
Abstract
Malignancy, including testicular tumors, significantly increases the risk of venous thromboembolism (VTE). In this study, we search for predictors that may help identify subgroups of patients at higher risk of VTE. Patients with confirmed diagnosis of testicular germ cell tumor and proven VTE were identified. Clinical and pathological features possibly associated with VTE were reviewed. A total of 322 patients, median age (range) 31 (18-76) years were identified. Tumors were mostly non-seminoma (n = 194, 60.2%), node-positive (n = 130, 40.4%) and 58 (18.0%) had metastatic disease at diagnosis. Venous thromboembolism were confirmed in 27 (8.4%) patients; however, rates were significantly higher (P < 0.001) in patients with node-positive (18.5%), metastatic disease (22.4%), and those with high lactate dehydrogenase (LDH) (21.3%). Rates were also significantly higher among those who received multiple lines of chemotherapy (27.5%) compared to those who received one line (13.8%) or none (<1.0%), P < 0.001. Patients with testicular tumors and high tumor burden, including nodal involvement, high LDH or metastatic disease, and those treated with multiple lines of chemotherapy have significantly higher rates of VTE.
Background
Testicular germ cell tumors are not commonly encountered; however, they are the most common malignancies affecting adolescents and young adults and their incidence is increasing. 1,2 Even in advanced-stage disease, testicular tumors are considered potentially curable and mostly using relatively old and widely available chemotherapy regimens. 3
Malignancy, including testicular cancer, significantly increases the risk of both deep vein thrombosis (DVT) and pulmonary embolism (PE), both referred to as venous thromboembolism (VTE). 4 Majority of patients with testicular cancer are treated in ambulatory settings where thromboprophylaxis is not routinely offered. 5
Most of patients with germ cell tumors are young without much of comorbidities and this should lower their risk for VTE. However, cancer itself and cisplatin; a chemotherapeutic agent that is routinely used in the treatment of testicular cancer, markedly increase their risk for VTE. In one study that involved 179 patients with germ cell cancer, 8.4% developed thromboembolic complications. 6 In another study that enrolled 153 patients undergoing cisplatin-based chemotherapy, 26 (17%) developed VTE. 7
Thrombosis in cancer patients is not without major complications. Post-phlebetic (thrombotic) syndrome with its associated poor mobility and intractable pain may negatively affect their quality of life. 8 Both the clot and its associated complications may interrupt or delay surgical interventions or the administration of chemotherapy in a highly curable disease, thus negatively affecting treatment outcomes. 9
Risk assessment models (RAM) grouped several risk factors related to the patient, the tumor and its therapy into models attempting to identify subgroups of patients with high-risk to justify thromboprophylaxis in ambulatory settings. 10 Testicular cancer was among the high-risk tumors in the highly cited Khorana RAM. 11
Cisplatin, a key chemotherapeutic agent in the well known BEP (Bleomycin, Etoposide and Cisplatin) regimen commonly used to treat testicular cancer. 12,13 Several studies had documented the high rates of thromboembolic events, both arterial and venous, among patients with different cancers treated with cisplatin-based regimen. 14,15 In one study, 18% of 932 patients treated with cisplatin-based regimens for various kinds of cancers had thromboembolic events. 16 Such findings were supported by a meta-analysis that involved more than 8000 patients with various solid tumors treated with different chemotherapy regimens. Patients treated with cisplatin-based chemotherapy had a significantly higher risk of VTEs (Relative Risk [RR], 1.67; 95% CI, 1.25 to 2.23; P = 0.01). 17 In this study, we search for clinical and pathological predictors that may help identify subgroups of patients with testicular cancer at higher risk for VTE to justify thromboprophylaxis.
Materials and Methods
Patients with pathologically confirmed diagnosis of testicular germ cell tumors; diagnosed, treated and followed in our institution, a tertiary cancer center, were retrospectively analyzed for a diagnosis of radiologically proven VTE. Clinical and pathological features known to increase the risk of VTE were reviewed.
Thrombosis was considered chemotherapy-related if diagnosed within 4 weeks after the last administration. Deep venous thrombosis was diagnosed by Doppler ultrasound, while PE was diagnosed by CT angiogram. Routine screening for VTE among asymptomatic patients was not performed.
