
Abstract
Introduction
Women with von Willebrand Disease (VWD) frequently experience heavy menstrual bleeding (HMB), impacting their health and quality of life. Hormonal contraceptives are a standard treatment.
Aim
We hypothesized that women with type 1 VWD using hormonal therapy would have lower bleeding scores and potentially higher VWF levels than non-users. To test this, we compared demographics, VWF levels, and International Society on Thrombosis and Haemostasis Bleeding Assessment Tool (ISTH-BAT) scores between hormone users and non-users in the Zimmerman Program cohort.
Methods
Data from 269 women with type 1 VWD enrolled in the Zimmerman Program were analyzed. Of these, 103 were hormone users, including oral contraceptives (71), medroxyprogesterone acetate (11), levonorgestrel IUD (11), contraceptive implant (3), and the etonogestrel/ethinyl estradiol vaginal ring (1) and (6) subjects were undergoing hormone replacement therapy. Participants who were postmenopausal were excluded from the study results.
Results
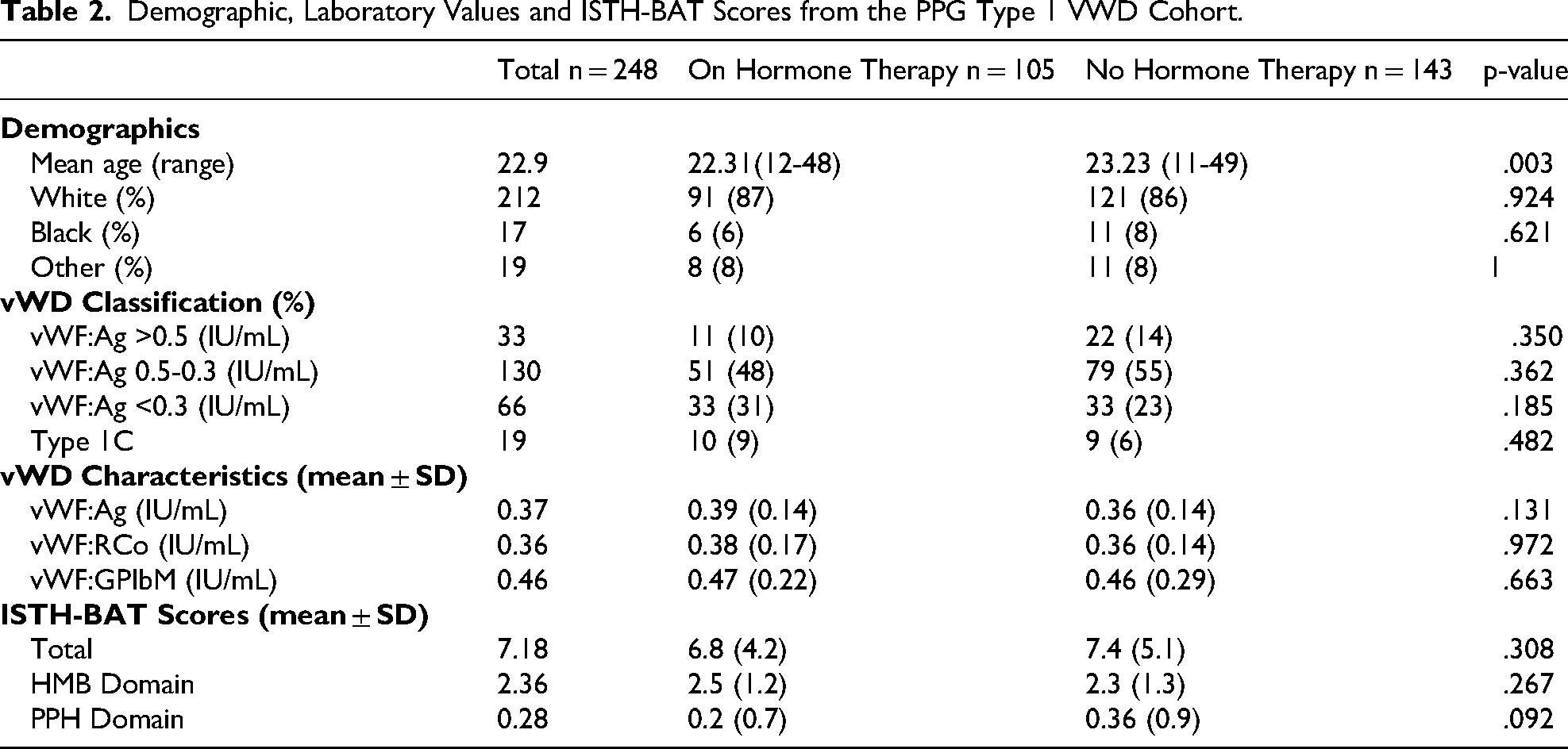
HMB was reported by 252 out of 269 participants (94%), with 118 (47%) reporting severe symptoms. While hormone users were younger than non-users, 22.3 versus 23.2 years, (p = .003), VWF levels were similar between groups, (0.36 vs 0.38IU/mL). Age-adjusted BAT scores revealed that in all age groups, more than 70% of patients had abnormal bleeding scores.
