
Abstract
This retrospective, descriptive study aimed to assess hematologic testing practices in 100 patients with preeclampsia undergoing neuraxial blockade (NB). Prior to NB, platelet (PLT) count was performed in 61 (98%) of 62 women in labor and in 37 (97%) of 38 women undergoing cesarean delivery (CD). No patients had a pre-NB PLT count <70 × 109/L. Pre-NB tests for prothrombin time (PT) and activated partial thromboplastin time (APTT) were less common and varied among laboring patients (15 [24%] of 62) and patients prior to CD (18 [47%] of 38). Prior to NB, PT and APTT values were within normal limits in all patients. The time intervals between laboratory testing and NB ranged from <2 to >12 hours. The lack of consistency in pre-NB coagulation testing and the variable time intervals between laboratory tests and NB may be due to a lack of consensus among anesthesiologists for determining “safe” hemostatic conditions for NB placement in patients with preeclampsia.
Introduction
Laboratory tests of platelet (PLT) count, prothrombin time (PT), and activated partial thromboplastin time (APTT) are relatively common in patients with preeclampsia. 1 –5 Although a low incidence of severe thrombocytopenia and coagulopathy has been reported in patients with mild and severe preeclampsia during the peripartum period, 6 –8 thrombocytopenia and coagulopathy are important risk factors for the development of epidural hematoma following a neuraxial anesthetic technique, which include single-shot spinal, epidural, or combined spinal–epidural techniques. 9
The indications for laboratory testing of PLT, PT, and APTT in all patients with preeclampsia undergoing neuraxial anesthesia during the peripartum period are unclear. The most recent American Society of Anesthesiologists (ASA) practice guidelines recommend obtaining PLT in patients with suspected preeclampsia. 10 However, there are no recommendations for timing preanesthesia laboratory tests prior to neuraxial blockade (NB) or on the indications for concomitant preanesthesia coagulation testing in patients with preeclampsia. As a result, these decisions are often at the discretion of the primary anesthesiologist. Time delays may occur due to the perceived need to request tests of PLT and coagulation function close to the time of neuraxial block placement, which may unduly affect patient care by subsequently delaying adequate labor analgesia. Furthermore, anesthesiologists may be reluctant to use a neuraxial anesthetic technique in a patient with preeclampsia requiring urgent or nonelective cesarean delivery without recent preoperative laboratory tests, which may culminate in the use of a general anesthetic and a higher potential risk of patient comorbidity (cerebral hemorrhage following endotracheal intubation). 11
To the best of our knowledge, no studies to date have specifically investigated the timing of laboratory tests performed prior to de novo NB in preeclamptic women in the peripartum period. The primary aim of this single-center, retrospective study was to evaluate preanesthesia PLT and coagulation indices in patients with preeclampsia who receive de novo NB for labor analgesia or nonelective cesarean delivery.
Patients, Materials, and Methods
After gaining institutional review board approval, we identified a convenience sample of preeclamptic patients admitted to Lucile Packard Children’s Hospital (LPCH) between January 2009 and August 2009. The LPCH is a university hospital and tertiary obstetric center with >4000 deliveries per year. During the study period, the labor and delivery unit at LPCH did not have formal departmental guidelines for laboratory tests prior to NB in patients with preeclampsia, and orders for laboratory tests are requested by obstetricians or obstetric anesthesiologists on a case-by-case basis.
Patients
We searched an institutional electronic data warehouse using administrative codes (specifically International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM]) for preeclampsia and hypertensive disease of pregnancy to initially identify our patient cohort. Participants were identified using the following search criteria: mild or unspecified preeclampsia (ICD-9-CM: 642.4), severe preeclampsia (ICD-9-CM: 642.5), preeclampsia, or eclampsia superimposed on preexisting hypertension (ICD-9-CM: 642.7). We subsequently reviewed the medical records of patients identified from the initial electronic search. Based on manual chart review, the final study cohort was identified according to the following inclusion criteria: patients with preeclampsia or HELLP syndrome (hemolysis, elevated liver enzymes and low platelet count) undergoing either a trial of labor or nonelective cesarean delivery receiving de novo NB (which includes an epidural, single-shot spinal, or combined spinal–epidural technique). For the purposes of this study, we did not define epidural anesthesia using an epidural “top-up” for cesarean delivery in patients with a preexisting epidural catheter as a de novo neuraxial block. Exclusion criteria included patients with preeclampsia undergoing elective (scheduled) cesarean delivery; intrauterine fetal death; patients <18 years old; patients receiving anticoagulant or antithrombotic drugs; patients with a previous history of thrombocytopenia, history of acquired or inherited coagulopathy, chronic hypertension, or nephropathy. Clinical and laboratory data were abstracted from the medical records for all patients included in the final study cohort.