In general, differences in proportions were tested with χ2 test or Fisher exact test while differences in continuous variables were tested with t-test or non-parametric test, depending on the assumption required for each test. Adjusted and unadjusted odds ratio was calculated by using logistic regression model. A significance criterion of P < 0.05 was used in the analysis. All analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC).
The research was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki). Because of the retrospective nature of the study and the lack of personal details of participants that compromise anonymity, consent was waived and the study was approved by King Hussein Cancer Center Institutional Review Board (IRB).
Results
Between 2006 and 2016, a total of 322 patients with testicular cancer; median age (range) 31 (18-76) years were identified. Pathological features include non-seminoma in 194 (60.2%), tumors larger than T1 in 125 (38.8%), node-positive in 130 (40.4%) and metastatic disease in 58 (18.0%).
Among the whole group, VTE were confirmed in 27 (8.4%) patients; 21 (77.8%) were DVT involving mostly the lower extremities, 3 (11.1%) were PE (one incidental; all were mild, non-obstructive), while one case each involved renal, splenic and mesenteric veins. Rates were higher among patients with node-positive compared to those with node negative (18.5% versus 1.6%, P < 0.001), in those with metastatic versus non-metastatic disease (22.4% versus 5.3%, P < 0.001) and in patients with high LDH (>280 U/L) (21.3% versus 4.5%, P < 0.001). Additionally, patients older than 30 years (n = 172) had higher rate (11.6%) compared to 4.7% among younger ones, P = 0.025. Tumor histology, seminoma versus non-seminoma, tumor size, smoking and overweight were not associated with higher rates of VTE, Table 1.
Patients’ Characteristics.
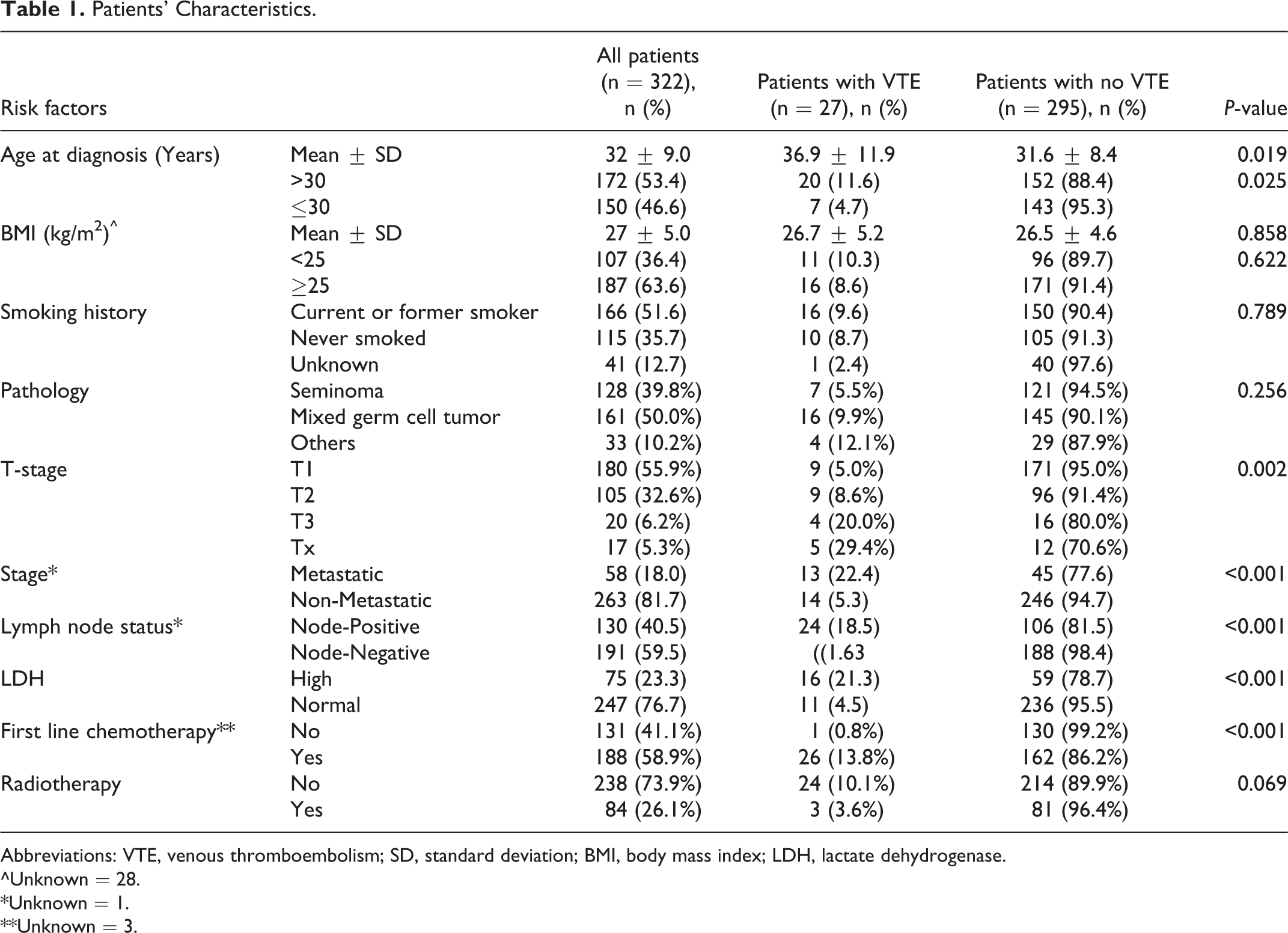
Abbreviations: VTE, venous thromboembolism; SD, standard deviation; BMI, body mass index; LDH, lactate dehydrogenase.