Conclusion
Hormonal therapy users had lower total BAT scores compared to non-users, though differences were not statistically significant. These findings suggest a potential but limited effect of hormone use on bleeding phenotype in women with type 1 VWD.
Keywords
Introduction
Von Willebrand Disease (VWD) is an inherited bleeding disorder caused by qualitative or quantitative abnormalities of von Willebrand factor (VWF). 1 Type 1 VWD, the most common subtype, accounts for approximately 75% of cases and is characterized by VWF antigen and activity levels of less than 0.5 IU/mL. 2 Although the incidence of VWD is similar in men and women, women experience a greater burden of bleeding symptoms due to reproductive hemostatic challenges, including heavy menstrual bleeding (HMB). 3 The American College of Obstetricians and Gynecologists (ACOG) defines HMB as “excessive menstrual blood loss that interferes with a woman's quality of life”. 4 HMB affects 20%–50% of women of reproductive age, but it impacts 50%–92% of women with VWD. 5
Heavy menstrual bleeding (HMB) significantly impacts quality of life, leading to reduced productivity, frequent school and work absences, and potential complications such as iron deficiency and iron deficiency anemia. 6 Per current ASH ISTH NHF WFH guidelines, 2 hormonal therapy—including combination oral contraceptives (COCs), progestin-only agents, intrauterine devices (IUDs), implants, and vaginal rings, is recommended as first-line treatment for HMB in patients with VWD. Hormonal therapy can profoundly affect the coagulation system, influencing VWF levels and activity. 7 Estrogens increase VWF production and release, while progestins exert a lesser effect. 8 Estrogen doses vary by preparation and route of administration, and over time, the dose of estrogen in contraceptives has decreased to reduce thromboembolism risk. 9 While hormonal therapy is a mainstay of VWD HMB management, the relationship between VWD and patient-specific factors and the decision to use hormonal therapy remains poorly understood.
Given the frequent use of hormonal therapy to manage HMB in women with VWD, it is essential to better understand how disease severity affects treatment decisions and influences clinical outcomes. This study utilized data from the Zimmerman Program (NHLBI HL081588), a multicenter natural history study funded by the NHLBI, which collects standardized clinical and laboratory data from a cohort of individuals with VWD. We hypothesized that women using hormonal therapy would have lower bleeding scores and potentially higher VWF levels due to treatment effects. Despite the established efficacy of hormonal therapy in managing HMB in these patients, its effect on bleeding assessment tools (BATs) remains unclear. Hormonal contraceptives, typically used as first-line treatment for HMB, are known to increase VWF activity (RCoF/GPb1 M) and antigen (Ag) levels. Therefore, this study aimed to compare patient-specific variables, disease characteristics, and BAT scores between type 1 VWD women, receiving hormonal therapy and those who did not, within the Zimmerman Program cohort.
Materials and Methods
Study Design
This study design was a retrospective, cross-sectional analysis. We hypothesized that women using hormonal therapy would have lower ISTH-BAT scores and higher VWF levels compared to non-hormone users. Data were collected from women enrolled in the Zimmerman Program for the Molecular and Clinical Biology of VWD, a natural history study (NHLBI HL081588). Data collected at enrollment included demographic information, medication history, and laboratory results. Our goal was to identify differences in patient characteristics, disease-specific factors, and bleeding assessment tool (BAT) scores between women with type 1 VWD who were on hormonal contraceptives and those who were not.
