
Abstract
Acute ischemic stroke (AIS) is a leading cause of mortality and disability worldwide. Recombinant human prourokinase (rhPro-UK) has emerged as a promising thrombolytic agent amid the global shortage of thrombolytics. We assessed the safety and efficacy of rhPro-UK in AIS patients within 4.5 h of stroke onset through a systematic review and meta-analysis of RCTs from PubMed, Web of Science, Scopus, and Cochrane until January 2024. Data were pooled using risk ratio (RR) or mean difference (MD) with 95% confidence intervals (CI) in R version 4.3. PROSPERO ID: CRD42025638980. Three RCTs (2289 patients) were included. rhPro-UK showed comparable efficacy to recombinant tissue plasminogen activator (r-tPA) in excellent neurological recovery (mRS 0–1: RR 1.04, 95% CI [0.98, 1.10], P = 0.19) and functional independence (mRS 0–2: RR 1.00, 95% CI [0.96, 1.05], P = 0.87). However, rhPro-UK significantly reduced NIHSS scores at 24 h (MD −0.43, 95% CI [−0.85, −0.02], P = 0.04) and seven days (MD −0.85, 95% CI [−1.39, −0.30], P < 0.01), and decreased systemic bleeding (RR 0.60, 95% CI [0.49, 0.75], P < 0.01). No significant differences were observed in 90-day mortality (RR 1.13, 95% CI [0.62, 2.05], P = 0.69) or intracerebral hemorrhage (RR 0.83, 95% CI [0.61, 1.13], P = 0.23). rhPro-UK demonstrates comparable efficacy to r-tPA with reduced NIHSS scores and systemic bleeding, supporting its role as a cost-effective and safer alternative for AIS treatment within 4.5 h. Further investigation in stroke management protocols is warranted.
Introduction
Acute ischemic stroke (AIS) is a medical emergency and a major cause of mortality and disability worldwide. Stroke is the second leading cause of death, and the third leading cause of disability and mortality combined, with the greatest disease burden in low-income countries. 1 Ischemic strokes account for around 80% of total stroke cases with behavioral risk factors such as smoking and a diet high in sodium, along with metabolic risk factors like high body mass index, high blood pressure, high LDL cholesterol, diabetes mellitus, and kidney dysfunction, are associated with ischemic stroke death.2,3
Treatment of stroke has evolved from solely preventive strategies, like controlling risk factors through lifestyle modifications, to surgical interventions on the carotid arteries. The greatest breakthrough came when recombinant tissue plasminogen activator (rtPA) was introduced by Désiré Collen in the 1980s. In 1996, alteplase became the first FDA-approved thrombolytic therapy for AIS. The early 2000s saw advancements in minimally invasive procedures to remove clots via endovascular thrombectomy.4,5 The current standard treatment for AIS is intravenous thrombolysis within the first 4.5 h of symptom onset for eligible patients without absolute contraindications, to avoid the transformation of ischemic to hemorrhagic type. Although alteplase has effectively improved neurological outcomes, its high cost and narrow therapeutic window, with a significant risk of intracerebral hemorrhage, have spurred the search for newer thrombolytic alternatives.6,7
Recombinant human prourokinase (rhPro-UK) is a selective glycosylated single-chain zymogenic plasminogen activator that converts plasminogen to plasmin, breaking down clots mainly at the thrombus site, with lesser effects in plasma, resulting in a lower risk of systemic bleeding than alteplase. 8 The potential of prourokinase as a treatment for ischemic stroke was first highlighted in 1999. The PROACT-II trial compared prourokinase plus intravenous heparin to intravenous heparin alone within 6 h of stroke onset in patients with proximal middle cerebral artery occlusion. The prourokinase group had more favorable neurological outcomes at 90 days. However, the efficacy and use of rhPro-UK in ischemic stroke are not yet well-established. 9
More recent studies on rhPro-UK in ischemic stroke have been conducted in the last couple of years. In 2022 and 2023, Song et al published results of phase IIa and a phase III randomized control trial (RCT), respectively. In phase IIa, they found both low- and high-dose rhPro-UK within 4.5 h to be safe, with efficacy comparable to rtPA 10 while in phase III, intravenous rhPro-UK was not inferior to alteplase in AIS patients and had a similar symptomatic intracerebral hemorrhage (ICH) risk but a lower risk of systemic bleeding. 11 The most recent study, the PROST-2 trial published in 2025, emphasized the safety and excellent efficacy of intravenous prourokinase in AIS, supporting its use as a viable alternative to alteplase. 12
Despite the progress in understanding and treating AIS, there remains a significant gap in knowledge regarding the comparative efficacy and safety of rhPro-UK and the current standard treatment. While recent studies have shown promising results for rhPro-UK, a comprehensive meta-analysis is needed to integrate these findings and provide clear evidence on its potential as a viable alternative. This meta-analysis aims to address this gap, offering a thorough evaluation of neurological outcomes and potential adverse events of rhPro-UK within the critical 4.5-h window in AIS.