^Unknown = 28.
*Unknown = 1.
**Unknown = 3.
Only one of 131 patients who never received any chemotherapy had a confirmed diagnosis of VTE compared to 13.8% among 188 patients who received one line and 27.5% among 40 patients who received multiple lines of chemotherapy, P < 0.001. On the other hand, patients treated with radiation therapy (n = 84) had lower rate of VTE (n = 3, 3.6%) compared to 24 (10.1%) episodes of VTE among 238 who did not receive radiation, P = 0.069, Figure 1.

VTE rates according to treatment. Venous thromboembolism (VTE) rates according to treatment given. Patients who received multiple lines of chemotherapy had significantly higher rate of VTE compared to those who had one line or none. Patient who had radiation therapy had lower VTE rate, but the difference was not significant.
To better estimate the risk of VTE in a unified group of patients, we also separately analyzed the 188 patients who were treated with single line of cisplatin-based regimen (BEP) and had a VTE rate of 13.8%. Similar to the whole cohort, VTE rates were also higher among patients with node-positive (20.7% versus 2.8%, P < 0.001), metastatic disease (23.6% versus 9.8%, P = 0.013), those with high LDH (25.8% versus 7.9%, P = 0.001), and patients older than 30 years (20.6 versus 6.6%, P = 0.005. Effect of other variables like smoking, tumor pathology, tumor size and overweight are detailed in Table 2. In multivariate analysis, only Age (>30 vs. ≤30); [odds ratio (OR) = 2.91, 95% Confidence Interval (CI):1.11-7.64, P = 0.0296], and nodal involvement (OR = 4.57, 95% CI: 1.14-18.32, P = 0.0321) were significant, Table 3. Similar conclusions were reached on multivariate analysis for the subgroup of patients who had chemotherapy (Table 3).
Unadjusted Odds Ratio for Venous Thromboembolism (VTE) Among All Patients and Chemotherapy Subgroup.^

Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; LDH, lactate dehydrogenase.
^Probability modeled is VTE = “Yes.”
*Reference.
