
Abstract
Introduction
Venous thromboembolism (VTE) is a medical condition in which a blood clot forms in a vein. A VTE event can be classified as deep vein thrombosis (DVT) or pulmonary embolism (PE), depending on the location of the clot. DVT ranks as one of the top leading causes of death from cardiovascular disease, following heart attacks and stroke. 1 Even in cases in which pulmonary embolism does not occur, recurrent thrombosis and the resulting “post-thrombotic syndrome” contribute significantly to morbidity.1,2
Furthermore, DVT has several risk factors that can increase risk and worsen outcomes; these factors are classified into two primary categories: acquired and inherited. Acquired risk factors include conditions or circumstances that can develop during an individual's lifetime, while inherited risk factors are associated with genetic predisposition. Moreover, acquired risk factors for DVT consist of various factors, including prolonged immobility, hospitalization, major trauma, cancer, hormonal therapies, pregnancy, obesity, smoking, and advanced age. Contrariwise, inherited risk factors involve a personal or family history of DVT or pulmonary embolism as well as genetic clotting disorders.2,3
DVT is the formation of a blood clot in the deep veins, typically in the lower extremities; however, it can also occur in the upper extremities as well as the mesenteric and cerebral veins.2–4 Based on the location and extent of the clot, DVT can be further classified into isolated distal DVT (iDDVT), isolated proximal DVT (iPDVT), or mixed DVT. iDDVT is confined to the veins below the knee, typically affecting the calf veins, without extending into the popliteal or more proximal vein. Meanwhile, iPDVT involves the veins above the knee, including the popliteal, femoral, and iliac veins, without extending into the calf veins. Mixed DVT refers to incidents in which both distal and proximal veins are involved: the clot extends from the calf veins into the popliteal, femoral, or iliac veins. 5 Understanding this classification system is crucial for determining appropriate treatment approaches and assessing the risk of complications. Complications of lower extremity DVT include PE, post-thrombotic syndrome (PTS), recurrent DVT, or chronic thromboembolic pulmonary hypertension (CTEPH).2,3 The aim of this study was to explore the baseline characteristics and clinical outcomes of patients with different types of DVT, namely iDDVT, iPDVT, and mixed DVT.
Methods
Study Design, Setting, and Ethical Approval
This was a retrospective single-center study of patients who experienced a new DVT event between January 2015 and September 2022 at King Abdulaziz Medical City in Riyadh. Patients aged 18 or older who experienced their first DVT event and received an anticoagulant for management were included in this study. Patients who were diagnosed with thrombus in other locations, patients with cancer, those who were lost to follow-up, and those receiving an anticoagulant for another indication or a prophylactic dose of anticoagulant were excluded from this study. This study obtained Institutional Review Board approval from the King Abdullah International Medical Research Center (SP22R/234/10).
Data Collection
The following data were collected: patient demographics and data regarding indexed DVT events, including the location of the DVT, year of diagnosis, etiology such as leg injury (any trauma or physical harm to the lower limb that results in structural damage, including fractures, contusions, sprains, or lacerations), pregnancy, estrogen use, and risk factors such as surgical history, oral contraceptive use, immobility, and obesity. Additional information was collected regarding comorbidities, such as hypertension, diabetes, stroke, transient ischemic attack (TIA), chronic kidney disease (CKD), valvular heart disease, and atrial fibrillation. Additionally, we collected laboratory data including hemoglobin (Hgb), serum creatinine, and the estimated glomerular filtration rate (eGFR). Information on anticoagulant agents and patient outcomes during hospitalization and over a 12-month follow-up period was collected, including recurrent DVT events, major bleeding (MB), rehospitalization, mortality, and bleeding events.
Study Outcomes and Statistical Analysis
The outcomes of this study include an evaluation of patient characteristics for individuals with different types of DVT (iPDVT, iDDVT, and mixed DVT), as well as an assessment of the incidence of recurrent DVT, MB, VTE-related rehospitalization, and DVT-related inpatient mortality across different types of DVT. Parametric continuous variables are presented as means with standard deviation (SD) values, while categorical variables are presented as frequencies with percentages. One-way ANOVA test was used to compare the continuous variables of baseline characteristics of the three study groups, while chi-square test was used to compare the categorical variables of baseline characteristics. A chi-square test was used for the comparison of patient characteristics and the study outcomes among different types of DVT. For all analyses, a P-value of <.05 was utilized to determine significance. The analysis was conducted using Stata version 16.1 (Stata Corp, College Station, TX).