Methodology
Protocol Registration
Our review was registered and published in PROSPERO with ID: CRD42025638980. We conducted a systematic review and meta-analysis sincerely guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 13 and the Cochrane Handbook of Systematic Reviews and Meta-Analysis. 14
Data Sources & Search Strategy
Web of Science, SCOPUS, PubMed (MEDLINE), and Cochrane Central Register of Controlled Trials (CENTRAL) were systematically searched from inception until JAN 10th, 2025. No search filters were used. The detailed search approach and results are outlined in (Table S1).
Eligibility Criteria
We included RCTs with the following PICO criteria:
Population: adult patients with AIS presenting at the time window (presentation within 4.5 after stroke onset) Intervention: rhPro-UK (at a 15-mg bolus, followed by 20 mg continuous infusion (35 mg)). Control: r-tPA (as 0.9 mg/kg; maximum dose 90 mg). Outcomes: our primary outcome was the modified rankin score (mRS) at 90 Days. Secondary outcomes were national institutes of health stroke scale (NIHSS), systemic bleeding, any intracerebral hemorrhage, symptomatic intracerebral hemorrhage (ECASS III criteria), all-cause mortality, ischemic stroke recurrence within 7 days and any serious adverse events (SAE).
The exclusion criteria for the papers were as follows: The following categories of studies are not regarded as unique: 1) book chapters; (2) non-human and in vitro experiments; (3) studies with overlapping or duplicate datasets; (4) book chapters, reviews, comments, letters to the editor, and guidelines; and 5) studies not published in English.
Study Selection
Search results from all the databases were imported to Covidence.org, and duplicates were removed automatically. Four authors (A.A.A., S.S.A., L.S., and H.A.A.) screened the remaining records independently, and a fifth author (A.A.I) resolved any conflict. The screening was done in two steps: (i) title and abstract screening to determine the study's relevance for this meta-analysis, and (ii) full-text screening according to the inclusion criteria for the final eligibility for qualitative and quantitative analysis.
Data Extraction
Four review authors collected data independently (M.R., S.M.A., Y.F.A., and Z.T.M.) and extracted it into a uniform data extraction Excel sheet. The extracted data included characteristics of the included studies, including first author name, year of publication, country, study design, blinding, total participants, intervention detail, control details, inclusion criteria, primary outcome, follow-up duration; participants’ baseline characteristics, including the number of participants, mean age, gender, time from onset to intravenous thrombolysis, NIHSS score, and comorbidities; efficacy and safety outcome measures across as previously described. Any disagreement was resolved by consensus.
Risk of Bias and Certainty of Evidence
Two reviewers (A.A.I., and A.O.A.) independently assessed the quality of the included studies using the Cochrane ROB2 tool. 15 The domains that were evaluated included the risk of bias resulting from the randomization process, the risk of bias due to deviation from the intended intervention, the risk of bias due to missing outcome data, the risk of bias in the measuring of outcomes, and the risk of bias in selecting the reported results. To appraise the quality of evidence, we utilized the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) guidelines.16,17 The evaluation was carried out for each outcome, and the decisions were justified and documented. Any discrepancies were settled through discussion.