Participants
Participants in this study were women enrolled in the Zimmerman Program for the Molecular and Clinical Biology of VWD (PPG). A pre-existing diagnosis of type 1 VWD was required for study entry, and women who provided menstrual history data were selected for analysis. Subjects who did not meet laboratory criteria at the time of enrollment were included if they had a previous diagnosis of type 1 VWD. The participants were divided into two groups: those using hormonal contraceptives (including oral contraceptive pills, injectable progestins, hormone replacement therapy, intravaginal devices, and intrauterine devices [IUDs]) and those who were not. To focus on the use of hormonal contraceptives for menstrual bleeding, subjects over age 50 were excluded.
Variables
The primary exposure of interest was hormonal contraceptive use, categorized as users or non-users. The primary outcomes were ISTH-BAT scores (total score, heavy menstrual bleeding [HMB] score, and postpartum hemorrhage [PPH] score) and VWF levels (VWF:Ag, VWF:RCo, and VWF:GPIbM). Potential confounders considered were age, BMI, and other medications known to affect bleeding (eg, anticoagulants, antiplatelet agents).
Study Size
A power analysis was not conducted for this retrospective analysis. The sample size was determined by the number of eligible participants enrolled in the Zimmerman Program during the study period who had complete data for the variables of interest. While we acknowledge the limitations of not having a prospective power calculation, the sample size of 269 participants was deemed sufficient to detect clinically meaningful differences in ISTH-BAT scores and VWF levels.
Statistical Analysis
Demographics, VWD testing results (VWF:Ag, RCoF/GPIbM), and ISTH-BAT scores (total, HMB, and postpartum hemorrhage [PPH]) were compared between groups by descriptive statistics. Continuous variables were compared between groups using a two-sample t-test, while categorical variables were analyzed using Fisher's exact test. A two-sided p-value of <.05 was considered statistically significant.
Results
In total, 269 women reported experiencing menstrual cycles. The cohort was predominantly composed of pediatric and young adult participants, with a mean age of 25.3 years (range: 11-76). The majority of the cohort (86%) identified as White. Based on laboratory testing, 153 women (57%) were diagnosed with VWF levels between 0.3–0.5 IU/mL, 57 women (21.2%) had VWF levels <0.3 IU/mL, and 26 women (9.7%) were classified with type 1C VWD (clearance-type VWD). Of the remaining subjects, 32 women (12%) were diagnosed with VWF levels between 0.5-0.6 IU/mL and 6 women (2%) had VWF levels >0.6 IU/mL. The mean VWF level for the entire cohort was 0.37 IU/mL (SD 0.14 IU/mL), while the mean vWFlevel was 0.36 IU/mL (SD 0.15 IU/mL).
ISTH-BAT scores in menstruating women of this cohort ranged from 0 to 29 points, with a mean of 7.6 points (SD 5.1). Evaluation of the HMB domain of the ISTH-BAT revealed that 94% (253) of the women who reported HMB had more than 1 point on the 4-point scale, with a mean of 2.4 points. Of these, 47% (119) reported severe HMB (scoring 3 or 4 points). At the time of enrollment, 103 women (40.1%) were using hormonal contraceptives, including oral contraceptive pills, medroxyprogesterone acetate, levonorgestrel IUD, contraceptive implant, hormone replacement therapy and the etonogestrel/ethinyl estradiol vaginal ring. Bleeding severity and VWF levels vary by therapy type
Bleeding Scores and von Willebrand Factor Levels by Hormonal Therapy Type.

After excluding women presumed to be postmenopausal (age > 50) l, 103 hormone users and 143 non users were analyzed. The distribution of ISTH-BAT scores by hormonal treatment status is shown in

Total ISTH-BAT Scores of Women with Type 1 VWD by Hormonal Therapy Treatment Status. Note: The purple color indicates regions of overlap between hormone user and non-hormone user groups.