Results
Patient Demographics and Medical History
A total of 1767 patients with a DVT event documented on their electronic medical record were assessed for their eligibility for inclusion in this study. This study ultimately included a subset of 493 patients; the remaining patients were excluded due to the criteria illustrated in Figure 1.

Patients’ inclusion and exclusion flow diagram. Abbreviations: VTE, venous thromboembolism; DVT, deep vein thrombosis; PE, pulmonary embolism; US, ultrasound.
Of the 493 patients with DVT, 273 (55.4%) had iPDVT, 25 (5.1%) had iDDVT, and 195 (39.6%) had mixed DVT. Among all patients, the mean age was 56.9 ± 21.7 years, 307 (62.3%) were female, and 356 (72.2%) had a provoked DVT event. Among those who had provoked DVT, the VTE etiology reported did not differ between the three groups except for leg injury (P = .002). The most prevalent comorbidity was hypertension (47.5%), followed by diabetes (43.6%). When comparing the three groups, no statistically significant difference was noted regarding comorbidities.
A total of 81 (16.4%) patients were on aspirin, and 31 (6.3%) patients were on P2Y12 inhibitors. Different types and approaches of parenteral anticoagulation were used; for example, 253 (51.3%) patients were on enoxaparin, and 79 (16.0%) patients were on heparin, while 52 (10.6%) patients received heparin followed by enoxaparin or enoxaparin followed by heparin. Direct oral anticoagulants (DOACs) including apixaban, rivaroxaban, or dabigatran were used; apixaban was used the most frequently, accounting for 49% of the patients. Moreover, warfarin was used by 90 patients, accounting for 18.3% of the sample. The use of warfarin differed among the three groups, as shown by a P-value of .028. The clinical characteristics, VTE etiologies, comorbidities, risk factors, and anticoagulants used are shown in Table 1.
