
Abstract
Objectives
This study aimed to assess the role of community pharmacists in managing abnormal uterine bleeding (AUB) in women on anticoagulant therapy, particularly in the context of a physician shortage in France, which exacerbates the pharmacist's role. Recognizing these bleedings, which impair the quality of life for women, is an essential role of pharmacists and could be crucial in preventing the risk of discontinuing anticoagulant treatment.
Methods
We conducted an anonymous survey from December 2023 to January 2024 among pharmacists in France to explore their experiences with patients on anticoagulants who presented at pharmacies with questions about AUB.
Results
Of the 115 respondents, only 9 (7.8%) pharmacists had been approached by patients with questions about AUB while on anticoagulants. These pharmacists reported a majority of cases in women of reproductive age, the drug the most frequently cited was rivaroxaban. No significant demographic differences were observed between the pharmacists who had faced these questions and those who had not. Additionally, 99 (86.1%) pharmacists considered that they did not have enough skills to adequately advise female patients about abnormal uterine/genital bleeding under anticoagulant therapy.
Conclusion
Our study showed that community pharmacists are not the primary healthcare contact for patients with AUB under anticoagulant therapy. Despite this, the low frequency of pharmacist-patient interactions regarding AUB suggests potential under-diagnosis and under-communication of adverse effects that negatively impact the quality of life of women on anticoagulants.
Keywords
Introduction
Anticoagulants have significantly evolved over the past 30 years, transitioning from non-specific drugs (heparins and vitamin K antagonists, VKA) to molecules that directly and specifically target coagulation factors (argatroban, fondaparinux, and direct oral anticoagulants, DOAC). For the past decade, DOAC have been widely used due to their ease of use, favorable pharmacological profile, and the advantage of not requiring routine biological monitoring,1,2 especially for the treatment and prevention of venous thromboembolism (VTE) and stroke prevention in non-valvular atrial fibrillation (NVAF). In phase III clinical trials, DOACs demonstrated efficacy comparable to VKAs, with better safety and a lower risk of major bleeding.3,4 However, despite a better safety profile than VKA, DOAC-related bleeding risk is not negligible. The risk of major bleeding using DOAC is estimated at approximately 2% per year,3,4 with a fatal outcome in 8% of cases.5,6 Furthermore, women on anticoagulant therapy appear to be at a higher risk of bleeding compared to men. 7 In women of childbearing age, anticoagulant use can lead to abnormal uterine bleeding (AUB), including heavy menstrual bleeding (HMB), intermenstrual bleeding, or postmenopausal bleeding. 8 These disruptions in a woman's normal menstrual cycle can significantly impair daily activities and quality of life of patient. 9 Addressing this issue is crucial when initiating anticoagulation and during follow-up by both specialists and general practitioners to prevent poor adherence or premature discontinuation of treatment. 8
Over the years, both globally and in France, there has been a growing shortage of physicians, particularly general practitioners and specialists, across much of the country. This has made healthcare access increasingly challenging for the population and has led to the creation of ‘medical deserts’—areas characterized by a low density of healthcare professionals. 10 These medical deserts are mainly in rural or isolated regions but are also becoming more prevalent in urban areas. In this context, community pharmacists play a crucial role as accessible and available healthcare professionals. They are often the first point of contact for many patients and enjoy a high level of trust from the public due to their proximity. However, their involvement in counseling anticoagulated patients remains unclear. The objective of this study was to assess the role of community pharmacists in managing AUB in women on anticoagulant therapy.
Materials and Methods
Study Population
The survey targeted all active community pharmacists in France, including PharmD graduates and sixth-year pharmacy students with a validated community pharmacy internship. Pharmacists from other specialties, such as hospital or industrial pharmacists, were excluded. The survey was conducted anonymously, with no names or email addresses being collected.
Study Period
The survey was conducted from December 4, 2023, to January 14, 2024, and distributed via social media platforms (Facebook, X/Twitter, LinkedIn, BlueSky) and email to reach as many eligible community pharmacists as possible. Additionally, it was shared on the Moodle platform for sixth-year pharmacy students in the 2023–2024 academic year at the School of Pharmacy, Université Paris Cité, Paris, France.