Adjusted Odds Ratio for Venous Thromboembolism (VTE) Among All Patients and Chemotherapy Subgroup.^
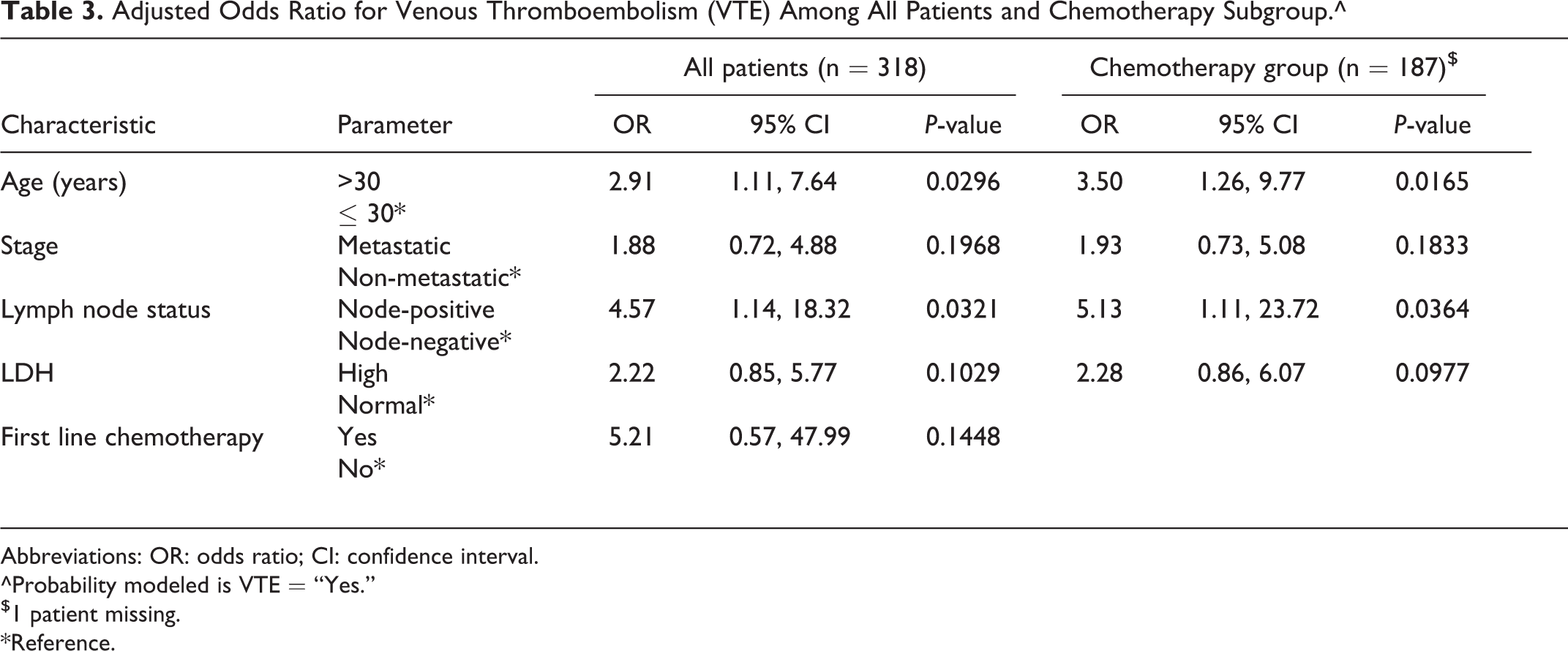
Abbreviations: OR: odds ratio; CI: confidence interval.
^Probability modeled is VTE = “Yes.”
$1 patient missing.
*Reference.
We also looked at the LDH levels in patients with or without VTE. The mean (95% CI) level of LDH among those with VTE was 469 (308, 630) U/L compared to 309 (272, 346) unit/L among those with no VTE, P = 0.0024. Similar trend was also observed in the smaller group of patients treated with one line of chemotherapy; mean LDH was 478 U/L (311, 645) versus 374 (315, 433) U/L, P = 0.058.
Because the majority (n = 149, 93.7%) of patients at time of chemotherapy had intermediate Khorana risk score and only 5 (3.1%) were at high risk, the application of Khorana RAM was not successful in segregating patients into different risk categories.
Discussion
Testicular cancer affects adolescents and younger adults and is highly curable even when diagnosed with advanced-stage disease; thus, management and prevention of complications associated with the cancer itself or its therapy is of paramount importance. 18,19
Given their young age and the absence of comorbidities, most of the contributing factors for thrombosis in patients with testicular germ cell tumors are related to the tumor itself and its therapy; both are non-modifiable factors. 7,20 However, underlying thrombophilic disorders could not be ruled out as contributing factors. Workup for such disorders is not routinely performed by treating oncologists. In our cohort, only few patients were tested and all were negative.