Clinical Characteristics, Etiology, Comorbidities, Risk Factors, and Medications Used among DVT Patients.
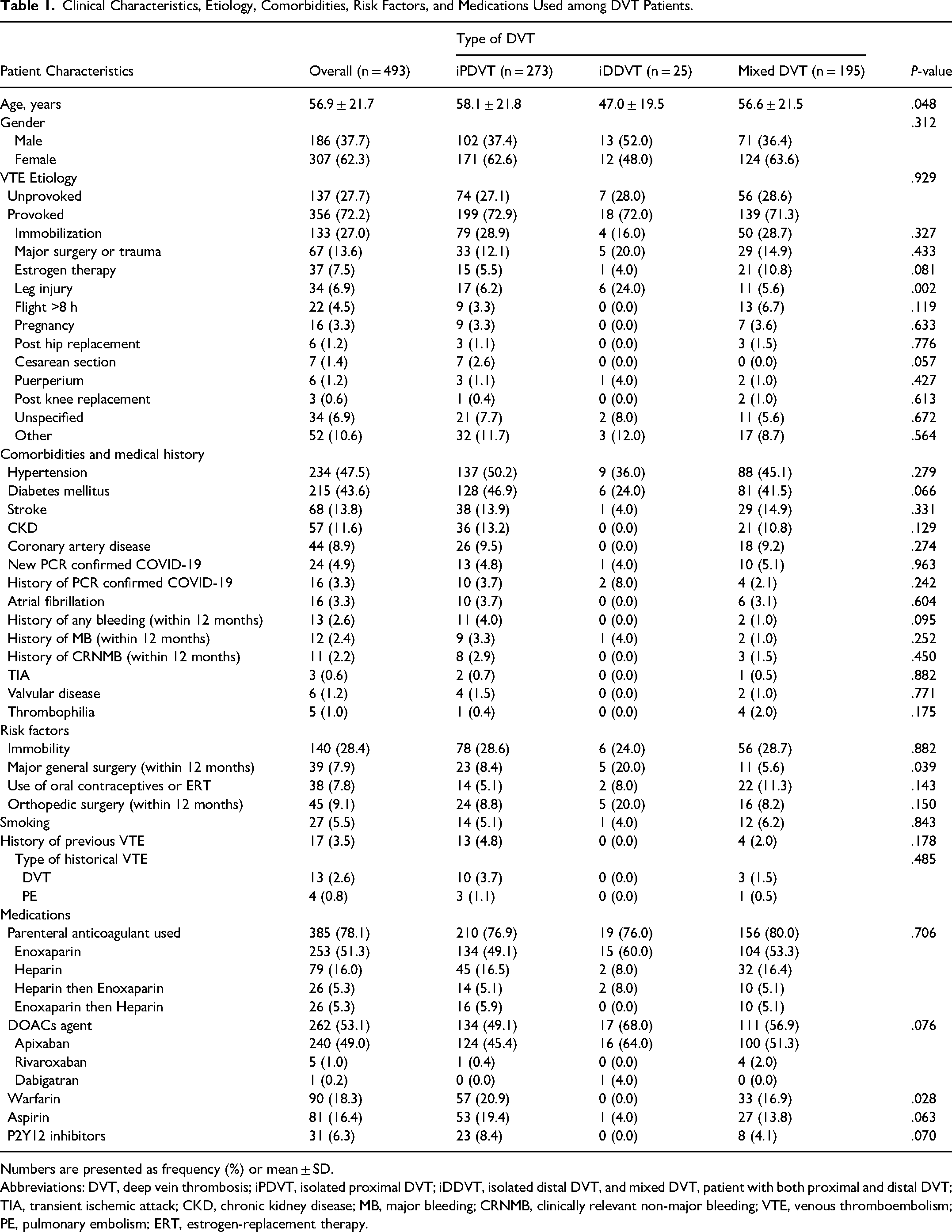
Numbers are presented as frequency (%) or mean ± SD.
Abbreviations: DVT, deep vein thrombosis; iPDVT, isolated proximal DVT; iDDVT, isolated distal DVT, and mixed DVT, patient with both proximal and distal DVT; TIA, transient ischemic attack; CKD, chronic kidney disease; MB, major bleeding; CRNMB, clinically relevant non-major bleeding; VTE, venous thromboembolism; PE, pulmonary embolism; ERT, estrogen-replacement therapy.
Before the initiation of an anticoagulant, the study population had a mean serum creatinine level of 92.7 ± 81.1 umol/L, while the mean eGFR was 91.0 ± 38.0 mL/min/1.73 m2. The mean Hgb was 120.3 ± 25.1 g/L at admission and 118.6 ± 25.0 g/dL on the day of DVT diagnosis. Detailed information about the lab values across the three groups are shown in Table 2.
Laboratory Values Before Anticoagulant Initiation.

Numbers are presented as mean ± SD.
Abbreviations: DVT, deep vein thrombosis; iPDVT, isolated proximal DVT; iDDVT, isolated distal DVT, mixed DVT, patient with both proximal and distal DVT; Scr, serum creatinine; eGFR, estimated glomerular filtration rate. Hgb, hemoglobin.
Clinical Outcomes
Data regarding clinical outcomes (DVT recurrence, major bleeding events, rehospitalization for DVT-related causes, and death from DVT during index hospitalization) are presented in detail in Table 3.
Clinical Outcomes Observed among DVT Patients.