Patients were Divided by Age Groups and BAT Scores were Analyzed. Q1 (11-18) Represents the Group of Subjects Under 18, in which a Bleeding Score >2 is Considered Abnormal. Q2 and Q3 Represent Subjects with Ages Between (18-30) and (31-41) Respectively, in which a Bleeding Score >4 is Considered Abnormal. Q4 Represents the Oldest Group of Patients (42-52), in which a Bleeding Score >5 is Considered Abnormal. Age Ranges (Q2-Q4) are Based on Those Proposed by Doherty et al. 11
Demographic, Laboratory Values and ISTH-BAT Scores from the PPG Type 1 VWD Cohort.
Discussion
We examined a cohort of women with type 1 von Willebrand Disease (VWD), specifically focusing on the impact of hormonal therapy on bleeding severity, as measured by ISTH-BAT scores. The cohort consisted of young women, predominantly white (86%), with a mean age of 25.3 years. The majority of women (69.1%) had VWF activity levels between 0.3–0.5 IU/mL, which is consistent with mild to moderate VWD. These results align with those reported by Flood et al (2016), 10 whose sample taken from the Zimmerman Program was 85% Caucasian with an average VWF level of 47 IU/dL. Notably, patients with VWF levels above 0.5 IU/mL were included due to the nature of the participants in the Zimmerman Program, which enrolls individuals with a historical diagnosis of VWD, even if they do not meet laboratory criteria at the time of enrollment. This approach reflects real-world clinical practice and acknowledges the clinical variability in VWF levels over time, ensuring our findings are representative of the broader population of individuals with a history of VWD. The ISTH-BAT scores varied significantly, reflecting the heterogeneity in bleeding symptoms across patients. One limitation of using ISTH-BAT as the sole marker of bleeding severity is the potential saturation of scores within specific domains, such as HMB, and the lack of hemostatic challenges in pediatric populations. 9 Some of the challenges that limit the ISTH-BAT were addressed using the age adjusted ranges proposed by Doherty et al. 11 Their data suggests that normal aging leads to an increased variability of bleeding scores, related not only to increases in the menorrhagia domain scores in women with HMB but also to an increase in score of post-procedure bleeding due to increased exposure to procedures with age.
Another finding was the high prevalence of heavy menstrual bleeding (HMB), with 94% of women reporting HMB symptoms and 47% suffering from severe HMB. These percentages are consistent with those reported by de Wee et al, 12 who found that 85% of their cohort in the Netherlands reported HMB symptoms. Interestingly, the HMB-specific BAT score was higher in hormone users. This likely reflects selection bias, as patients with more severe symptoms may have been more likely to receive hormonal therapy.
Comparing women hormone users with non-users, several observations were made. Women on hormonal contraceptives were younger on average (22.3 years) than those not on hormonal contraceptives (23.2 years), suggesting that younger women might be more likely to use hormonal treatments, presumably for both contraceptive and therapeutic purposes. Despite the age difference, other disease features, such as VWF levels and bleeding severity in specific ISTH-BAT domains, were not significantly different between the groups. Interestingly, women on hormonal contraceptives had lower total ISTH-BAT scores (6.8) compared to those not using contraceptives (7.4). However, this difference was not statistically significant. The lack of significant differences between groups suggests that while hormonal contraceptives may moderately reduce overall bleeding symptoms, they may not fundamentally alter the clinical profile of women with VWD. This highlights both the need for better outcome measures than ISTH BAT as well as additional therapeutic options, particularly for women with severe HMB. While this study was not powered for subgroup comparisons, descriptive trends suggest that oral contraceptive users had higher VWF levels and lower BAT scores, these trends may reflect differences in systemic versus local hormonal effects. Given the small sample sizes in most categories, these findings should be interpreted cautiously. Nonetheless, they underscore the need for future studies to evaluate the differential impact of hormonal regimens on bleeding burden in women with VWD.
These findings are consistent with previous studies showing variable effects of hormonal contraceptives on bleeding symptoms in women with VWD. James et al 13 found that hormonal contraceptives can reduce menstrual blood loss in women with bleeding disorders, but the extent of benefit varies widely among individuals, with reductions ranging from 35%–69%. Our study supports this variability and suggests that while hormonal contraceptives may provide some benefit, they are not equally effective for all women with VWD. The variability in response may be influenced by individual differences in VWF levels, the severity of the underlying disorder, or hormonal regulation pathways.