Methods
During medical chart review, mild preeclamptic participants were identified using current diagnostic criteria defined by the American College of Obstetricians and Gynecologists 12 –14 :≥2 systolic blood pressure (SBP) readings ≥140 mm Hg or diastolic blood pressure (DBP) readings ≥90 mm Hg and ≥+1 protein on urine dipstick evaluation or >300 mg protein excretion in a 24-hour urinary sample. Severe preeclampsia was defined according to the presence of 1 or more of the following criteria: ≥2 SBP readings ≥160 mm Hg or DBP ≥110 mm Hg or evidence of end organ damage (≥3 g proteinuria in 24 hours or ≥+3 protein on urine dipstick evaluation, central nervous system, pulmonary or liver dysfunction, epigastric pain, or evidence of fetal compromise). We also separately documented laboratory and clinical data for patients with HELLP syndrome, based on the following diagnostic criteria 15,16 :PLT < 150 × 109/L, aspartate transaminase >40 U/L, alanine transaminase >60 U/L (diagnosis of hemolysis by peripheral blood smear or low serum haptoglobin if measured).
During medical record review, we recorded demographic, obstetric data, and neuraxial anesthetic interventions. We recorded the highest maternal SBP values, and data on proteinuria (24-hour urinary protein excretion, urinary protein dipstick evaluation within 1 week prior to delivery) to determine the severity of preeclampsia during the peripartum period or prior to nonelective cesarean delivery. Preneuraxial block laboratory data abstracted were PLT, PT, and APTT. We also recorded the lowest PLT and the highest PT, APTT, blood urea nitrogen, creatinine levels measured between 48 hours before delivery to 48 hours after delivery. For the purposes of this study, this time period was defined as “the peri-delivery period.”
Laboratory PLT, PT, and APTT measurements are performed in the Stanford University Medical Center Clinical Laboratories. The PLT is measured using one of the following instruments: Coulter LH 750 or LH 780 hematology analyzers (Beckman Coulter, Inc, Brea, California); CELL-DYN Sapphire or CELL-DYN 1800 hematology analysers (Abbott Laboratories, Abbott Park, Illinois). Both PT and APTT are measured using the STA-R Evolution Expert Series Hemostasis System (DiagnosticaStago, Inc, Parsippany, New Jersey).
Our primary outcome measures were to evaluate hematologic indices (PLT, PT, and APTT) in patients receiving de novo NB for labor analgesia or de novo neuraxial anesthesia for nonelective cesarean delivery. Secondary aims were to assess the time intervals between laboratory testing and neuraxial block placement and to examine potential relationships between clinical/biochemical parameters and intrapartum hematologic indices.
Statistical Analysis
Data are expressed as mean (SD), median (interquartile range), and number or percentages as appropriate. Normal distribution was determined using QQ plots and the Kolmogorov-Smirnov test. Pearson and Spearman correlation coefficients were used to assess the correlation between individual hematological indices with biochemical parameters and clinical parameters (highest SBP and DBP, 24-hour urinary protein levels) relevant to preeclampsia. Microsoft Excel (Microsoft Corporation, Redmond, Washington) was used for data entry, and IBM SPSS Version 19 (IBM Corporation, Somers, New York) was used for data analyses; P < .05 was considered statistically significant.
Results
The initial electronic search identified 271 patients with ICD-9 codes for preeclampsia, and 100 patients met the inclusion criteria for the final study cohort (Figure 1 ). Patient demographic, obstetric, and delivery data are summarized in Table 1 . In the study cohort, 75 patients underwent a trial of labor, with most women (50 [67%] of 75) ultimately having a spontaneous or assisted vaginal delivery (Table 1). Neuraxial blockade was performed for labor analgesia in the majority of patients undergoing a trial of labor (62 [83%] of 75; the remainder (13 [17%] of 75) did not receive neuraxial analgesia during a trial of labor but ultimately received a neuraxial technique for cesarean delivery. Fifty patients underwent cesarean delivery, with an equal number of women (25 [50%] of 50) experiencing and not experiencing labor (Table 1). For patients undergoing cesarean delivery, 38 (76%) of 50 received a de novo neuraxial anesthetic technique, 11 (22%) of 50 underwent epidural anesthesia using the preexisting labor epidural (epidural “top-up”) and 1 of 50 (2%) underwent general anesthesia. For patients receiving labor analgesia and neuraxial anesthesia for cesarean delivery, details of the de novo neuraxial techniques performed and disease categories (mild preeclampsia, severe preeclampsia, and HELLP syndrome) are presented in Table 2 . The majority of patients undergoing NB for labor or nonelective cesarean delivery (>90%, respectively) were diagnosed with mild or severe preeclampsia (Table 2).