Statistical Analysis
The study employed R version 4.3, utilizing the meta, metafor, and dmetar packages for statistical analysis. The analysis combined results from multiple studies using either risk ratios (for dichotomous outcomes) or mean differences (for continuous outcomes), both with 95% confidence intervals. A random-effects model was applied when significant heterogeneity (I2 > 50%) was detected using the Chi-square and I-square tests; otherwise, a common-effect model was used. Heterogeneity was interpreted according to the Cochrane Handbook (chapter nine), 14 with an I2 value of 0%–40% indicating low heterogeneity, 30%–60% signifying moderate heterogeneity, 50%–90% may represent substantial heterogeneity, and 75%–100% signifying considerable heterogeneity A Chi-square test p-value below 0.1 was considered statistically significant for heterogeneity.
Results
Search Results and Study Selection
Database searches yielded 786 articles from Cochrane Central, PubMed, Web of Science, and Scopus. Covidence Online eliminated 115 duplicates, and 669 articles were screened. 655 articles were eliminated by screening the title and abstract, yielding 14 articles assessed for eligibility, of which we identified three eligible RCTs. A PRISMA flow chart depicts the database search and research selection procedure (Figure 1).

PRISMA flow chart of the screening process.
Characteristics of Included Studies
Three RCTs with 2289 participants were included in the final analysis: 1141 in the rhPro group and 1148 in the r-tPA group. RCTs varied in their sample size, ranging from 74 to 1552 patients. They compared intravenous rhPro-UK as a 15-mg bolus administered within 3 min, followed by 20 mg continuous infusion within 30 min with intravenous r-tPA as 0.9 mg/kg; maximum dose 90 mg; 10% bolus followed by the remainder as infusion over 60 min. The follow-up period in the included studies was all the same at 90 days after randomization. A summary of the included studies is shown in (Table 1), and the baseline characteristics of their populations are shown in (Table 2).