Additionally, recent studies on the use of recombinant von Willebrand Factor (VWF) and tranexamic acid for HMB in VWD patients provide further context. Ragni et al (2023) 14 conducted a randomized crossover trial to assess the efficacy of recombinant VWF and tranexamic acid in managing HMB in VWD patients. While neither treatment normalized Pictorial Blood Assessment Chart (PBAC) scores, tranexamic acid significantly reduced PBAC scores compared to recombinant VWF. Despite not meeting the primary objective, tranexamic acid was associated with a larger reduction in menstrual blood loss, suggesting it may be a more effective option for controlling HMB in VWD patients.
Other studies are exploring alternative treatment options for VWD patients. Sidonio et al (2023) 15 described the efficacy of prophylactic von Willebrand factor/factor VIII concentrate. Kiss et al 16 extrapolated data from the Sidonio study and determined that patients receiving continuous prophylaxis experienced a 43% reduction in PBAC scores, decreasing from a mean of 227 with on-demand treatment to 131 with prophylaxis.
There are several limitations to this study. Historical VWF levels were not available for analysis. The indication and duration of hormonal therapy are also unknown, limiting our ability to assess treatment intention or duration-effect relationships. We could not control for personal, cultural, or contraceptive motivations for hormone use, which may affect bleeding patterns independently. This may be a potential confounding factor as it would influence bleeding patterns and severity which would be reflected in these patients’ BATs. Sequential BATs were not performed, as this was a cross-sectional study. This limits our ability to draw conclusions regarding the impact of HT on bleeding symptoms. The effect of age on VWF levels was not controlled in our analysis. Age-related increases in VWF may confound the results of BATs. BMI and concurrent medications (eg, antifibrinolytics, DDAVP) were not adjusted for in this analysis and may influence bleeding scores. The cohort was predominantly White (86%), which may limit generalizability of our findings. Given that Black women have higher rates of HMB, often due to fibroids, and may be underdiagnosed with VWD, there is a need for more diverse cohort studies to ensure broader applicability of results. These limitations highlight the need for caution when interpreting out findings and suggest that future studies should consider longitudinal designs and improved control for potential confounders.
Our study highlights the high prevalence of HMB in women with VWD and suggests that while hormonal contraceptives may offer symptom relief, the variability in response underscores the need for more sensitive markers of HMB and personalized treatment approaches. Given the high prevalence of HMB and the variability in response to hormonal contraceptives, a personalized treatment approach is essential for improving outcomes in this population. Future research should focus on optimizing individualized management strategies to address the diverse needs of women with VWD.
Conclusion
Among women with Type 1 VWD experiencing heavy menstrual bleeding, von Willebrand factor levels were similar between hormonal contraceptive users and non-users, with mean levels of 0.36 IU/mL and 0.38 IU/mL, respectively. Additionally, while the total ISTH-BAT scores indicated a trend towards higher scores in hormone users (6.8) compared to non-users (7.4), this difference was not statistically significant (p = .308). These findings suggest that despite the common use of hormonal therapy, it does not significantly alter VWF levels or bleeding severity in this population, highlighting the need for more tailored treatment approaches to effectively manage HMB in women with VWD.
Footnotes
Acknowledgements
The authors thank the women who participated in the Zimmerman Program for the Molecular and Clinical Biology of VWD for their time and contribution to this research. We are grateful to the clinical and research staff at participating institutions for their dedication to patient care and data collection. We also thank the investigators of the Zimmerman Program for their collaborative efforts and continued commitment to advancing the understanding of von Willebrand Disease.
Ethical Considerations
This study was conducted in accordance with relevant institutional and national guidelines and was approved by the Institutional Review Board at the University of Pittsburgh. The data analysis, manuscript preparation, and submission were conducted per established ethics guidelines, and all involved followed best publishing practices per ICJME.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nicoletta Machin has received research funding from Takeda USA and serves on advisory boards for Sanofi and Star Therapeutics. Margaret Ragni has received research funding to the University from Sanofi, BioMarin, SPARK, and Takeda USA, and serves on advisory boards for Sanofi, BeBio, HEMAB, SPARK, and Takeda USA. Veronica Flood has received research funding from Octapharma. Anthony Navarrete, Pamela Christopherson, and Robert Montgomery have no conflicts of interest to declare related to this research.