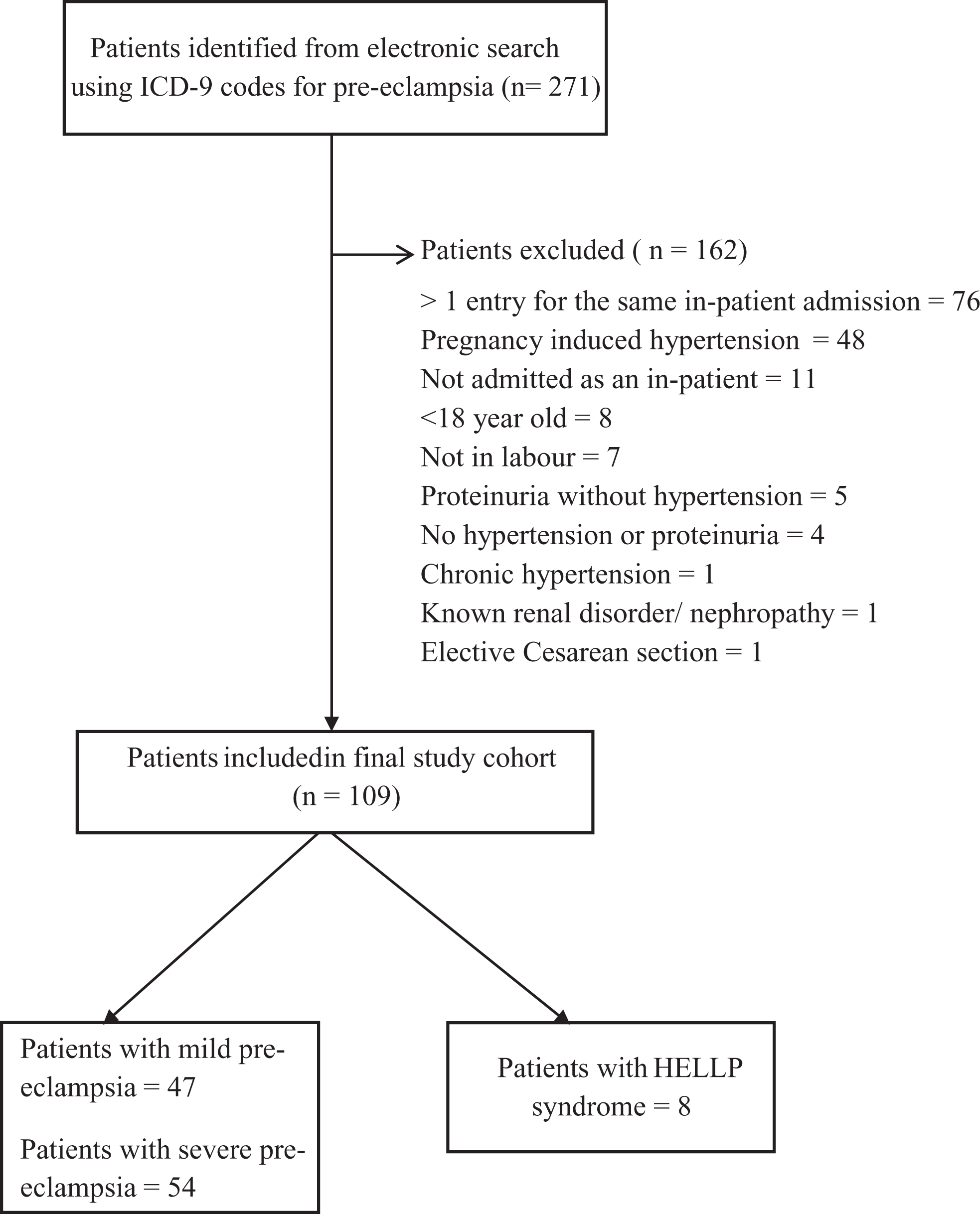
Flow diagram summarizing patient selection for the initial and final study cohort.