Summary Characteristics of the Included RCTs.

Abbreviations: NIHSS: National Institutes of Health Stroke Scale, AIS: arterial ischemic stroke.
Baseline Characteristics of the Participants.

Abbreviations: NIHSS: National Institutes of Health Stroke Scale, SD: standard deviation, AF: atrial fibrillation, HTN: hypertension, DM: diabetes mellitus, TIA: transient ischemic attack.
Risk of Bias and Certainty of Evidence
Each study's risk of bias assessment is detailed (Figure 2, Tables S2-S4). All the studies included demonstrated a low risk of bias across all assessed domains except Song et al 2022 raised some concerns in domain 4 due to unblinding of outcome assessors. Also, the certainty of evidence is demonstrated in a GRADE evidence profile (Table 3).
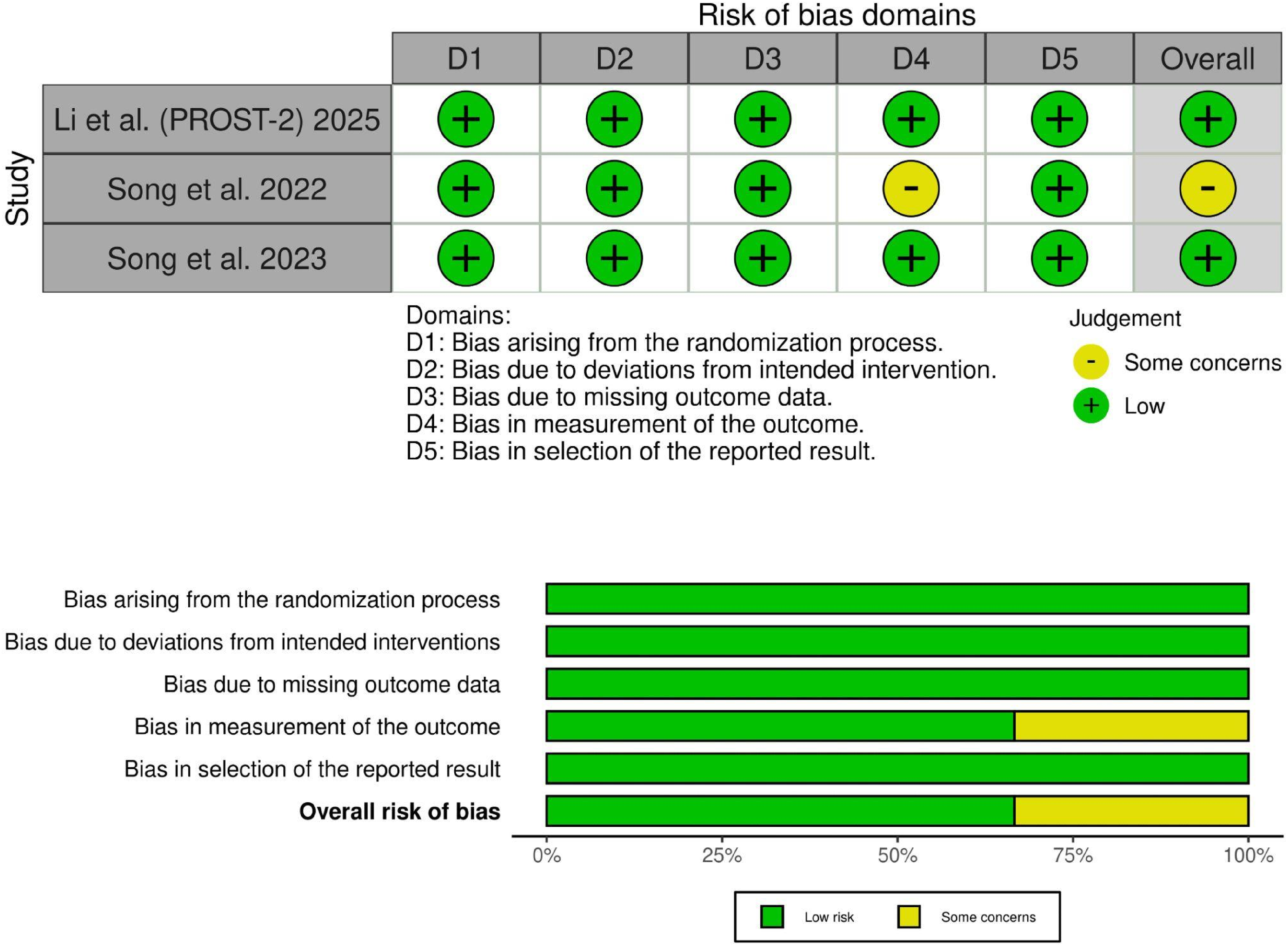
Quality assessment of risk of bias in the included trials. The upper panel presents a schematic representation of risks (low = red, unclear = yellow, and high = red) for specific types of biases of each study in the review. The lower panel presents risks (low = red, unclear = yellow, and high = red) for the subtypes of biases of the combination of studies included in this review.
GRADE Evidence Profile.

CI: confidence interval; MD: mean difference; RR: risk ratio
Explanations
a. A wide confidence interval that does not exclude the appreciable harm or benefit.
b. A wide confidence interval, with a low number of events.
Primary Outcome: Modified Rankin Score (mRS) at 90 Days
There was no significant difference between prourokinase and the r-tPA group in excellent neurological recovery (mRS 0-1) (RR: 1.04 with 95% CI [0.98, 1.10], P = 0.19), functional independence (mRS 0-2) (RR: 1.00 with 95% CI [0.96, 1.05], P = 0.87), and independent ambulation (mRS 0-3) (RR: 1.00 with 95% CI [0.97, 1.03], P = 1.00) (Figure 3-A).

Forest plot of the primary efficacy outcome after 90 days: A: Modified Rankin Score (mRS); B: National Institutes of Health Stroke Scale (NIHSS). MD: mean difference, RR: risk ratio, CI: confidence interval.