Survey
The questionnaire was developed in the Hematology department at the European Hospital Georges Pompidou, Paris, France. The first version was created using Google Forms and initially tested with a sample of individuals. These individuals were not part of the target population; their feedback was used to ensure the clarity of the questions and expected answers. Their responses were not included in the final data analysis. The survey was subsequently distributed to the study population.
The questionnaire was divided into three sections (See Supplemental Appendix). The first section collected demographic information from respondents, including their status as a community pharmacist, gender, age, pharmacy setting (urban or rural), and department of practice in France. Respondents were also asked to provide information on the average number of daily transactions in their pharmacy and the frequency of vitamin K antagonist (VKA)-related counseling sessions if applicable. The number of transactions per day refers to the average daily volume of patient interactions within the pharmacy. This includes the dispensing of prescription and over-the-counter medications, pharmaceutical counseling, and the sale of health-related and parapharmaceutical products. Finally, pharmacists were asked if they had ever encountered a patient on anticoagulant therapy with questions about AUB while on anticoagulants. If the response was “yes,” the pharmacist proceeded to the second section of the survey. If “no,” they were directed to the third section. The second section focused on pharmacists who had encountered patients with AUB while on anticoagulants, collecting data on patient demographics, the frequency and timing of consultation during anticoagulation follow-up, and the oral and/or parenteral anticoagulants most frequently mentioned. The third section addressed general questions about AUB and anticoagulants. The final question assessed the pharmacists’ confidence (yes or no) in advising these patients based on their knowledge and competencies. The survey was designed to be completed in less than five minutes to maximize response rates.
Statistical Analysis
Qualitative data were presented as numbers (percentages), while quantitative data were expressed as medians [interquartile range, 25th to 75th percentile]. Differences between groups were assessed using the non-parametric Mann-Whitney test. Categorical data were compared using the Chi-square test when expected cell counts were ≥5, and Fisher's exact test was applied when small sample sizes or expected counts <5 were observed . All analyses were 2-sided with a p-value <.05 considered statistically significant. Statistical analyses were performed using GraphPad Prism version 9.1.2.