Maternal Demographic and Obstetric Data.a

Abbreviations: BMI, body mass index; SD, standard deviation.
a Data presented as n (%), mean (SD), and median (interquartile range).
b n = 96 patients.
c Twenty-five women underwent nonelective cesarean delivery with labor; 25 women underwent nonelective cesarean delivery without labor.
Data on Severity of Preeclampsia and Anesthetic Technique in Patients Undergoing De Novo Neuraxial Blockade for Labor Analgesia and Cesarean Delivery.a
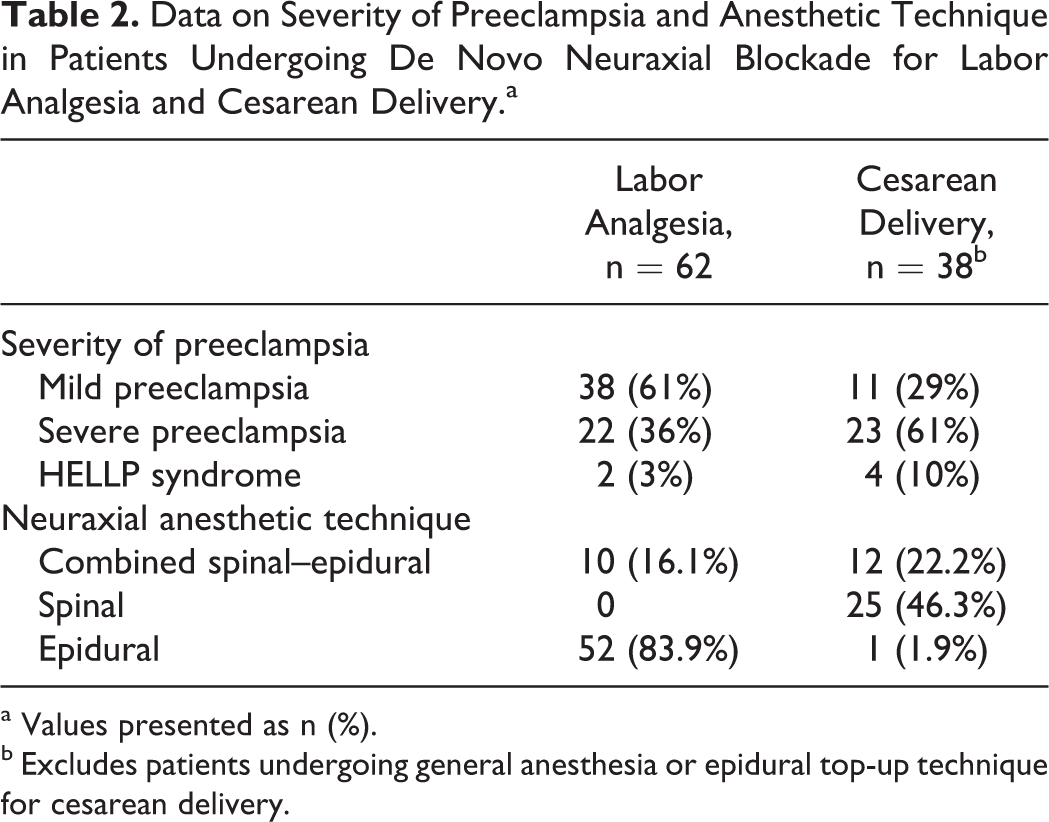
a Values presented as n (%).
b Excludes patients undergoing general anesthesia or epidural top-up technique for cesarean delivery.
Laboratory data for patients who received neuraxial labor analgesia and patients who underwent neuraxial anesthesia with a de novo technique for cesarean delivery are presented in Table 3 . The distribution of preblock platelet counts in all patients, according to disease severity (mild preeclampsia, severe preeclampsia, and HELLP syndrome), that received a de novo neuraxial technique are presented in Figure 2 . A preanesthesia PLT was performed in the majority of women (98%) receiving NB for labor analgesia, and in 97% women undergoing neuraxial anesthesia for cesarean delivery. No patients had a recorded PLT <70 × 109/L prior to neuraxial block for labor analgesia or cesarean delivery (our departmental threshold for performing NB). One patient with HELLP syndrome received a spinal anesthetic for cesarean delivery but did not have a recorded preblock laboratory tests. This patient experienced a massive postpartum hemorrhage requiring transfusion of 9 units of packed red blood cells and 4 units of platelets. The initial postoperative hematologic indices were PLT = 23 × 109/L; PT = 15.8 seconds, and APTT = 34.1 seconds. The patient did not incur any neurological deficit or epidural hematoma in the postpartum period.