Pooled studies were homogenous in excellent neurological recovery (mRS 0-1) (I2= 0%, P = 0.88), functional independence (mRS 0-2) (I2= 0%, P = 0.89), and independence ambulation (mRS 0-3) (I2= 0%, P = 0.50).
Secondary Outcomes
National Institutes of Health Stroke Scale (NIHSS)
Prourokinase was significantly associated with reduced NIHSS score compared to r-tPA group either at 24 h (MD: −0.43 with 95% CI [−0.85, −0.02], P = 0.04) or at seven days (MD: −0.85 with 95% CI [−1.39, −0.30], P < 0.01) (Figure 3-B).
Pooled studies were homogenous in NIHSS score either at 24 h (I2= 0%, P = 0.43) or at seven days (I2 = 0%, P = 0.59).
Safety Outcomes
Prourokinase was significantly associated with decreased incidence of systemic bleeding compared to r-tPA (RR: 0.60 with 95% CI [0.49, 0.75], P < 0.01) (Figure 5). However, there was no significant difference between prourokinase and the r-tPA group in poor neurological recovery (mRS 4–6) (RR: 1.00 with 95% CI [0.80, 1.25], P = 1.00), all-cause mortality within 7 days (RR: 0.92 with 95% CI [0.16, 5.21], P = 0.92), all-cause mortality within 90 days (RR: 1.13 with 95% CI [0.62, 2.05], P = 0.69), any SAE (RR: 0.92 with 95% CI [0.75, 1.13], P = 0.41) (Figure 4), any intracerebral hemorrhage (RR: 0.83 with 95% CI [0.61, 1.13], P = 0.23), symptomatic intracerebral hemorrhage (ECASS III criteria) (RR: 0.52 with 95% CI [0.23, 1.19], P = 0.12), and ischemic stroke recurrence within 7 days (RR: 0.85 with 95% CI [0.16, 4.54], P = 0.85) (Figure 5).

Forest plot of primary safety outcomes (poor neurological recovery, all-cause mortality, and any severe adverse events), RR: risk ratio, CI: confidence interval.

Forest plot of secondary safety outcomes (intracerebral hemorrhage, systemic bleeding, and ischemic stroke recurrence), RR: risk ratio, CI: confidence interval.
Pooled studies were homogenous in poor neurological recovery (mRS 4–6) (I2= 0%, P = 0.51), all-cause mortality within 90 days (I2= 24%, P = 0.27), any SAE (I2= 0%, P = 0.38), any intracerebral hemorrhage (I2= 0%, P = 0.67), symptomatic intracerebral hemorrhage (ECASS III criteria) (I2= 0%, P = 0.48), any systemic bleeding (I2= 0%, P = 0.75), and ischemic stroke recurrence within 7 days (I2= 0%, P = 0.74).
However, pooled studies were heterogeneous in all-cause mortality within 7 days (I2= 80%, P = 0.03). Sensitivity analysis was not applicable.