Results
Study Population
Between December 4, 2023, and January 14, 2024, a total of 115 respondents from 45 departments completed the survey. The most represented departments included Paris with 21 (18.3%) respondents, followed by Cher, Hauts-de-Seine, and Essonne with 5 (4.3%) respondents (Figure 1).
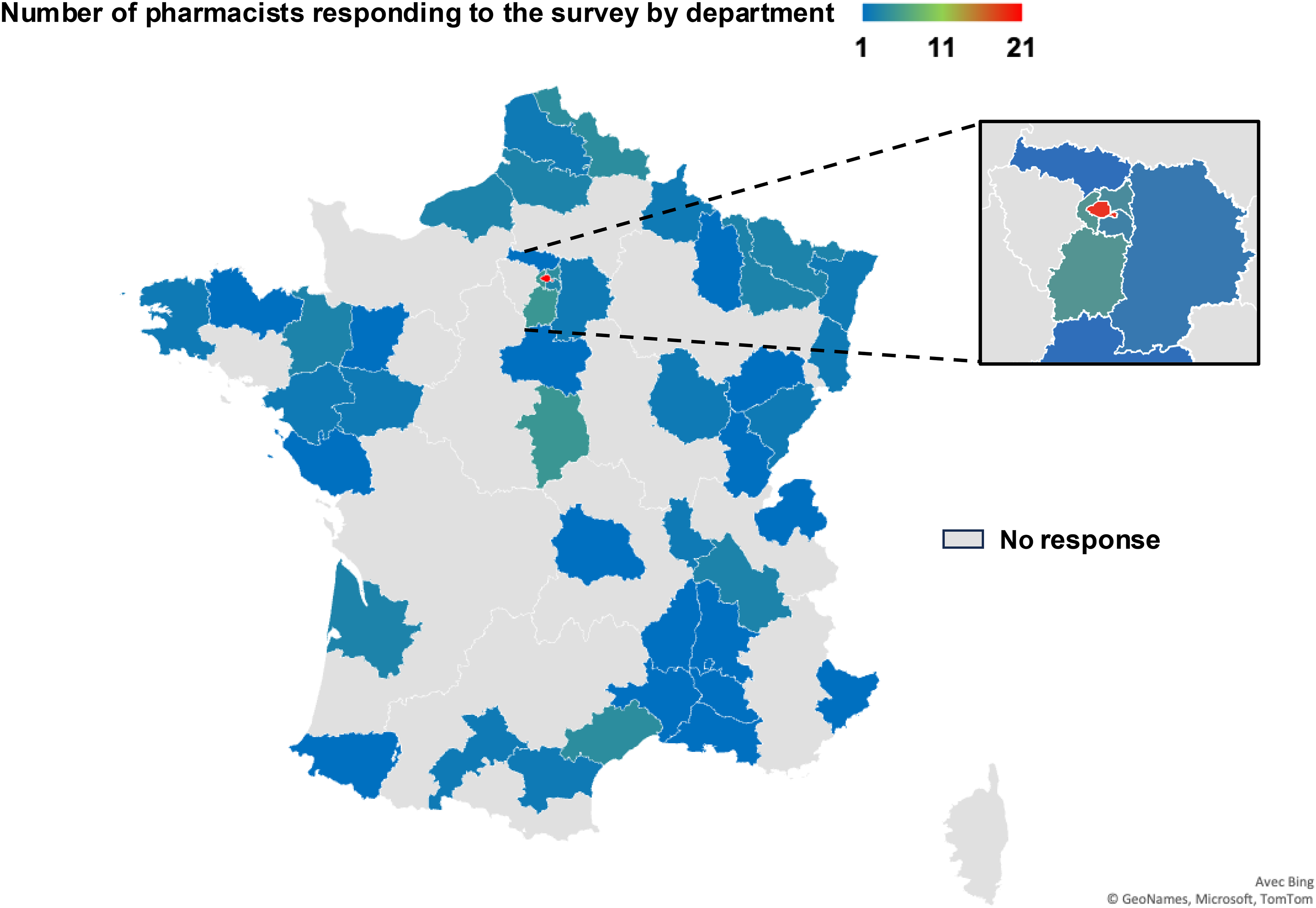
Number of French Pharmacists Responding to the Survey by Department.
The demographic characteristics of the 115 respondents are presented in Table 1. The median age was 30 years (IQR 27.0-38.3), with 71.3% being women. Of the respondents, 90 (78.3%) were licensed pharmacists (PharmD), and 25 (21.7%) were sixth-year pharmacy students with a validated internship. Most respondents (72.2%) worked in urban areas. Over half (55.6%) practiced in small pharmacies, defined as having fewer than 200 daily transactions, while only 16 (14%) worked in pharmacies with over 400 daily transactions. Of the 115 pharmacists, only 21 (18.3%) conducted VKA counseling sessions, with 8 (38.1%) doing so at least once every six months, 3 (14.3%) more than once a month, and 1 (4.8%) more than once a week (Figure 2A and B). No significant differences in demographic data were observed between male and female pharmacists (p > .05).

Proportion of Pharmacists Responding to the Questionnaire Who Conduct Vitamin K Antagonist Counseling Sessions and the Frequency of these Sessions.
Demographic Characteristics of the Pharmacists Responding to the Questionnaire.

abbreviations: IQR, interquartile range; PharmD, doctor of pharmacy; VKA, vitamin K antagonist.
*Average daily volume of patient interactions, including the dispensing of prescription and over-the-counter medications, pharmaceutical counseling, and the sale of health-related and parapharmaceutical products.
AUB Related to Anticoagulant use in Pharmacies
Overall, only 9 (7.8%) of the 115 respondents had encountered patient questions about gynecological bleeding while on anticoagulant therapy (Figure 3A). These pharmacists were predominantly women (55.6%) and worked mainly in urban areas (77.8%, Table 2). Among them, 5 (55.6%) were PharmD, but only 2 (22.2%) conducted VKA counseling sessions. There were no statistically significant demographic differences between these 9 pharmacists and the 106 who had not encountered such questions. The 9 pharmacists described most patients (77.7%) as being of childbearing age, with 33.3% between 25 and 35 years old (Figure 3B). None reported patients under 25 years old. For one-third of the respondents, these situations occurred about once a year (Figure 3C).