Hematologic Indices and Timing of Laboratory Results in Patients Receiving Neuraxial Block for Labor Analgesia and Cesarean Delivery.a
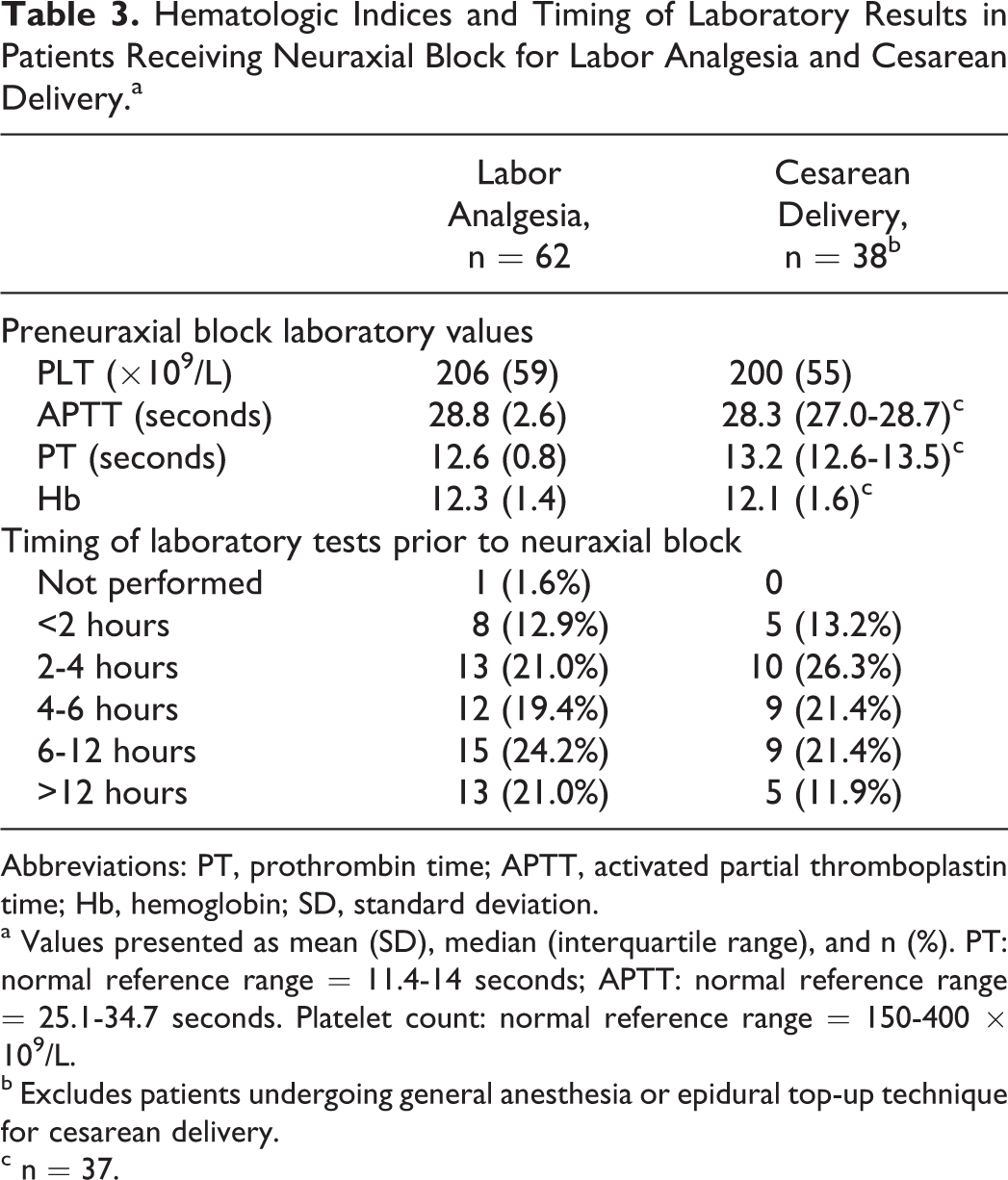
Abbreviations: PT, prothrombin time; APTT, activated partial thromboplastin time; Hb, hemoglobin; SD, standard deviation.
a Values presented as mean (SD), median (interquartile range), and n (%). PT: normal reference range = 11.4-14 seconds; APTT: normal reference range = 25.1-34.7 seconds. Platelet count: normal reference range = 150-400 × 109/L.
b Excludes patients undergoing general anesthesia or epidural top-up technique for cesarean delivery.
c n = 37.