Discussion
In this systematic review and meta-analysis, we incorporated evidence from the most recent three multicentered RCTs with total of 2289 participants with AIS within 4.5 h of stroke onset to compare the novel thrombolytic agent (intravenous recombinant human prourokinase) as a 15-mg bolus followed by 20 mg continuous infusion with intravenous r-tPA as 0.9 mg/kg; maximum dose 90 mg. The analysis showed that there was no significant difference between prourokinase and the r-tPA group in neurological recovery on mRS at 90 days follow-up period. Moreover, rhPro-UK was significantly associated with a reduced NIHSS score either at 24 h or at seven days. The incidence of systemic bleeding significantly reduced in the prourokinase group. However, no difference was detected in all-cause mortality, any SAE
Alteplase has been the standard treatment for AIS; however, alternative thrombolytic agents have been investigated due to the global shortage of thrombolytics, the high bleeding risk of alteplase stemming from its narrow therapeutic window, and its high cost, which limits its use in some developing countries. 18 Investigated thrombolytic alternatives include tenecteplase (TNK), non-immunogenic staphylokinase, reteplase, and recently, rhPro-UK. In addition to new drugs, there are new treatment strategies aimed at reducing the risk of vessel reocclusion and considering the use of intraarterial thrombolysis after mechanical thrombectomy. 19
Previously, stroke research focused on large vessel occlusion and recanalization. Recently, treatment strategies have targeted cerebral reperfusion and the cerebral circulation microthrombi that remain before and after endovascular thrombectomy.20,21 The development of stroke and reperfusion therapeutic options has been heavily highlighted lately. This can be attributed to the evolution of telemedicine, which has enhanced the identification of cases indicated for thrombolysis. Additionally, an increased number of mobile stroke units have boosted early intervention in AIS and shortened the time between symptom onset and medical care.22,23
Many recent trials on tenecteplase and reteplase suggested that both are non-inferior to alteplase regarding functional outcomes at 90 days.24,25 Tenecteplase, a novel thrombolytic drug modified from alteplase, has a longer half-life, allowing for ease of administration as a single IV bolus and a faster onset of action compared to alteplase. It has been approved in Europe, China, and Argentina. Multiple new meta-analyses of RCTs suggested that tenecteplase is as effective and safe as alteplase in AIS and might be more beneficial.26–28 Reteplase is another promising thrombolytic for AIS, associated with excellent neurological outcomes compared to alteplase. 25 Non-immunogenic recombinant staphylokinase, another new thrombolytic option, was compared to alteplase in AIS in the FRIDA trial conducted in Russia which provides evidence for the non-inferiority of non-immunogenic staphylokinase to alteplase. 29 rhPro-UK was more famous for being a thrombolytic drug for acute myocardial infarction. Studies showed that prourokinase is a safe and effective option in acute STEMI, improving reperfusion and reducing infarction size. 30 The first trial to use rhPro-UK in AIS was the PROACT randomized controlled trial conducted between February 1996 and August 1998. In this trial, intra-arterial prourokinase plus IV heparin was compared to IV heparin alone in patients with middle cerebral artery occlusion within 6 h of stroke onset. The recanalization rate was 57.7% in the prourokinase group and 15.4% in the control group, but the frequency of early symptomatic cerebral hemorrhage was significantly increased in the prourokinase group while our meta showed no difference regarding the symptomatic intracerebral hemorrhage. This conflict may be attributed to the use of heparin besides prourokinase in PROACT trial. 31 Moreover, Furlan et al concluded that the improvement in neurological outcomes with prourokinase is significant over its cerebral bleeding risk. 9 Despite these results, prourokinase was not established in AIS management.
Recently, more trials have been conducted to reinvestigate the safety and efficacy of this myocardial infarction-approved drug in the treatment of AIS. In 2022, Song et al published the results of their phase IIa RCT. They found both low and high doses of intravenous rhPro-UK to be safe and as effective as rtPA, this trial results were similar to our results as it showed no significant difference in the rate of favorable neurological outcome (mRS score 0–1) also, they found no difference in mortality or intracerebral hemorrhage or any SAE between the two groups but, it didn't detect a significant difference in NIHSS score or in systemic bleeding, unlike our meta that showed both to be reduced with the prourokinase. 10 This trial was limited by its small sample size but provided crucial data, which helped in conducting phase III multi-center clinical trial to further evaluate the drug's safety and efficacy and prove its non-inferiority to alteplase.
