolism in patients with AF, the benefit was only observed in institutions that achieved a median TTR above 58% to 65%. 8
The TTR has been explored in several controlled studies assessing VKA therapy, originally versus aspirin or placebo, and later in large comparative studies with DOAs. With the exception of the ROCKET-AF trial, mean TTR has remained above 60% in all the aforementioned trials (Table 3A in the supplementary material summarizes the most relevant trials of the last decade). Given the unique conditions in which controlled clinical trials are conducted, these TTR levels may be difficult to attain in daily practice. The TTR levels in patients from Argentina who participated in the ARISTOTLE (Apixaban for Reduction In STroke and Other ThromboemboLic Events in Atrial Fibrillation), ROCKET-AF (Rivaroxaban Once daily, oral, direct Factor Xa inhibitionCompared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation), and RELY (Randomized Evaluation of Long-term anticoagulant therapY) international trials were 72%, 63%, and 69.5%, respectively, that is, similar to those obtained in our study. 10,11,12
A meta-analysis published in 2008 showed that TTR in international trials with a retrospective cohort design (n = 22 studies) was 59% (29%-75%), whereas in prospective cohort studies (n = 5 studies), TTR was 61% (56%-66%). 18,19,20 Compared to these data and those of other observational studies, our median TTR of 67.5% can be considered consistent with international standards (results of several international observational studies are summarized in Supplementary Table 4A). Some of these registries, such as the National Swedish Registry, have reported TTR values close to 75%, a much higher value than that shown even in randomized controlled trials. 21
Our findings only reflect the practice in centers with hemostasis specialists, which is the predominant form of anticoagulation control in Argentina. We have no data available regarding the number of patients whose anticoagulation is controlled by general practitioners (GPs) or their outcomes. One registry that assessed INR levels in patients who consulted the emergency department for various reasons and had chronic AF reported that, in Latin America, only 44% of patients had an INR within a range of 2 to 3. 22 The TTR in specialized anticoagulation centers or clinics is usually higher than that obtained with routine clinical management by family physicians, internists, or GPs. A meta-analysis reviewed all randomized or cohort studies that measured INR systematically in patients under VKA (n = 50 000) and reported that TTR in randomized studies was 12.2% higher than in general practice. Also, TTR in specialized centers was higher than in the setting of routine clinical management, with a difference close to 8%. 23 Median TTR value with routine clinical management was 50%. This finding was confirmed by another meta-analysis of 8 studies conducted in the United States, which included 22 237 patients. Overall, TTR was 55% (95% CI: 51%-58%) and was higher in specialized centers, that is, 63% (95% CI: 58%-68%) compared to 51% (95% CI: 47%-55%) with routine clinical management. 24 The ISAM study reported similar findings. 25,26
Can These Results Contribute to Improved Clinical Practice?
In our country, most institutions use paper records or preprinted cards so that treatment can be assessed both visually and qualitatively. The transition to electronic medical records may contribute to the overall assessment of VKA effect in terms of the individual patients as well as the institution.
The percentage of visits in range does not adequately assess TTR level. Although both parameters exhibit a high correlation, detailed analysis shows a substantial dispersion in the individual patient. This information may help us analyze the potential impact of the recommendations included in international guidelines regarding our local practice.
In the ARISTOTLE trial, in patients treated with warfarin, annual incidence of stroke or embolic events was 1.75% for centers with TTR <58%, 1.3% for centers with TTR values between 58% and 66%, and 0.83% for centers with TTR >72%. 27 In this case, the relative benefit of apixaban compared to warfarin was maintained in the 4 quartiles, but the absolute benefit was greater when the institutional TTR was lower. The trend was similar in the RELY study with dabigatran: In patients with TTR below 53.6% (first quartile), the incidence of embolic events was 2.34%, whereas in the 2 upper quartiles, with TTR above 67%, the incidence was 1.34% per year. 13
The new guidelines differ in several respects but agree that patients with inadequate control of INR levels, despite adequate adherence to VKA treatment should be switched to DOA agents.