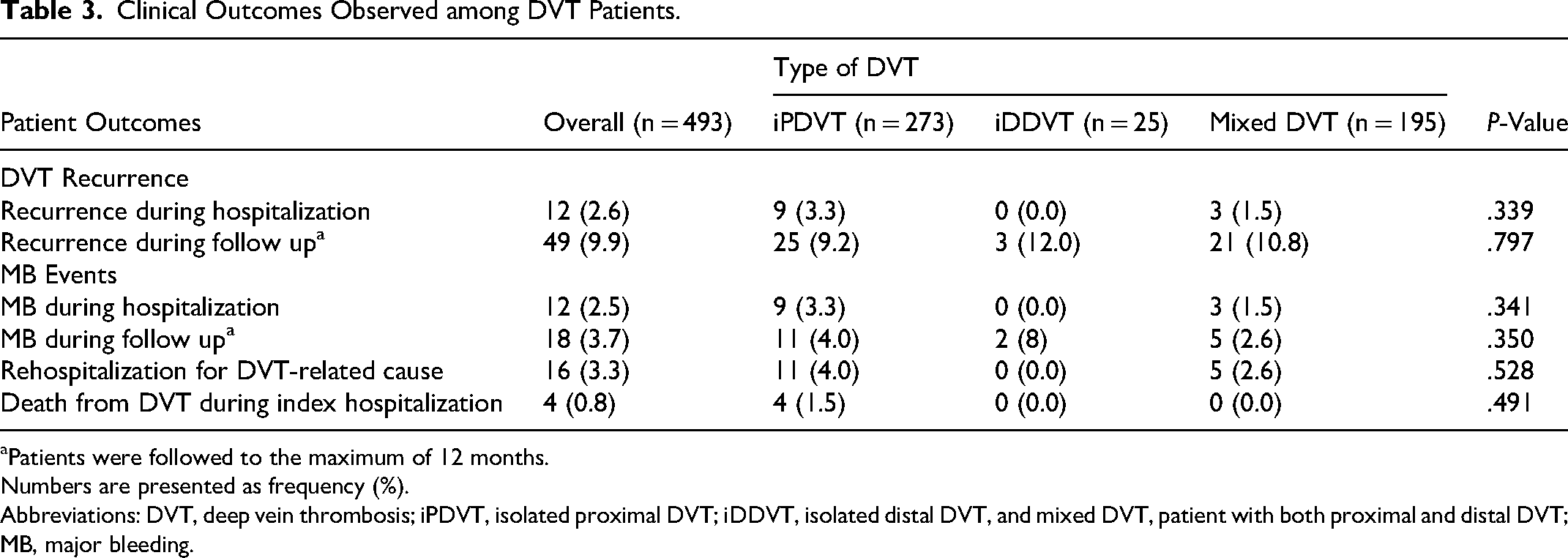
Patients were followed to the maximum of 12 months.
Numbers are presented as frequency (%).
Abbreviations: DVT, deep vein thrombosis; iPDVT, isolated proximal DVT; iDDVT, isolated distal DVT, and mixed DVT, patient with both proximal and distal DVT; MB, major bleeding.
DVT Recurrence
Among the study participants, 12 patients (2.6%) experienced a recurrent DVT event during the index hospitalization, including 9 (3.3%) and 3 (1.5%) patients from the iPDVT and mixed DVT groups, respectively. Likewise, during the follow-up period of up to 12 months, a total of 49 patients (9.9%) had a recurrent DVT event; among these patients, 25 (9.2%) were in the iPDVT group, 3 (12.0%) were in the iDDVT group, and 21 (10.8%) were in the mixed DVT group. There was no statistically significant difference between the study groups in terms of DVT recurrence.
MB Events
The occurrence of MB events during hospitalization was observed in 12 (2.5%) patients; 9 (3.3%) and 3 (1.5%) were in the iPDVT and mixed DVT groups, respectively. During the 12-month follow-up period, 18 (3.7%) patients experienced MB events, encompassing 11 (4%) patients from the iPDVT group, 2 (8%) patients from the iDDVT group, and 5 (2.6%) patients from the mixed DVT group. Similar to the recurrent DVT outcome, the findings suggest no statistically significant difference between the groups.
Re-Hospitalization for DVT-Related Causes
Within a 12-month follow-up, 16 (3.3%) patients, 11 (4.0%) patients from the iPDVT group and 5 (2.6%) patients from the mixed DVT group, were re-hospitalized for DVT-related causes, with no significant difference between the groups.
Death from DVT During the Index Hospitalization
During the index hospitalization, death attributed to DVT was reported in four patients (0.8%), all from the iPDVT group, with no statistically significant differences between groups.
Discussion
This study investigated differences in baseline characteristics, risk factors, and clinical outcomes for patients with different types of DVT, namely iPDVT, iDDVT, and mixed DVT. The distribution of DVT types in our cohort was consistent with previous research showing that iPDVT is more common than iDDVT.6–8 However, there is a large variation in the incidence of iDDVT in the literature which could be attributed to the use of different imaging techniques in institutions and variations in diagnostic criteria and protocols which focus on diagnosing and treating proximal DVT, which can cause iDDVT to be under-reported. 9 In our analysis, leg injury was significantly higher in patients with iDDVT. This is consistent with a study that showed injuries in the leg were associated with a greater risk of developing iDDVT. 10 Major general surgery is a known risk factor for all DVT subtypes due to immobility, changes in blood flow, and vascular injury. 11 Notably, it was found that general surgery was significantly higher in patients with the iDDVT subtype compared to the other groups. The absence of significant associations with other triggering factors, such as estrogen therapy, pregnancy, and travel, could potentially be attributed to the limited number of cases within these categories. The prevalence of comorbidities, such as atrial fibrillation, coronary artery disease, and hypertension, was also assessed, with no significant differences found among different types of DVT. Although these comorbidities and triggering factors are important factors in overall DVT management. 3 our findings suggest that these do not significantly influence the type of DVT event.