Pharmacists and Abnormal Uterine Bleeding Related to Anticoagulants.
Demographic Characteristics of Pharmacists who had Received Questions About Gynecological Bleeding Related to Anticoagulant use.

abbreviations: IQR, interquartile range; PharmD, doctor of pharmacy; VKA, vitamin K antagonist.
Regarding the anticoagulants mentioned, each drug was cited at least twice by the pharmacists, but rivaroxaban was mentioned 7 times, enoxaparin 5 times, and apixaban 4 times (Figure 3D). When asked which medication stood out the most, 44.4% of pharmacists named rivaroxaban (Figure 3E). The majority (77.8%) stated that patient inquiries occurred during a bleeding episode (whether normal or abnormal) rather than at the initial dispensing of anticoagulant therapy.
Pharmacist Responses to Gynecological Bleeding Inquiries
Pharmacists were asked to prioritize several responses from 1 (highest priority) to 7 (lowest priority) when faced with patient inquiries about gynecological bleeding. Of the respondents, only 40 (34.8%) provided answers (Table 3). For the top priority, 16 (40%) pharmacists indicated, “I ask if the bleeding is abnormal,” and 13 (32.5%) chose, “I ask if the bleeding existed before starting anticoagulant therapy.” For the second priority, the responses were 37.5% and 27.5%, respectively. The third priority was “I refer to the general practitioner,” selected by 27.5% of pharmacists. The fourth and fifth priorities involved referring the patient to a prescribing physician or a gynecologist. The option “I suggest a more absorbent hygienic product” was ranked last (seventh priority) by 40% of respondents who answered correctly.
Pharmacists’ Recommendations for Managing Gynecological Bleeding Related to Anticoagulant use by Priority Ranking.
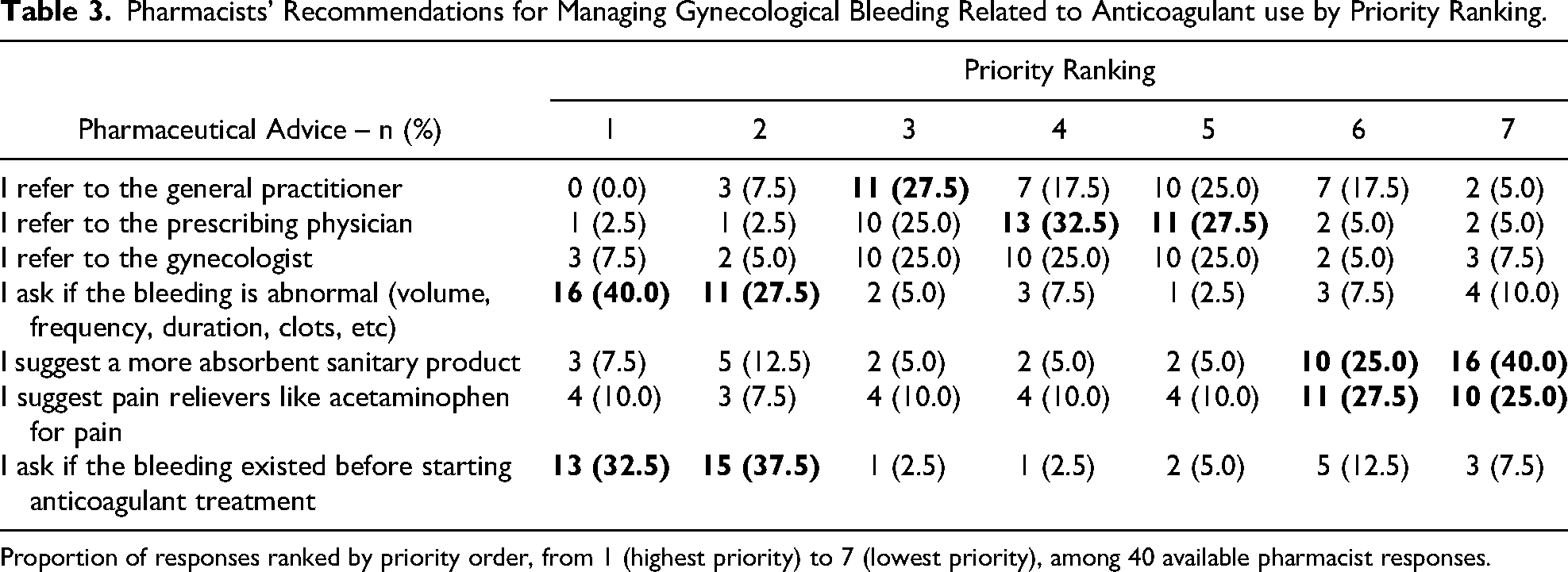
Proportion of responses ranked by priority order, from 1 (highest priority) to 7 (lowest priority), among 40 available pharmacist responses.