The PROST trial, conducted across 35 hospitals in China, included 663 ischemic stroke patients. The study demonstrated that 35 mg prourokinase was non-inferior to alteplase, with both treatments yielding similar rates of favorable outcomes (mRS score of 0–1 at 90 days). There was no significant difference in the incidence of intracerebral hemorrhage or any SAE between the two treatments. Notably, rhPro-UK exhibited a lower risk of systemic bleeding. The results of our meta-analysis support most of the findings of this trial. 11 The lower bleeding rate could be due to prourokinase acting mainly at the thrombus site and not forming protease inhibitor complexes in the plasma. 8
However, the predefined margin of non-inferiority was based on a 10% difference in the PROST trial, which may be considered too generous. The PROST-2 phase III RCT further expanded the evidence of prourokinase's non-inferiority. The study enrolled 1552 patients in 61 hospitals in China and suggested that prourokinase is non-inferior to alteplase, with an absolute margin of 1.3%, consistent with MCID for functional independence. It also showed a comparable risk of sICH defined by ECASS III criteria and major or non-major bleeding and no difference in all-cause mortality or SAEs within 90 days12–32 which is consistent with our meta-analysis results. The rate of events for these safety outcomes was generally low in both groups, so the possibility of chance cannot be excluded. Unlike alteplase, Prourokinase can save both time and money as it doesn't need adjustment of the dose according to body weight which can save time and it is roughly half the cost of alteplase and two-thirds the cost of tenecteplase, making it a cost-effective option for stroke cases given its favorable safety and non-inferior efficacy compared to the standard treatment. 12
Implication for Future Research
The findings of this meta-analysis highlight the non-inferiority of rhPro-UK compared to rtPA in the treatment of AIS within the 4.5-h window. Despite these promising results, further research is warranted to confirm the generalizability of rhPro-UK's efficacy and safety across diverse populations and different healthcare settings. Future studies should focus on larger, multicenter trials with varied demographics to address the current limitation of studies predominantly conducted in Chinese populations. Additionally, the impact of rhPro-UK on long-term functional outcomes, healthcare costs, and quality of life should be investigated. Exploring the potential benefits of combining rhPro-UK with other therapeutic strategies, such as endovascular thrombectomy, may also provide valuable insights. Finally, given the promising results observed, it is a logical step to further investigate the efficacy and safety of lower-dose rhPro-UK in a large-scale, well-powered RCTs. Addressing these research gaps will contribute to a more comprehensive understanding of rhPro-UK's role in AIS management and its potential as a cost-effective alternative to alteplase.
Strengths and Limitations
This study is the first meta-analysis to provide collective evidence for prourokinase use in AIS and includes 3 high qualities recent RCTs with large sample size and minimal heterogeneity. To assess the certainty of evidence, we employed the GRADE tool which provides a systematic and transparent examination method in systematic reviews and meta-analyses.16,17
This study has multiple limitations. First, all patients were Chinese, so the results may not be generalized in different populations. Second, the open label design of the included studies may have introduced biases to the results. Third, in the largest trial (PROST-2) women were underrepresented and stroke mimic rate data was not collected, and they excluded patients eligible for endovascular thrombectomy so genializing the finding of this study could be questioned.
Conclusion
This meta-analysis provides evidence supporting the non-inferiority of rhPro-UK compared to rtPA in the treatment of AIS within the critical 4.5-h window. The results demonstrate that rhPro-UK offers similar efficacy in neurological recovery on mRS, with the added benefit of a lower NIHSS and a lower incidence of systemic bleeding without affecting the overall mortality. These findings underscore the potential of rhPro-UK as a cost-effective and safer alternative to rtPA. Further large-scale, multi-center trials involving diverse populations are essential to validate these results and explore the long-term benefits and adverse effects of rhPro-UK in AIS patients.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251328025 - Supplemental material for Efficacy and Safety of Recombinant Human Prourokinase in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cat-10.1177_10760296251328025 for Efficacy and Safety of Recombinant Human Prourokinase in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis by Abdulaziz A. Alzahrani, Ahmed A. Maiz, Ahmed A. Ibrahim, Mohamed Rifai, Suhaiyh Sanad Alotibi, Leena Salem, Hadeel A. Alzabidi, Sarah Mansour Alshehri, Yara Fahad Almazyad, Zeyad T. Mansour and Abubaker Osman Ahmed in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgment
None.
Author Contributions
A.A.I. conceived the idea. A.O.A. and A.A.I. designed the research workflow. M.R. and A.A.I. searched the databases. A.A.A., S.S.A., L.S., and H.A.A. screened the retrieved records. M.R., S.M.A., Y.F.A., and Z.T.M. extracted relevant data, assessed the quality of evidence, and A.A.I. resolved the conflicts. A.A.I performed the analysis. A.AM
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.