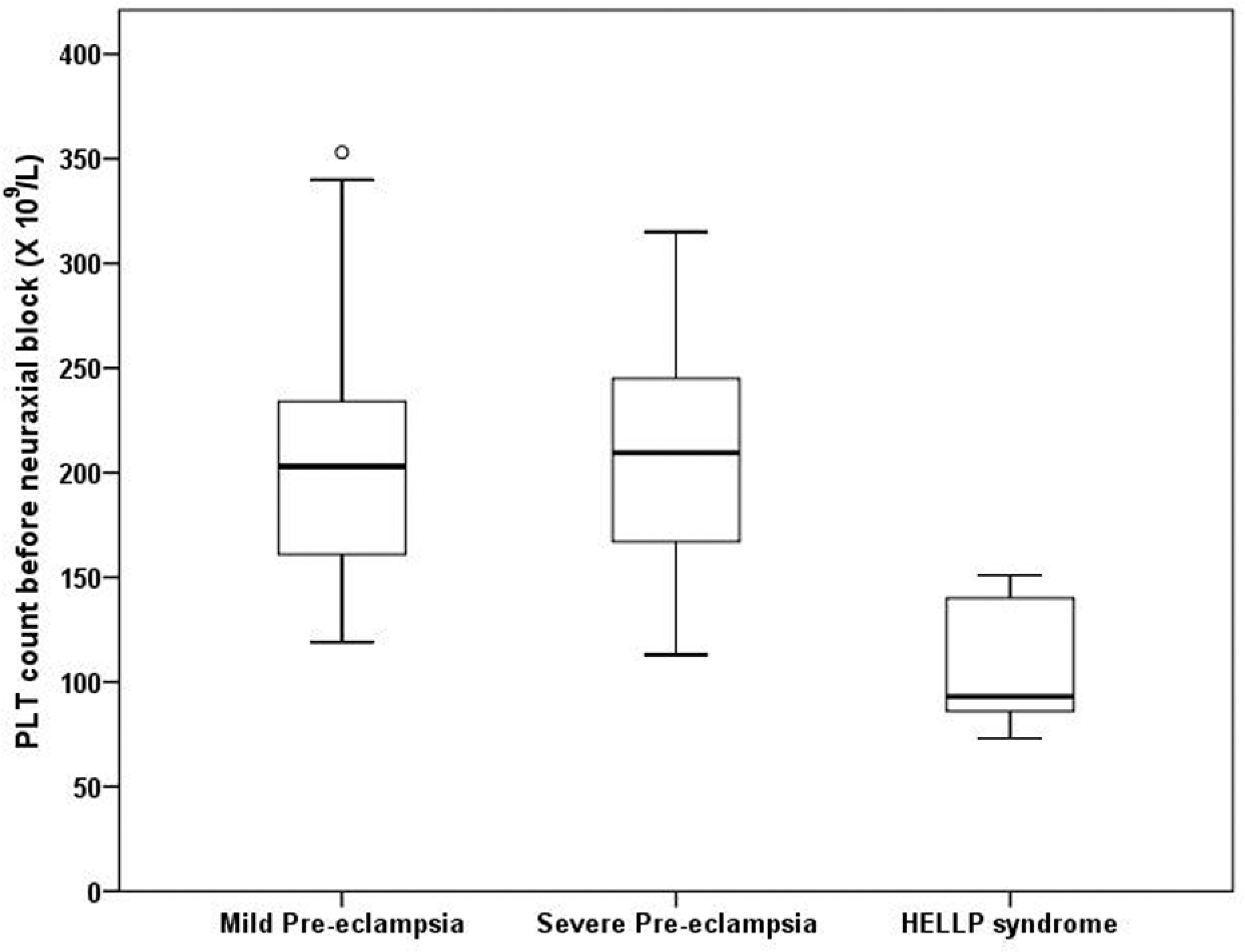
Median (interquartile range) in platelet counts for patients with mild preeclampsia, patients with severe preeclampsia, and patients with HELLP syndrome receiving de novo neuraxial blockade. Horizontal line denotes median values, box borders refer to interquartile range, whiskers indicate range of values, and circle indicates outlier (>1.5 times the interquartile range).