Our rates of VTE are consistent with previously published studies. 6,7 However, the relatively large group of patients in our study, allowed us to have a closer look into a unified group of 188 patients, all treated with a single line of cisplatin-based chemotherapy (BEP) and achieved a response without the need for more lines of salvage chemotherapy. A thromboembolic rate of 13.8% encountered in such young patients, treated in ambulatory setting, is relatively high and worth preventive measures. Even in this subgroup, who are not heavily treated, significantly higher rates of VTE were noted among patients with positive lymph nodes, metastatic disease and high LDH. Such factors are not incorporated in the widely cited Khorana RAM. Interesting enough, patients who received radiation therapy had a lower VTE rate (3.6%) compared to 10.1% among those who never had radiation therapy. Such finding can be explained by the fact that patients with early-stage disease are more likely be treated with radiation therapy and are potential cured, while those with more advanced-stage disease are not offered radiation and are usually treated, when indicated, by chemotherapy.
The association between high LDH and the risk of thrombosis in testicular germ cell tumors is interesting. In both cohorts, the whole group and those who received one line of chemotherapy, high LDH was associated with significantly higher rates of VTE. Traditionally, LDH is considered a surrogate marker of disease activity and is considered a tumor marker in testicular germ cell tumor.
Because majority of our patients had an intermediate risk score, we were not able to use the Khorana RAM in our patients’ population. Several other studies had questioned the utilization of Khorana RAM in clinical practice especially so when studied in a single tumor site, including testicular cancers. 7,21 –24
Patients with testicular germ cell tumors are young but have other special features that can be used to derive a specific risk assessment model taking into consideration patient’s age, disease stage, lymph node involvement and LDH. In a multi-center observational retrospective study, 255 patients with testicular germ cell tumors treated with platinum-based chemotherapy, 49 (19%) patients experienced a VTE. In multivariate analysis, clinical stage ≥IIC disease, elevated serum LDH, febrile neutropenia and central venous access were all associated with higher risk. 25 Our data suggests that salvage chemotherapy beyond the first line should also be considered among other contributing factors. However, larger modeling studies will be able to find if such variable is an independent factor or a reflection of other contributing factors.
Several previously published studies went even beyond VTE risk stratification to offer prophylaxis based on preset risk criteria. In one study, rates of both arterial and venous thrombosis dropped by 50% following the implementation of thromboprophylaxis for patients treated with cisplatin-base regimen. However, the study was not randomized and used historical control for comparison. 26 In another study, extended out-of-hospital prophylaxis with low molecular weight heparin (LMWH) was given from day-1 of chemotherapy until 3 weeks after the last cycle of chemotherapy to 45 out of 93 patients, while the other 48 were offered prophylaxis during their hospitalization only. Unfortunately, extended out of hospital prophylaxis failed to lower this risk: (extended: 26.7 vs. limited: 20.8%, P = 0.5). 27
Conclusion
Our study confirms the high rate of venous thromboembolism in patients with testicular germ cell tumors. Age >30 years, lymph node involvement, advanced-stage disease, high LDH and the need for more than one line of chemotherapy are all important factors that may increase the risk of VTE. The retrospective nature of our study could be a limiting factor that preclude solid conclusions. However, we believe that data exists to justify efforts to derive a VTE risk assessment model designed specifically for patients with testicular germ cell tumor.
Footnotes
Abbreviations
BEP: Bleomycin, Etoposide and Cisplatin; BMI: Body Mass Index; IRB: Institutional Review Board; LDH: Lactate Dehydrogenase; LMWH: Low Molecular Weight Heparin; OR: Odds Ratio; RAM: Risk Assessment Models; RR: Relative Risk; VTE: Venous Thromboembolism.
Authors’ Note
Conception and design: HA. Collection and assembly of data: FT, ZO, OS, AF, AA, HQ, AN, YH. Data analysis and interpretation: HA, RA, SS, AT. Manuscript Writing: All authors. Final approval of manuscript: All authors. Accountable for all aspects of the work: All authors. Consent to participate: Because of the retrospective nature of the study and the lack of personal details of participants that compromise anonymity, consent was waived. Consent for publication: Given the retrospective nature of the study and the lack of personal details of participants that compromise anonymity, consent for publication was not sought from the participants, but obtained from the hospital administration. Ethics approval: This research was done in accordance with the ethical standards of the institutional and national research standards and with the 1964 Helsinki declaration and its later amendments. The study was approved by King Hussein Cancer Center Institutional Review Board (IRB). Availability of data and material: Data will be made available, as per the Journal and publisher rules and regulations, from the corresponding author on reasonable request. Prior Presentation: The paper was presented in-part-at the International Society of Thrombosis and Hemostasis (ISTH) annual meeting, July-2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.