The criterion of inadequate control is not rigid or consistent. Two recent meta-analyses 28,29 assessed the correlation between TTR observed in clinical trials of warfarin compared to DOAs and the occurrence of clinical events. Using a TTR of 65% as cutoff point, the following was noted: (1) the effect on the prevention of stroke and embolism was independent of TTR, but the absolute reduction in events favored DOA when TTR was <65%; (2) a greater reduction in bleeding was seen with DOA, but only with TTR values <65%, hazard ratio (HR) 0.75, whereas not with TTR >65%, HR 1; (3) total mortality decreased 9% overall, 15% when TTR was below 65%, and only 3% when TTR was above this value. The 65% criterion was adopted for the purpose of the meta-analyses, and it was analyzed in each quartile for each individual drug, as mentioned earlier. In both meta-analyses, the effect is inconsistent for the different therapeutic agents.
These results have been translated into clinical practice guidelines with different recommendations: the European Guideline considers a TTR of 70% as adequate, the Spanish Guideline uses the criterion of less than 65%, 30 and others provide more generic recommendations. 5 In our study, as shown in Table 3, 55% of patients had a TTR below 70%, in half of them TTR was below 67%, and in approximately one-third it was below 60%. Even when the acceptable INR values were modified to less stringent levels (1.9-3.1), 35% of the population in our database still had TTR levels below 65%.
In our study, analysis of TTR showed that an important percentage of patients exhibit, on average, suboptimal levels of control with VKA, and values are distributed inconsistently among the different institutions.
At the institutional level, a low mean TTR implies that we have an opportunity to assess new treatment algorithms and their efficacy. 31 Algorithms to establish how frequently patients should attend control visits and how VKA doses should be changed influence TTR levels. 32
At the individual level, a low TTR helps us to carefully review adherence to treatment and concomitant external factors, such as the diet or drug interactions that might explain such low values. More frequent controls might be an alternative for these unstable patients to ensure a higher TTR. When patients adhere well to treatment and nevertheless do not obtain adequate TTR levels, an alternative is to prescribe DOAs.
Limitations of the Study
This study has several limitations. The intention to explore TTR levels in patients with good adherence to treatment implies the exclusion of patients with poor adherence. Additionally, the retrospective design with a single prospective visit excludes patients who have had severe complications during the previous year, which could have resulted in a change in their treating physician or hindered their outpatient visits. Assessment of such patients would have required a prospective cohort design. Highly stable patients were also excluded, since in some institutions they were monitored every 2 to 3 months and therefore did not attend the minimum number of control visits required for inclusion. Median TTR in the 84 patients excluded from the analysis because of less than 8 visits in the previous 12 months was 73.6%, that is, higher than the median TTR in the 1190 study patients.
In our study, TTR results represent centers with hemostasis specialists, which is the main modality for treatment control in Argentina and thus do not reflect patients whose anticoagulation control is conducted by GPs. With this design, however, it is highly unlikely that we underestimate the percentage of TTR that can be obtained in specialized centers. The assumption that such patients, even with this treatment regimen, are still not within adequate range conveys a very relevant message for clinical purposes as well as for the planning of treatment improvement strategies.
Conclusion
The multicenter TERRA trial has allowed us to know the mean TTR levels in a network of Argentine institutions with hemostasis specialists. These results compare well to other studies in the literature, albeit with noticeable inter-institutional variations. The electronic worksheet was well accepted and may be used in daily practice as an aid to assess individual patients. Its regular use may help demonstrate that a certain percentage of patients does not obtain an adequate TTR, despite good treatment adherence and requires a more thorough clinical follow-up or a change in therapeutic strategy, that is, switching to a DOA. From the institutional standpoint, information regarding TTR levels contributes to control performance, which can help increase awareness regarding the need to make changes or introduce self-corrective measures, as well as to prospectively assess the impact of such measures.
Footnotes
Appendix A
Appendix B
Authors’ Note
TERRA study authorities. Director: Carlos Daniel Tajer. Scientific Committee: José Ceresetto (Hospital Británico), Federico J. Bottaro (Hospital Británico), Marcelo Casey (Instituto Fleni), Alejandra Martí (Hospital El Cruce).
This report was delivered as a lecture at the XI Argentine Conference on Thrombosis and Hemostasis held in Buenos Aires in September 2014. The study was awarded the first prize.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grants and Financial Support: This protocol was proposed by a group of independent Argentine investigators who received a grant from the Bristol-Myers Squibb-Pfizer Partnership, coded CV-185-260.
Supplemental Material
The supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.