Coagulation tests (PT and APTT), prior to NB for labor, were performed in 24% women, and all patients had preblock PT and APTT values within normal limits. Coagulation tests were performed in nearly half of the women who underwent de novo NB (47%) for cesarean delivery; PT and APTT values were within normal limits for all patients.
The timing of the preanesthesia laboratory tests for NB for labor and cesarean delivery is shown in Table 3. We observed marked variability in the time intervals between laboratory testing and placement of an NB, with preblock intervals varying from <2 to >12 hours.
We found no significant correlations between individual clinical parameters (highest SBP, highest DBP, or 24-hour urinary protein values) with individual hematological values (lowest PLT, highest PT, or highest APTT; P > .05). However, we observed significant negative correlations between the lowest PLT and the highest APTT (r = −.25; P =.038) and highest PT values (r = −.264; P = .032) and between the highest APTT and highest PT values (r = .947; P < .001).
Discussion
In this retrospective study, severe thrombocytopenia (PLT <70 × 109/L) was not detected in any of the patients with preeclampsia in this study cohort prior to NB. Nearly all patients with preeclampsia receiving NB for labor analgesia (97%) or cesarean delivery (98%) had a PLT recorded prior to anesthesia, which is in keeping with ASA guidelines. However, preblock coagulation testing in labor or cesarean delivery in patients with preeclampsia undergoing NB occurred in fewer patients and was more variable (incidence = 24% and 47%, respectively). Marked variability was also observed in the time intervals between laboratory testing and neuraxial block placement in all patients. The lack of consistency in performing coagulation testing and the variability in the time intervals between laboratory tests and NB may be related to subjective variability among anesthesiologists for determining “safe” hemostatic conditions for neuraxial block placement.
In our study, no patients with mild or severe preeclampsia undergoing NB had clinically significant thrombocytopenia (PLT <70 × 109/L) or prolonged PT or APTT values. These results suggest that the patients with mild or severe disease may have peripartum hematologic and coagulation indices within an acceptable range for performing NB. Our results are similar to those of Barker et al and Trotter et al who reviewed predelivery PLT and laboratory coagulation tests in patients with preeclampsia. 6,8 In the cohort of Barker of over 400 patients with preeclampsia who underwent coagulation testing prior to delivery, 90% had a PLT >100 × 109/L and coagulation indices within a predefined normal range; PLT <100 × 109/L occurred in 9% of all cases, all of whom were diagnosed with severe preeclampsia. 6 Similarly, an audit of 176 coagulation screens performed by Trotter et al reported that no preeclamptic patients with PLT >150 × 109/L were found to have abnormal coagulation. 8 However, no specific details were provided in either study detailing the timing of laboratory testing prior to NB.
No patients received NB with a preblock PLT <70 × 109/L, which suggests that neuraxial anesthetic practice is in keeping with our departmental guidelines or that anesthesiologists at our institution have similar PLT thresholds when considering NB. Although there is no consensus with regard to a PLT threshold below which NB is contraindicated for patients with preeclampsia, surveys of anesthesiologists' preferences for performing neuraxial block in nonpreeclamptic patients with thrombocytopenia suggest the threshold above which neuraxial block can be performed is between 50 and 100 × 109/L. 17,18,19 Our predetermined departmental PLT threshold of 70 × 109/L for performing NB is within this range. Furthermore, guidelines from the American College of Obstetricians and Gynecologists state that healthy parturient with PLT between 50 and 100 × 109/L may be considered for regional anesthesia. 20
In our study, the presence of preblock coagulation studies was less common than platelet counts. We speculate that anesthesiologists order fewer tests of coagulation indices prior to NB compared with platelet counts in patients with preeclampsia. Our results are consistent with those of a previous survey of obstetric anesthesia directors' preferences for coagulation testing in patients with preeclampsia. 21 In this survey, variation in the need for preblock coagulation testing was reported among respondents; 20% of anesthesiologists would order coagulation tests for patients with mild preeclampsia and 75% of anesthesiologists would order these tests for patients with severe preeclampsia. 21
One patient with HELLP syndrome received a spinal anesthetic for cesarean delivery without preanesthesia laboratory tests and had prolonged PT (15.8 seconds) and profound thrombocytopenia (23 × 109/L), after receiving a massive transfusion, in the postoperative period. In this case, the preoperative hematologic and coagulation indices were unknown. Rapidly decreasing PLT is a characteristic feature of HELLP syndrome. 22,23 In addition, a previous study reported a 30% incidence of coagulopathy in patients with HELLP syndrome. 19 Although the incidence of spinal hematoma among the obstetric population is rare, a population-wide study by Moen et al identified 2 obstetric patients, both with HELLP syndrome, who developed spinal hematomas after receiving NB. 24 Our case emphasizes the importance of close hematological monitoring prior to neuraxial anesthesia in patients with HELLP syndrome and the need to individualize the decision to perform NB in patients with HELLP syndrome.