Finally, when asked if they felt they had the knowledge and skills to advise patients with AUB on anticoagulants, only 13.9% responded positively, while 86.1% did not (Figure 3F). Among the 13.9% who felt confident, 62.5% were women.
Discussion
The role of community pharmacists in France has evolved, with expanding responsibilities over the years. Recognized as the most accessible healthcare professional, pharmacists played a crucial role during the COVID-19 pandemic, providing information, performing antigen tests, and administering vaccinations. In this survey conducted among pharmacists in France, only 7.8% of respondents had encountered questions from women on anticoagulants about AUB, and for one-third of them, this situation occurred only once per year. These observations suggest that community pharmacists are not the primary healthcare contact for these patients, even though the prevalence of gynecological bleeding among women of childbearing age is estimated to be between 10% and 30%, 11 and only 4 out of 10 women with HMB seek medical help. 12 The lack of recognition, reporting, and diagnosis of HMB not only leads to untreated symptoms but can also result in missed underlying bleeding disorders requiring medical intervention. 12 Gynecological bleeding has multiple etiologies, including polyps, adenomyosis, leiomyomas, malignancy and hyperplasia, coagulopathy, 13 ovulatory disorders, endometrial issues, and iatrogenic causes. 14 However, the medical follow-up of women treated with oral anticoagulants, often managed by specialists such as vascular doctors, cardiologists, pulmonologists, hematologists, internists, or emergency physicians, is challenging. The growing shortage of physicians makes patients less likely to attend follow-up appointments or report issues. 12 According to Paoletti et al, 15 in 2020, only half (47.5%) of general practitioners in France regularly addressed AUB with their female patients on anticoagulants, and only 25% reported a quality of life impact. These findings suggest that the topic is rarely discussed in consultations and even less so in pharmacies, despite its potential impact on women's quality of life.
A recent prospective Franco-Dutch study 9 observed that two-thirds of women who started anticoagulant therapy for VTE experienced gynecological bleeding, which had a significant negative impact on quality of life. Such bleeding can adversely affect the patient's physical, social, and emotional well-being and may lead to non-adherence or premature discontinuation of anticoagulant therapy, increasing the risk of VTE and recurrences. 8 Bryk et al found that women on rivaroxaban, compared to those on VKAs, had a higher risk of AUB (OR = 3.2; 95% CI, 1.4-8.2), treatment interruption (OR = 3.2; 95% CI, 1.1-11.6), and VTE recurrence (OR = 5.3; 95% CI, 1.1-33.3). 16 In our study, 86.1% of pharmacists reported lacking sufficient knowledge and skills to advise patients with gynecological bleeding while on anticoagulants. This highlights the limited experience of community pharmacists regarding oral anticoagulant-related AUB. Many prefer to refer patients to a physician, acknowledging gaps in their expertise. Interestingly, 62.5% of pharmacists who felt confident in their knowledge were women, suggesting that female pharmacists may feel more capable of discussing gynecological issues, possibly due to personal experiences with menstruation. In the present study, only 18.3% of pharmacists conducted VKA counseling sessions, typically once every six months. The low participation rate may be attributed to the modest remuneration provided by French Health Insurance for these sessions, which does not adequately compensate for the time and effort involved.17,18 Addressing this issue may require developing new tools, such as training sessions or e-learning modules, to enhance pharmacists’ knowledge. It is also crucial to improve the initial education in hemostasis for pharmacy students, especially concerning anticoagulant-induced bleeding. Recent findings from our team indicate that French pharmacy students have a poor understanding of oral anticoagulants despite dedicated courses in their curriculum. 19
In 2022, a French national diagnostic and care protocol was established 20 to improve the management of AUB in young women with congenital or acquired bleeding disorders. However, the protocol assigns only a minor role to community pharmacists, who are expected to refer patients to their general practitioners. Even when referred, the management of these women on anticoagulants remains unclear. First-line treatments for HMB, such as combined oral contraceptives, are contraindicated in women with a history of VTE. Tranexamic acid is often mentioned for women with hereditary bleeding disorders, but there is no consensus on its use in this context. 21
The Dutch MEDEA study, a randomized, open-label trial 22 evaluated management strategies for women with HMB associated with oral factor Xa inhibitors. Despite a small sample size, the study suggested that adding tranexamic acid to oral factor Xa inhibitors therapy or switching to dabigatran were safe and effective strategies to reduce blood loss.