In the cohort overall, the use of a DOAC was more common than warfarin, which is justified given the updated 2021 CHEST guidelines which recommend the use of DOACs over warfarin for PE or DVT of the leg. 12 Furthermore, the recent literature supports the use of DOACs over warfarin due to factors such as convenience, the lack of need for parenteral anticoagulation for agents like apixaban and rivaroxaban, no monitoring requirement monitoring, and fewer drug–drug interactions. 13 DOACs have been established to have benefits over warfarin in the long-term treatment of symptomatic VTE disorders like DVT and PE. 14 Comparing the use of warfarin and DOACs in different subtypes of DVT, the data showed interesting trends. It was noted that among patients with iPDVT compared to mixed DVT cases, more patients were on warfarin, while none of the patients with iDDVT received warfarin. This indicates a significant difference in the use of warfarin across different types of DVT. Conversely, the data revealed similar rates of DOAC usage across the three subtypes.
Previous research by Galanaud et al indicated that patients with iDDVT had similar rates of adverse outcomes (death, VTE recurrence, or major bleeding) compared to those with iPDVT. 15 However, the study was conducted in patients with cancer, whom we excluded from our study. In addition, Hansson et al found no significant difference in recurrence rates during follow-up between patients with DVT in the upper or lower extremities; however, proximal DVT was found to be an independent predictor for VTE recurrence. 16 This contrasts with our findings, which suggest that there was no statistically significant difference in the rate of recurrence among patients with iPDVT, iDDVT, or mixed DVT. Similarly, the rates of MB events, re-hospitalization for VTE-related causes, and death from DVT during the index hospitalization across different types of DVT indicate that for these patients, management and outcomes were generally comparable. Further research may be warranted to explore potential factors influencing these outcomes and to optimize care and treatment strategies for patients with different types of DVT.
There are some limitations to our study, including its retrospective design and small sample size. Furthermore, we excluded patients with cancer; while this could be considered a strength given the unique characteristics of the cancer population, this exclusion could limit the generalizability of our findings to clinical practice. Despite these limitations, our study evaluated DVT recurrence, MB events, mortality, and hospitalizations from VTE-related causes across three subtypes of lower extremity DVT and provided some data on these outcomes in iPDVT, iDDVT, and mixed DVT. More studies using real-world data should aim to collect and analyze data on long-term outcomes, such as mortality and recurrence rates, to better understand the implications of different types of DVT. Moreover, prospective studies could provide more robust evidence about the efficacy of various treatment strategies in different types of DVT.
Conclusion
Baseline characteristics were not significantly linked to the risk of developing a specific type of lower extremity DVT. Likewise, the long-term outcomes examined, mortality and the recurrence rate, were not increased in one specific type compared to another. However, among different DVT etiologies, leg injury was a prevalent characteristic among patients with iDDVT. As for the treatment approaches, DOACs were the most commonly used therapy in these patients, while warfarin was not used in patients with iDDVT. Larger prospective studies with a long duration of follow-up are still warranted to prove the absence of a link between different etiologies or baseline characteristics and a specific type of DVT, as well as any association between different types of DVT and the outcome of DVT management.
Footnotes
Acknowledgments
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2024R418), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. The authors would like to extend their appreciation to King Saud University for funding this work through the Researcher Supporting Project (RSP2025R77), King Saud University, Riyadh, Saudi Arabia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author (OAA) received funding from the Research Supporting Project (RSP2025R77), King Saud University, Riyadh, Saudi Arabia to support the publication of this article. The funding agency played no role in designing the study, analyzing and interpreting the data, or writing the manuscript.
Ethics Approval
This study obtained Institutional Review Board approval from the King Abdullah International Medical Research Center (SP22R/234/10).