In our study, there was marked variability in the time intervals between laboratory testing and NB. We speculate that the lack of consensus about the recommended time intervals for preblock laboratory testing and the resulting variation in anesthesiologists' preferences on our labor and delivery unit contributed toward the marked variability in the time intervals between laboratory testing and neuraxial block placement. As a result, it is possible that patients with mild preeclampsia may experience delays in receiving labor analgesia due to apprehension by the anesthesiologist about proceeding with NB in the absence of a “normal” PLT ± PT/APTT. However, preblock hematological laboratory testing is justified in patients with severe preeclampsia and HELLP syndrome due to the higher potential for hematological derangement in these patient subpopulations.
We observed significant correlations between the lowest PLT and the highest PT and APTT values. Previous work has shown that an inverse relationship exists between platelet count and antithrombin III activity 25 and that fibrinopeptide A concentrations are elevated in preeclampsia only when significant activation of platelets occurs. 26 These results support a low grade disseminated intravascular coagulation (DIC) picture in the presence of severe preeclampsia, which may contribute to an inverse relationship between lowest PLT and highest PT/PTT values. However, our study was not powered to assess individual relationships between biochemical indices, clinical parameters, PLT, PT, and APTT in preeclamptics, and future work is needed to formally assess these relationships.
Limitations of this study include the retrospective nature of our study design. It is possible that we did not identify all patients with preeclampsia in our initial search due to ICD-9 miscoding for preeclampsia. The inclusion of data on urinalysis to determine proteinuria was incorporated into the inclusion criteria as not all patients had 24-hour urine collection to confirm proteinuria of >300 mg/d or >3 g/d. Although 24-hour urinary protein studies are known to be more accurate than urinalysis in determining proteinurea in pregnancy, 27 we feel that our data reflects clinical practice as clinical care often needs to be delivered acutely for obstetric patients with preeclampsia before 24-hour urinary protein results become available. Preanesthesia coagulation tests were performed in 24% of laboring patients and 47% of patients undergoing cesarean delivery (undergoing a de novo anesthetic), therefore it is uncertain whether coagulation abnormalities existed in patients with preeclampsia within our study cohort, who did not receive preanesthesia coagulation testing. We note that other studies have reported variable incidences of thrombocytopenia (PLT <100 × 109/L), prolonged PT, and prolonged APTT during pregnancy in patients with preeclampsia: 2% to 19%, 2,7,28 0% to 16%, 2,5 and 1.3% to 2.5%, 2,5 respectively. We were unable to deduce whether anesthesiologists were primarily involved in ordering laboratory tests prior to anesthetic intervention. As a result, it is uncertain whether the requests for laboratory tests were made by the obstetric or the anesthesia team, nor whether the anesthesia team made specific requests regarding the timing of laboratory testing prior to anesthetic intervention. Lastly, these data are sourced from a single, obstetric tertiary-care center with 24 hours in-house attending obstetric anesthesia coverage. Therefore, preblock hematological testing and obstetric/anesthesia practices may vary at other academic and nonacademic institutions.
In conclusion, we observed no evidence of clinically significant thrombocytopenia (<70 × 109/L) or coagulopathy in patients with mild or severe preeclampsia who underwent NB. However, due to a lack of consensus, inconsistencies exist in the practice of preblock coagulation testing and in the time intervals between laboratory testing and NB. Population-wide studies incorporating comparative effectiveness research and cost–benefit analyses 29 are needed to ascertain the indications, timing, and relevance of laboratory testing prior to NB in patients with preeclampsia.
Footnotes
Acknowledgments
We wish to acknowledge the assistance and support of researchers within the Stanford Center for Clinical Informatics (Stanford University School of Medicine) for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was internally funded by Stanford University School of Medicine