Our survey found that rivaroxaban was the most frequently implicated drug, though the survey's design did not allow for precise conclusions about the incidence of bleeding by anticoagulant. This is consistent with previous studies,16,23 which found that DOACs, particularly rivaroxaban, are associated with a higher risk of AUB than warfarin. The post hoc analysis of the EINSTEIN-DVT and EINSTEIN-PE trials, 24 found a 10.7% incidence of abnormal uterine bleeding in women treated with rivaroxaban, with a higher risk than warfarin (HR = 2.13; 95% CI, 1.57-2.89). In contrast, the AMPLIFY trial's post hoc analysis 25 reported 1.4% of women on apixaban experiencing menorrhagia compared to 1.1% on VKAs. Less than 0.1% of women on apixaban experienced major gynecological bleeding, while 2.5% experienced clinically relevant non-major bleeding, compared to 2.1% on warfarin. 25 Among pharmacists who had encountered questions about AUB, none reported such inquiries at the initial dispensing of anticoagulants. This is likely because VTE treatments are typically initiated in emergency departments or by vascular specialists immediately following imaging confirmation. Given the apparent underreporting and potential stigma surrounding AUB, community pharmacists could play a proactive role in identifying women at risk when dispensing oral anticoagulants. The prognostic score developed by Sarlon-Bartoli et al could help pharmacists identify at-risk patients based on age <50 years, weight >70 kg, and prescription of an oral FXa inhibitor. 26
We acknowledge that the small number of respondents is a limitation of the study. The low response rate may be due to the nonmandatory and nonrewarding nature of the survey. Additionally, the survey could not be disseminated by the National Council of the Order of Pharmacists due to a high volume of similar requests, which limited its distribution scope. We acknowledge that the survey was distributed over a relatively short period of approximately one month, which may have limited the number of responses. However, the survey format was intentionally kept short to retain respondents, with a completion time of under 5 min, as community pharmacists are currently overwhelmed with numerous responsibilities. 17 We also acknowledge that although we reported the total number of daily transactions per pharmacy as a proxy indicator of the pharmacy's activity level, we were not able to evaluate their specific experience with anticoagulants based on the proportion of anticoagulant-related transactions per day.
Conclusion
Our study showed that community pharmacists are not the primary healthcare contact for patients with AUB under anticoagulant therapy. Despite this, the low frequency of pharmacist-patient interactions regarding AUB suggests potential under-diagnosis and under-communication of adverse effects that negatively impact the quality of life of women on anticoagulants. Strengthening pharmacists’ training in this area is essential to improve the identification, monitoring, and management of patients with AUB, thereby optimizing their quality of life and minimizing the risks associated with anticoagulant misuse
Supplemental Material
sj-docx-1-cat-10.1177_10760296251350078 - Supplemental material for Pharmacists’ Knowledge of Abnormal Uterine Bleeding in Women on Anticoagulant Therapy: A French Survey
Supplemental material, sj-docx-1-cat-10.1177_10760296251350078 for Pharmacists’ Knowledge of Abnormal Uterine Bleeding in Women on Anticoagulant Therapy: A French Survey by Sibylle Frerebeau, Benjamin Planquette, Gabrielle Sarlon and Nicolas Gendron in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgements
We would like to thank all the pharmacists who responded to this survey.
Authors Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.